

Foot pain is one of the most common musculoskeletal complaints in adults, affecting people who spend long hours standing, walking, or exercising. The foot is a highly complex structure with 26 bones, dozens of joints, and a dense network of ligaments, tendons, and nerves. Even small changes in load, footwear, or daily habits can trigger pain, stiffness, or swelling.
Most cases of foot pain come from overuse, poor footwear, or biomechanical issues such as flat feet or high arches. But pain can also signal inflammation of the plantar fascia, irritation of a nerve, arthritis, or even a stress fracture. Understanding where the pain appears — heel, arch, toes, or forefoot — is the first step toward identifying the underlying cause.
This article breaks down 33 most common causes of foot pain, explains their typical symptoms, and shows how to recognize them early. You’ll also learn when home treatment is enough, when to see a specialist, and which exercises can help reduce pain and improve foot mechanics.
Key Clinical Points – Foot Pain by Location
- Heel pain most often comes from conditions like plantar fasciitis or Achilles tendon irritation. Pain may appear under the heel or at the back of the heel and is frequently worse with first steps or uphill walking.
- Top of foot pain usually reflects midfoot or ankle joint irritation, tendon overload, or early stress reactions in the metatarsals. Patients describe aching or sharp discomfort across the dorsum of the foot that increases with walking or standing.
- Lateral foot pain (outer edge) commonly arises from overload of the 5th metatarsal region, peroneal tendons, or the cuboid area. Symptoms often worsen with side‑to‑side movements or uneven terrain.
- Medial foot pain (inner edge) is often linked to tibialis posterior strain, navicular overload, or medial midfoot joint irritation. Pain typically follows the inner arch or inner ankle, especially during prolonged walking.
- Bottom of foot pain includes heel pain, arch discomfort, and forefoot pain. Common sources are plantar fascia overload, arch strain from flatfoot mechanics, and forefoot overload conditions such as metatarsalgia or neuroma.
- Big toe pain frequently stems from joint stiffness, sesamoid irritation, gout flares, or bunion‑related mechanical changes. Pain often increases during push‑off or when bending the toe.
- Lesser toe pain (2nd–5th toes) often reflects capsular irritation, plantar plate strain, toe deformities, or nerve irritation between the toes. Symptoms may include aching, burning, or pain during push‑off.
- Red flags requiring urgent evaluation include severe swelling or spreading redness, inability to bear weight, night pain, sudden big‑toe inflammation, persistent numbness or burning, and trauma with visible deformity.
Epidemiology: How Common Is Foot Pain?
Foot pain is extremely common in adults, affecting anywhere from 10% to 35% of the population depending on age group. Prevalence rises steadily with age, and studies show that one in three older adults experiences persistent foot pain that affects daily activities, balance, and walking tolerance.
Several factors significantly increase the risk of developing foot pain. Obesity is one of the strongest predictors — individuals with higher body weight are about 60% more likely to develop foot pain due to increased mechanical load on the foot’s joints, ligaments, and plantar fascia. Women also report foot pain more frequently than men, with a 40% higher prevalence, partly due to narrow footwear and high‑heeled shoes that increase forefoot pressure.
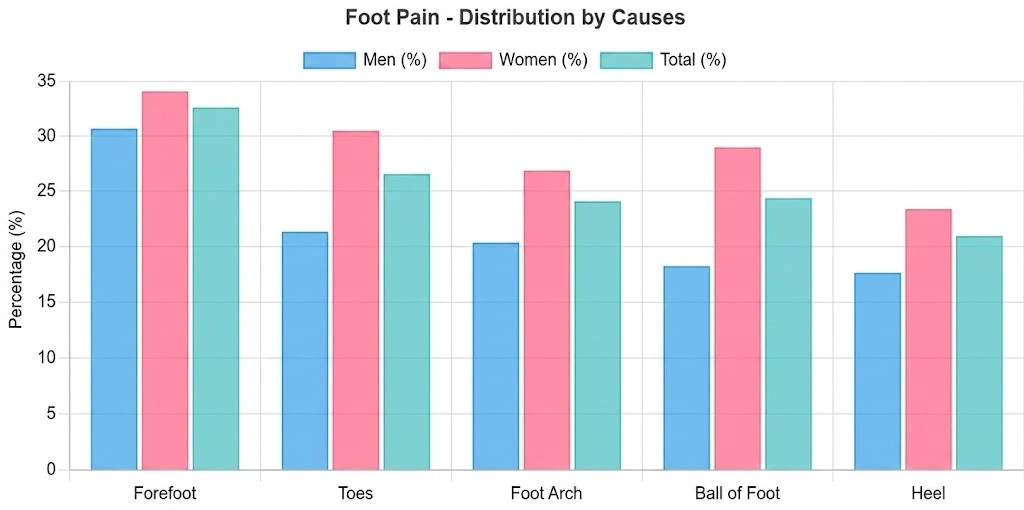
Foot pain often coexists with pain in other weight‑bearing joints. People with hip or knee osteoarthritis frequently report foot discomfort as well, likely due to altered gait mechanics and compensatory loading patterns. The distribution of pain across the foot is broad: heel, arch, midfoot, forefoot, and toes are all commonly affected.
The graph below illustrates the percentage distribution of foot pain by region, showing that discomfort is spread fairly evenly across all anatomical zones. This pattern underscores how varied and multifactorial foot pain truly is.
Foot Anatomy: A Quick Overview Before We Explore the Causes
The human foot is a highly complex structure made up of 26 bones, 33 joints, and more than 100 muscles, tendons, and ligaments. Together, these tissues allow the foot to support body weight, absorb impact, and transfer forces during walking, running, and standing. Because so many structures work together, even small changes in load or mechanics can lead to pain.
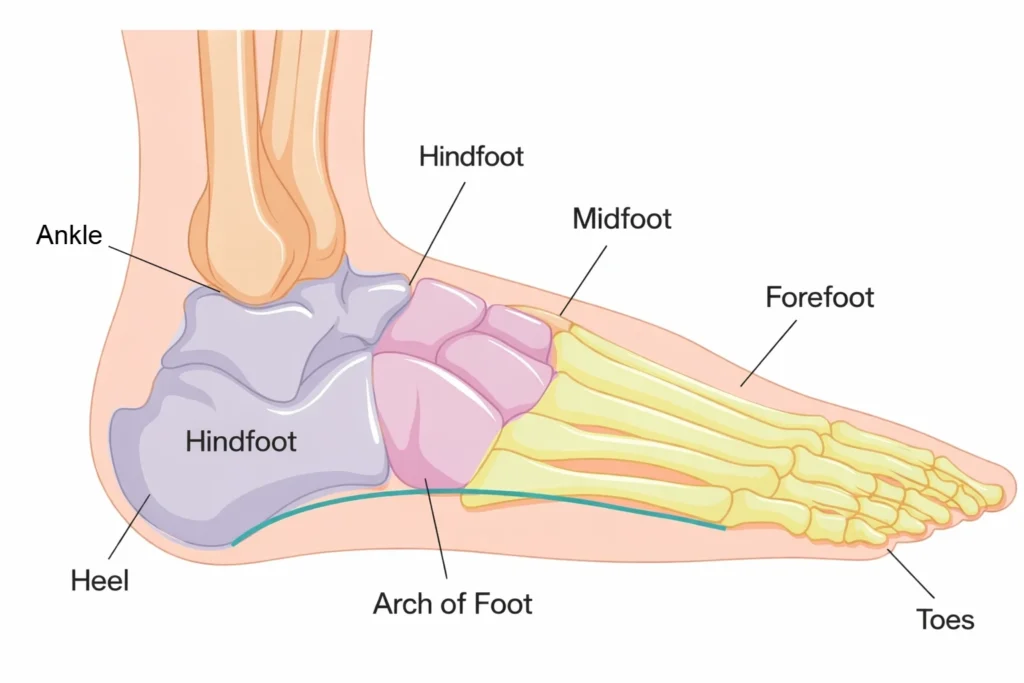
Anatomically, the foot is divided into three main regions:
- Forefoot — toes and metatarsal heads
- Midfoot — the arch of the foot
- Hindfoot — heel and ankle
The arch acts as a natural shock absorber, the heel carries most of the load during heel strike, and the toes help maintain balance and generate push‑off during gait. Each region has distinct anatomical structures — and each can produce pain for different reasons.
Understanding where the pain occurs is often the first clue to identifying the underlying cause. Heel pain, arch pain, midfoot stiffness, forefoot burning, or toe discomfort each point toward different conditions.
In the next sections, we’ll walk through each region of the foot and explain what typically causes pain in that specific area — helping readers quickly connect their symptoms with the most likely source.
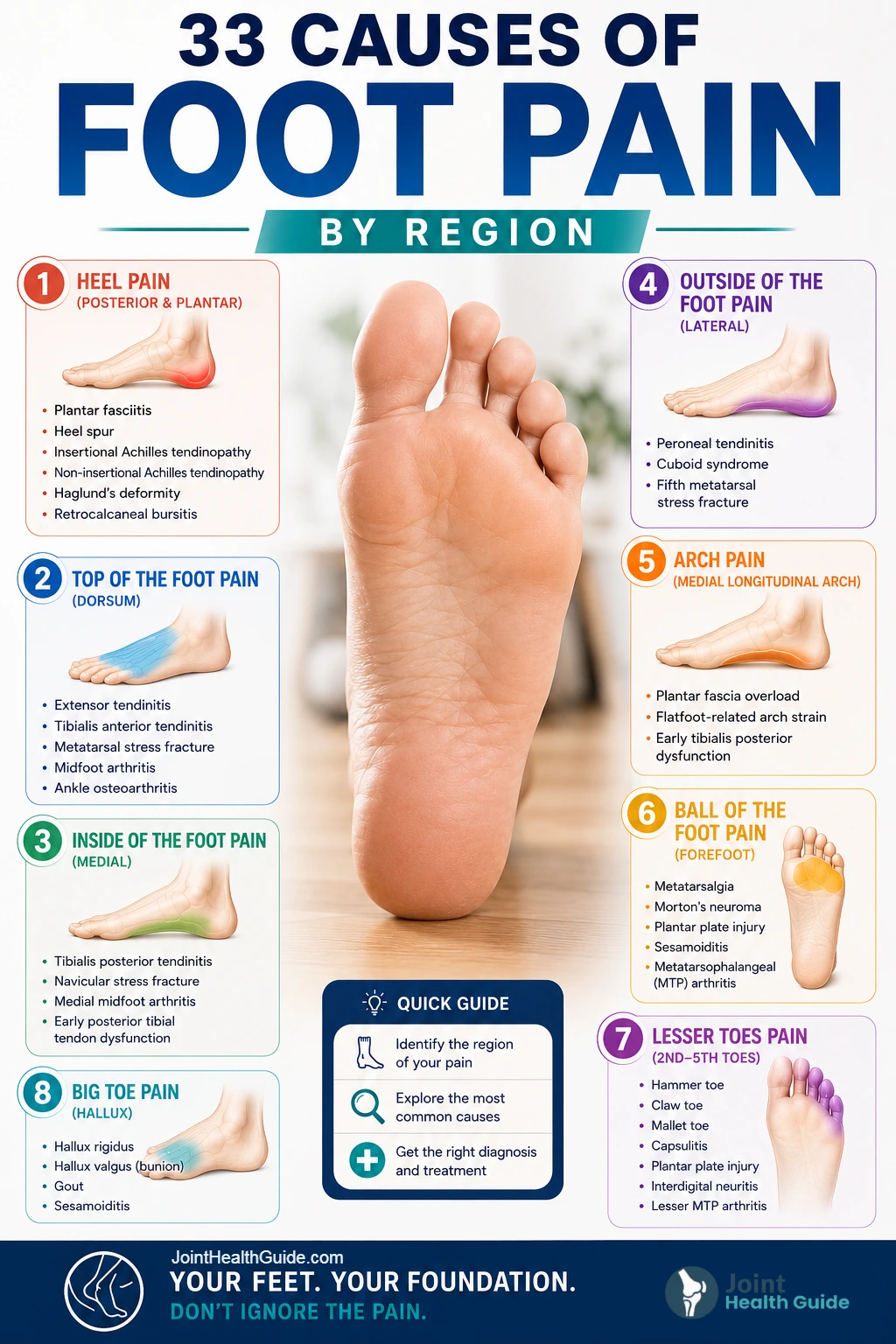
33 Causes of Foot Pain by Region
The table below systematically summarizes the 33 most common causes of foot pain by anatomical location, making it easier to identify the most likely source of your symptoms.
| Foot Region | Most Common Causes | Typical Pain Characteristics |
|---|---|---|
| Heel (Posterior & Plantar) |
Plantar fasciitis Heel spur Insertional Achilles tendinopathy Non-insertional Achilles tendinopathy Haglund’s deformity Retrocalcaneal bursitis |
Pain with the first steps in the morning, tenderness beneath or behind the heel, pain during walking, running, or wearing rigid shoes. |
| Top of the Foot (Dorsum) |
Extensor tendinitis Tibialis anterior tendinitis Metatarsal stress fracture Midfoot arthritis Ankle osteoarthritis |
Pain across the top of the foot that worsens with walking, running, climbing stairs, or pressure from shoelaces. |
| Inside of the Foot (Medial) |
Tibialis posterior tendinitis Navicular stress fracture Medial midfoot arthritis Early posterior tibial tendon dysfunction |
Aching pain along the inner arch or ankle, often aggravated by prolonged walking, standing, or excessive pronation. |
| Outside of the Foot (Lateral) |
Peroneal tendinitis Cuboid syndrome Fifth metatarsal stress fracture |
Pain along the outer edge of the foot, commonly aggravated by uneven surfaces, running, or side-to-side movements. |
| Arch (Medial Longitudinal Arch) |
Plantar fascia overload Flatfoot-related arch strain Early tibialis posterior dysfunction |
Pain and fatigue within the arch during prolonged standing, walking, or after increased physical activity. |
| Ball of the Foot (Forefoot) |
Metatarsalgia Morton’s neuroma Plantar plate injury Sesamoiditis Metatarsophalangeal (MTP) arthritis |
Burning, aching, or sharp pain beneath the metatarsal heads that increases during push-off, walking, or running. |
| Big Toe (Hallux) |
Hallux rigidus Hallux valgus (bunion) Gout Sesamoiditis |
Pain around the first MTP joint with stiffness, swelling, difficulty pushing off, or sudden severe inflammation. |
| Lesser Toes (2nd–5th Toes) |
Hammer toe Claw toe Mallet toe Capsulitis Plantar plate injury Interdigital neuritis Lesser MTP arthritis |
Localized toe pain, swelling, deformity, burning sensations, or discomfort during walking and shoe wear. |
Heel Pain
Heel pain is slightly more common in younger and physically active individuals. The location of pain often helps identify its cause:
- Pain at the back of the heel usually points to problems with the Achilles tendon.
- Pain on the underside of the heel is most often linked to plantar fasciitis.
Let’s look at the most common causes of heel pain.

1. Achilles Tendinopathy
Achilles tendinopathy can be insertional (where the tendon attaches to the heel bone) or non‑insertional (higher up along the tendon). Insertional tendinopathy causes pain directly at the heel, often aggravated by uphill walking or tight shoes. Non‑insertional tendinopathy affects the mid‑portion of the tendon and is common in runners.
Both forms involve micro‑tears and degeneration of tendon fibers, leading to stiffness and pain during activity. Early management includes load modification, eccentric exercises, and footwear adjustments.
2. Plantar Fasciitis
Plantar fasciitis is the most common cause of heel pain, especially in middle‑aged adults. Pain is sharp and stabbing and is usually worst with the first steps in the morning or after getting up from rest. As the fascia warms up, symptoms often ease.
The pain is located on the underside of the heel, slightly toward the medial side, right at the plantar fascia’s attachment to the heel bone. Many patients describe it as a “stone bruise” sensation under the heel.
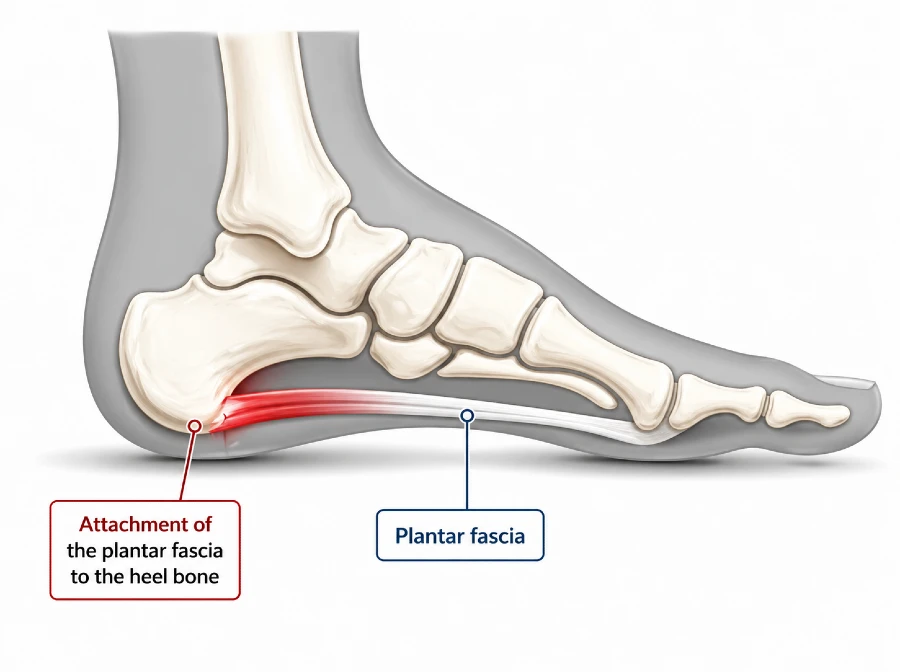
Plantar fasciitis develops due to micro‑tears and inflammation of the plantar fascia caused by overload, prolonged standing, poor footwear, or biomechanical factors.
Management includes stretching, orthotics, load reduction, and gradual return to activity.
If your heel pain feels sharp under the inside edge of the heel—especially with the first steps in the morning—you may be dealing with plantar fasciitis. Learn the key symptoms, causes, and treatment options in our full guide: Plantar Fasciitis.
3. Heel Spur
A heel spur is a small bony growth on the underside of the heel bone and is a common finding in older adults. Many people have a heel spur without any symptoms, and the spur itself often isn’t the source of pain.
When symptoms do appear, they usually present as localized tenderness or sharp pain on the bottom of the heel, especially during weight‑bearing. Discomfort tends to worsen with prolonged standing, walking barefoot on hard surfaces, or after periods of rest.

Heel spurs are frequently associated with chronic plantar fasciitis, and inflammation around the spur is what typically causes pain. Diagnosis is confirmed by X‑ray, and treatment follows the same principles as plantar fasciitis — reducing strain, improving foot mechanics, and calming inflammation.
If you have sharp, pinpoint pain under the heel, learn more in our full guide: Heel Spur.
4. Haglund’s Deformity
Haglund’s Deformity
Haglund’s deformity is a bony prominence at the back of the heel that irritates the Achilles insertion and surrounding soft tissues. It often causes redness, swelling, and pain when wearing rigid shoes, especially those with a hard heel counter. Chronic friction can lead to bursitis or additional tendon irritation.
Pain is felt on the posterior aspect of the heel, directly over the bony bump that rubs against footwear.
Treatment focuses on reducing pressure — soft‑back shoes, heel lifts, and physical therapy to calm inflammation.
If you have pain at the back of the heel that worsens with rigid shoes, learn more in our full guide: Haglund’s Deformity.
5. Retrocalcaneal Bursitis
Retrocalcaneal bursitis involves inflammation of the small bursa between the Achilles tendon and heel bone. It causes swelling and tenderness just above the heel, often triggered by repetitive friction or tight footwear. Rest, ice, and proper shoe fit are key to symptom relief.
Top of Foot Pain
The top of the foot — often called the dorsum of the foot — is the area between the ankle and the toes on the upper side of the foot. Patients commonly describe discomfort here using phrases such as “pain on the top of my foot,” “pain in top of foot,” “pain top of foot,” “top of the foot pain,” or “top of foot pain close to the ankle.”
Pain in this region is most often caused by:
- Ankle arthritis
- Midfoot arthritis
- Metatarsal stress fractures
- Extensor tendinitis
Arthritis is more common in older adults, while tendon inflammation and stress fractures typically occur in younger, active individuals — especially runners, hikers, and people who suddenly increase their training load.
In the next sections, we’ll break down each condition individually.

6. Ankle Arthritis
Ankle arthritis is a common cause of top of foot pain, especially in older adults. It develops when the cartilage in the ankle joint wears down, leading to inflammation, stiffness, and reduced joint mobility. Patients often describe symptoms as pain on the top of my foot, top of foot pain close to the ankle, or a deep aching sensation around the front of the ankle.
Pain typically worsens with walking, going downhill, or after longer periods of standing. Morning stiffness and swelling around the ankle joint are also frequent. As the joint becomes more irritated, even low‑impact activities can trigger discomfort.
Management focuses on load modification, supportive footwear, ankle‑strengthening exercises, and anti‑inflammatory strategies. More advanced cases may require bracing or medical interventions.
7. Midfoot Arthritis
Midfoot arthritis is a frequent cause of top of foot pain, especially in older adults. It develops when the small joints in the midfoot lose cartilage and become inflamed. Patients often describe symptoms as pain in top of foot that worsens with walking or standing.
People with high arches (pes cavus) are more prone to midfoot arthritis because the increased rigidity of the foot places extra stress on the midfoot joints. Pain typically intensifies during weight‑bearing, especially when pushing off the ground or walking uphill.
A common clinical finding is the presence of bony bumps on the top of the foot — dorsal osteophytes — which can rub against footwear and add to discomfort. Stiffness, swelling, and tenderness over the midfoot joints are also typical.
Management focuses on load reduction, supportive footwear, orthotics, and activity modification to decrease joint stress.
8. Metatarsal Stress Fracture
Metatarsal stress fractures are tiny cracks in the bone caused by overload or repetitive impact. They are common in high‑intensity activities such as running or jumping, but can also occur during everyday walking when bone strength is reduced — for example in osteoporosis.
Pain usually starts gradually, often as a mild, nagging discomfort on the top of the foot, and becomes more noticeable during or after activity. If loading continues, symptoms worsen and the stress fracture can progress into a complete fracture, which is why early recognition and activity reduction are essential.
9. Extensor Tendinitis of Foot
Extensor tendinitis involves irritation of the extensor hallucis longus (EHL), extensor digitorum longus (EDL), and sometimes the tibialis anterior tendon — all located on the top of the foot and front of the ankle. These tendons lift the toes and dorsiflex the foot during walking and running.
Pain appears on the top of the foot, often with swelling, and is typically most intense at the front crease of the ankle, just above the joint. Symptoms worsen with repetitive activities such as running, dancing, climbing stairs or ladders.
Tibialis anterior tendinitis produces similar discomfort but slightly more toward the front‑inner aspect of the ankle, where the tendon crosses the joint. Both conditions are frequently triggered by overly stiff footwear or shoelaces tightened too firmly, which increase pressure on the tendon group.
Lateral Foot Pain
Lateral foot pain refers to discomfort felt on the outside of the foot, often described by patients as pain on outside of foot, pain on the lateral side of the foot, or pain on the outer edge of the foot. This region includes the 5th metatarsal, cuboid, and the peroneal tendon complex — structures commonly involved in lateral-sided symptoms.
Pain in this region is most often caused by:
- 5th Metatarsal Stress Fracture — a frequent bony cause of lateral foot pain, typically worsening with weight‑bearing.
- Peroneal Tendinitis — inflammation of the peroneal tendons that stabilize the outer foot, often aggravated by uneven surfaces.
- Cuboid Syndrome — irritation or subtle subluxation of the cuboid bone, commonly triggered by repetitive lateral movements.
Stress fractures are more common in active individuals, while tendon irritation often develops with repetitive side‑to‑side loading or inappropriate footwear. Cuboid syndrome frequently appears after overuse or sudden changes in activity.
In the next sections, we’ll break down each condition individually.

10. 5th Metatarsal Stress Fracture
A 5th metatarsal stress fracture is a small crack in the outer metatarsal bone caused by repetitive loading. Pain is felt on the outside of the foot, often worsening with running, jumping, or prolonged walking. Localized tenderness over the 5th metatarsal shaft is typical, and symptoms gradually intensify if activity continues.
11. Peroneal Tendinitis
Peroneal tendinitis is inflammation of the peroneus longus and peroneus brevis tendons along the outer ankle and lateral foot. Pain is usually felt behind and below the lateral malleolus, sometimes radiating toward the 5th metatarsal. Symptoms worsen with uneven terrain, side‑to‑side movements, or excessive pronation.
12. Cuboid Syndrome
Cuboid syndrome involves irritation or subtle subluxation of the cuboid bone, leading to sharp or aching pain on the outer midfoot. It often develops after repetitive lateral loading, sudden directional changes, or overuse. Patients may describe a feeling of “blockage” or discomfort during push‑off.
Struggling with pain on the outer side of your foot? Discover what cuboid syndrome is, why it happens, and how to fix it in our full guide: https://jointhealthguide.com/cuboid-syndrome/
Medial Foot Pain
Medial foot pain refers to discomfort felt on the inner side of the foot, often described as pain on inside of foot, inner foot pain, or pain along the arch. This region includes the tibialis posterior tendon, navicular bone, medial midfoot joints, and supporting ligaments — structures that commonly generate symptoms when overloaded.
Pain in this region is most often caused by:
- Tibialis Posterior Tendinitis — inflammation of the tendon that supports the arch, causing pain along the inner ankle and medial foot.
- Navicular Stress Fracture — a high‑risk stress injury presenting as deep, localized pain on the medial midfoot.
- Medial Midfoot Arthritis — degeneration of the medial tarsal joints, leading to stiffness and aching pain during weight‑bearing.
Tibialis posterior tendinitis is most common in active individuals and those with flatfoot mechanics, while navicular stress fractures appear in athletes exposed to repetitive high‑impact loading. Medial midfoot arthritis is more typical in older adults or after previous injuries.

13. Tibialis Posterior Tendinitis
Tibialis posterior tendinitis is inflammation of the tendon that supports the medial arch and stabilizes the inner side of the foot. Pain is typically felt along the inside of the ankle and medial foot, often worsening with prolonged walking, running, or activities that increase pronation. Early stages present with tenderness behind the medial malleolus; more advanced cases may show arch fatigue or mild flattening.
14. Navicular Stress Fracture
A navicular stress fracture is a high‑risk overuse injury affecting the navicular bone in the medial midfoot. Pain is usually deep, pinpoint, and localized on the inner midfoot, often aggravated by jumping, sprinting, or high‑impact sports. Because the navicular has limited blood supply, symptoms can be persistent and require careful evaluation.
15. Medial Midfoot Arthritis
Medial midfoot arthritis involves degeneration of the talonavicular and naviculocuneiform joints, leading to aching pain on the inner arch region. Symptoms include stiffness, swelling, and discomfort during weight‑bearing, especially on uneven surfaces. It is more common in older adults or individuals with previous midfoot injuries.
Bottom of Foot Pain (Plantar Foot Pain)
Bottom of foot pain refers to discomfort felt on the underside of the foot, including the heel, arch, and ball of the foot. Patients often describe this as pain on bottom of foot, pain under the foot, or pain when walking barefoot.
Pain in this region is most often caused by three anatomical zones:
- Heel Pain — most commonly plantar fasciitis and calcaneal heel spur, causing sharp pain with first steps in the morning.
- Arch Pain — typically related to plantar fascia overload, flatfoot mechanics, or tibialis posterior dysfunction.
- Ball of Foot Pain (Forefoot Pain) — includes metatarsalgia, Morton’s neuroma, and plantar plate irritation, all causing pain under the metatarsal heads.
Heel pain is common in adults with tight calves or prolonged standing, arch pain often appears with altered foot mechanics, while forefoot pain is typical in runners, walkers, and individuals wearing narrow or high‑heeled shoes.
Pain on the bottom of the heel is most often caused by plantar fasciitis and calcaneal heel spurs. Since we’ve already covered heel pain in detail in a separate article section, we won’t go deeper here — but it’s important to mention it as one of the key contributors to bottom‑of‑foot pain.
In the next sections, we’ll break down each region individually.

Arch Pain (Pain in the Arch of the Foot)
Pain in the arch of the foot is typically linked to plantar fascia overload or altered foot mechanics such as flatfoot. The medial longitudinal arch contains the plantar fascia, tibialis posterior tendon, and several stabilizing ligaments — structures that often become irritated when the arch collapses, is overstressed, or absorbs repetitive impact.
The most common causes include:
- Plantar Fascia Overload / Plantar Fasciopathy — aching or sharp pain along the arch, often worse after long walks or standing.
- Tibialis Posterior Dysfunction (Early Stage) — inner‑arch pain caused by fatigue or irritation of the tendon that supports the arch.
- Flatfoot‑Related Arch Strain — mechanical overload of the arch due to excessive pronation or collapsing foot posture.
Arch pain is common in individuals with increased training load, prolonged standing, or biomechanical changes such as flatfoot.
16. Plantar Fascia Overload / Plantar Fasciopathy
Plantar fascia overload causes aching or sharp pain along the medial arch, especially during prolonged standing or walking. Symptoms often develop when the plantar fascia absorbs excessive tension from tight calves, increased training load, or poor footwear support.
17. Tibialis Posterior Dysfunction (Early Stage)
Early tibialis posterior dysfunction leads to inner‑arch pain and fatigue as the tendon struggles to support the medial longitudinal arch. Patients typically report discomfort behind the medial malleolus or along the arch, especially during activities that increase pronation.
18. Flatfoot‑Related Arch Strain
Flatfoot mechanics place continuous stress on the arch structures, causing aching pain and a sense of collapse during weight‑bearing. Excessive pronation stretches the plantar fascia and tibialis posterior tendon, leading to progressive medial arch discomfort.
Ball of Foot Pain (Forefoot Pain / Metatarsalgia Zone)
Pain under the ball of the foot is commonly caused by metatarsalgia, Morton’s neuroma, or plantar plate irritation — especially in runners, walkers, and individuals who wear narrow or high‑heeled shoes. This region absorbs significant load during push‑off, making the metatarsal heads and surrounding soft tissues vulnerable to overload, compression, and repetitive stress.
The most common causes include:
19. Metatarsalgia
Metatarsalgia refers to overload of the metatarsal heads, causing aching, burning, or sharp pain under the forefoot. Symptoms worsen with prolonged walking, running, or tight footwear that increases pressure on the ball of the foot.
Struggling with pain under the ball of your foot? Read our full guide on Metatarsalgia (Ball of Foot Pain) to learn the key causes and the most effective treatment options.
20. Morton’s Neuroma
Morton’s neuroma is irritation or thickening of the interdigital nerve, most often between the 3rd and 4th metatarsals. Patients describe burning pain, tingling, or a “pebble in the shoe” sensation, typically aggravated by narrow shoes or forefoot compression.
21. Plantar Plate Irritation / Tear
Plantar plate irritation affects the ligament beneath the 2nd metatarsal head, leading to localized forefoot pain and sometimes mild toe deviation. Symptoms increase with push‑off activities and can mimic metatarsalgia in early stages.
22. Sesamoiditis
Sesamoiditis is inflammation of the sesamoid bones beneath the big toe joint, causing focal pain during push‑off. It is common in dancers, runners, and anyone performing repetitive forefoot loading.
23. Metatarsophalangeal Joint Arthritis
Metatarsophalangeal (MTP) joint arthritis affects the joints between the metatarsal bones and the toes, located directly beneath the ball of the foot. Degeneration or inflammation — most commonly from osteoarthritis or rheumatoid arthritis — leads to pain, stiffness, and swelling in one or more MTP joints. Symptoms worsen with walking and improve with rest, and patients may notice localized tenderness or visible swelling around the affected joint.
Big Toe Pain (Hallux Pain)
Big toe pain is a common problem because the hallux carries a large portion of body weight during walking, running, and push‑off. Pain in this region often comes from the first metatarsophalangeal (MTP) joint, the sesamoid bones, or soft‑tissue structures around the big toe. Symptoms may include stiffness, swelling, sharp pain during push‑off, or difficulty bending the toe.
The most frequent causes include joint degeneration, inflammation, overload injuries, and mechanical deformities.
25. Hallux Rigidus / Hallux Limitus
Hallux rigidus is arthritis of the first MTP joint, causing stiffness, reduced motion, and pain during walking. Early stages (hallux limitus) present with limited upward bending of the big toe, while advanced stages lead to significant joint degeneration and difficulty with push‑off.
26. Sesamoiditis
Sesamoiditis is inflammation of the sesamoid bones beneath the big toe joint. It causes focal pain during push‑off, especially in runners, dancers, and individuals who perform repetitive forefoot loading. Pain is typically sharp and localized under the big toe.
27. Gout (Big Toe Joint Inflammation)
Gout is a crystal‑induced inflammation that often affects the big toe joint, causing sudden, intense pain, redness, and swelling. Attacks frequently occur at night and can make even light touch extremely painful. The first MTP joint is the most classic location for gout flares.
28. Hallux Valgus (Bunion)
Hallux valgus is a deformity where the big toe drifts toward the second toe, creating a bunion on the inner side of the foot. This leads to pain, irritation from footwear, and altered mechanics during walking. Over time, the deformity can worsen and contribute to forefoot overload.
General Toe Pain / Lesser Toe Pain
Pain in the lesser toes (2nd–5th toes) can come from the joints, tendons, ligaments, or nerve structures around the toes. Because these toes are smaller and more flexible than the hallux, they are prone to overload, deformities, and capsular irritation, especially in people who walk long distances, wear narrow shoes, or have altered forefoot mechanics. Symptoms may include aching, burning, stiffness, swelling, or pain during push‑off.
The most common causes include capsular irritation, toe deformities, plantar plate problems, and nerve irritation.
29. Capsulitis of the Lesser MTP Joints
Capsulitis is inflammation of the joint capsule of the lesser metatarsophalangeal (MTP) joints, most often the 2nd MTP joint. It causes localized pain, swelling, and tenderness that worsens with walking. Patients often describe a bruised feeling under the affected toe.
30. Plantar Plate Injury (Lesser Toes)
Plantar plate irritation or partial tearing leads to pain beneath the 2nd metatarsal head, often accompanied by mild toe deviation or instability. Symptoms increase during push‑off and may mimic metatarsalgia in early stages.
31. Hammer Toe / Claw Toe / Mallet Toe
Toe deformities develop when the tendons and ligaments around the lesser toes lose balance, causing the toe to bend upward or downward. These deformities lead to pain from pressure points, shoe irritation, and altered forefoot loading.
32. Interdigital Neuritis (Non‑Morton’s)
Irritation of the small nerves between the toes can cause burning, tingling, or sharp pain. Unlike Morton’s neuroma, this neuritis may affect other web spaces and is often triggered by tight footwear or repetitive forefoot compression.
33. Arthritis of the Lesser MTP Joints
Degeneration or inflammation of the lesser MTP joints leads to aching pain, stiffness, and swelling. Symptoms worsen with walking and improve with rest. This condition may coexist with forefoot overload or toe deformities.
Foot Pain Diagnosis Procedure
Foot pain requires a clear and structured diagnostic approach because many different tissues can generate similar symptoms.
A clinician first listens to the patient’s story — when the pain started, where it is felt, whether it worsens with walking or improves with rest, and whether swelling, stiffness, or numbness are present. This helps determine whether the problem is more likely related to bone, joint, tendon, ligament, or nerve structures.
During the physical exam, the doctor inspects the foot for deformities such as bunions or hammer toes, checks for swelling or redness, and palpates specific areas like the plantar fascia, metatarsal heads, sesamoids, or MTP joints to identify the exact source of tenderness.
Range‑of‑motion testing of the big toe, ankle, and midfoot helps reveal stiffness typical of conditions like hallux rigidus or midfoot arthritis, while functional tests such as heel raises or forefoot loading can uncover tendon overload or plantar plate irritation.
Imaging is chosen based on which tissue is suspected.
X‑ray is the first step when bone or joint problems are likely. It shows fractures, bone spurs, joint space narrowing, and deformities — for example, hallux rigidus or MTP arthritis.
Ultrasound is excellent for soft tissues: it can detect plantar fascia thickening, tendon inflammation, tenosynovitis, joint effusion, and even Morton’s neuroma.
MRI provides the most detailed view, revealing plantar plate tears, early stress fractures, bone marrow edema, tendon tears, synovitis, and sesamoid injuries. When inflammatory or metabolic causes are suspected, blood tests such as uric acid or inflammatory markers help diagnose conditions like gout or rheumatoid arthritis.
By combining history, examination, and targeted imaging, clinicians can accurately identify the source of foot pain — whether it’s plantar fasciitis, metatarsalgia, Morton’s neuroma, sesamoiditis, arthritis, or tendon overload — and guide patients toward the right treatment.
Treatment
General treatment for foot pain focuses on reducing inflammation, improving tissue load tolerance, and restoring healthy biomechanics. Although specific conditions differ, most respond well to a combination of activity modification, supportive footwear, targeted exercises, and symptom‑relief strategies. Below is a clear, patient‑friendly overview of the main treatment approaches.
- Activity Modification — temporarily reducing high‑impact activities such as running or long walks helps calm irritated tissues. Switching to low‑impact exercise (cycling, swimming) often reduces symptoms quickly.
- Footwear Optimization — shoes with good cushioning, a stable heel counter, and adequate toe box space reduce pressure on the forefoot and improve arch support. Many patients improve simply by avoiding narrow or overly flexible shoes.
- Orthotic Support — prefabricated or custom orthotics can redistribute pressure, support the arch, and reduce strain on structures like the plantar fascia, metatarsal heads, and sesamoids.
- Strengthening Exercises — targeted exercises for the intrinsic foot muscles, calf complex, and tibialis posterior improve stability and reduce overload. Strengthening is especially helpful for arch pain, plantar fasciopathy, and metatarsalgia.
- Stretching — calf and plantar fascia stretches reduce tension on the heel and arch, improving mobility and decreasing morning stiffness.
- Ice or Heat — ice helps calm acute inflammation, while gentle heat can relax stiff joints or tight muscles.
- Anti‑Inflammatory Strategies — doctors may consider short‑term use of anti‑inflammatory approaches to reduce swelling and pain, especially in conditions like MTP arthritis or tendon irritation.
- Load Management — gradually increasing activity allows tissues to adapt without becoming overloaded again. This is essential for plantar plate injuries, sesamoiditis, and tendinopathies.
- Physical Therapy — therapists use manual techniques, taping, gait retraining, and progressive strengthening to restore normal mechanics.
- Medical Evaluation — persistent swelling, severe pain, inability to bear weight, or suspected fractures require professional assessment to rule out serious conditions.
Red Flags: When to See a Doctor Immediately
Certain symptoms require prompt medical evaluation because they may indicate a fracture, infection, severe inflammation, or nerve involvement. While most foot pain comes from overload or biomechanics, the following warning signs should not be ignored.
- Severe Swelling or Spreading Redness — rapidly increasing swelling, warmth, or redness that spreads across the foot may signal infection, acute inflammation, or a significant joint flare. This is especially important if the skin feels hot or if symptoms worsen over hours.
- Inability to Bear Weight — if you cannot put weight on the foot without sharp pain, a fracture, severe tendon injury, or joint damage may be present. Sudden inability to walk normally always warrants medical assessment.
- Night Pain — pain that wakes you from sleep or worsens at night can indicate a stress fracture, infection, or significant inflammation. Unlike mechanical pain, night pain does not improve with rest and should be evaluated.
- Sudden Big Toe Pain with Redness — abrupt, intense pain in the big toe joint accompanied by redness and swelling is characteristic of a gout flare. Because gout can mimic infection, proper diagnosis is important.
- Numbness, Tingling, or Burning — neurological symptoms may point to nerve entrapment, Morton’s neuroma, tarsal tunnel syndrome, or peripheral neuropathy. Persistent sensory changes should be assessed to prevent progression.
- Trauma with Visible Deformity — twisting injuries, falls, or impacts that result in abnormal foot shape, severe bruising, or inability to move the toes may indicate fractures or ligament ruptures.
Prognosis: How Long Recovery Usually Takes
Recovery time depends on which tissue is irritated, how long symptoms have been present, and how quickly load is adjusted, but most foot conditions follow predictable healing timelines. In general, soft‑tissue overload improves within weeks, while structural injuries or arthritis require longer‑term management. Below is a clear, patient‑friendly overview of typical recovery durations.
- Plantar Fasciitis — most patients improve within 6–12 weeks with stretching, load reduction, and supportive footwear. Morning pain usually decreases first, while full resolution may take several months if symptoms were long‑standing.
- Metatarsalgia — forefoot overload typically settles in 4–8 weeks once pressure is redistributed with footwear changes, metatarsal pads, and strengthening. Runners may need a gradual return to impact activities.
- Tendinopathies (Achilles, tibialis posterior, peroneal) — tendon recovery is slower because tendons adapt gradually to load. Most cases improve over 8–12 weeks, especially with progressive strengthening and careful load management.
- Stress Fractures — bone healing usually requires 6–10 weeks, depending on location. High‑risk areas like the navicular may take longer and require stricter rest. Pain should steadily decrease once impact activities are reduced.
- Arthritis — arthritis is chronic, with periods of improvement and flare‑ups. Symptoms can be well‑managed with footwear optimization, strengthening, and load control, but structural changes in the joint do not fully reverse.
Most patients experience meaningful improvement once they adjust activity levels, optimize footwear, and begin targeted exercises. If pain persists beyond expected timelines or worsens despite treatment, a medical evaluation can help rule out more serious conditions and guide further care.
FAQ: Frequently Asked Questions About Foot Pain
Why does my foot hurt in the morning?
Morning pain is most commonly linked to plantar fasciitis, because the plantar fascia tightens overnight and becomes painful with the first steps. Arthritis can also cause morning stiffness, though it usually improves gradually as the joint warms up.
Why does my foot hurt when walking barefoot?
Walking barefoot increases pressure on the heel, arch, and forefoot without cushioning. Conditions like plantar fasciitis, metatarsalgia, sesamoiditis, and flatfoot‑related arch strain often worsen without supportive footwear.
How do I know if it’s a stress fracture or just inflammation?
Stress fractures typically cause pinpoint pain, swelling, and discomfort that worsens with every step — often accompanied by night pain. Soft‑tissue inflammation is usually more diffuse and improves with rest. Imaging (X‑ray or MRI) is needed for confirmation.
Why do I feel burning or tingling in my toes?
Burning or tingling often indicates nerve irritation, such as Morton’s neuroma, interdigital neuritis, tarsal tunnel syndrome, or peripheral neuropathy. Persistent sensory changes should be evaluated by a clinician.
Can foot pain come from poor footwear?
Yes — narrow shoes, high heels, overly flexible footwear, or worn‑out soles can overload the forefoot, arch, or heel. Many conditions (metatarsalgia, neuroma, plantar fasciitis) improve significantly with proper footwear.
Is swelling always a sign of something serious?
Not always. Mild swelling can occur after long walks or standing. However, rapid swelling, spreading redness, or warmth may indicate infection, gout, or acute inflammation and should be assessed promptly.
Why does my big toe hurt during push‑off?
Pain during push‑off often comes from sesamoiditis, hallux rigidus, plantar plate irritation, or MTP arthritis. These structures carry high load during gait, making them prone to irritation.
Can foot pain be related to flat feet or high arches?
Absolutely. Flat feet often cause arch pain, tibialis posterior overload, and forefoot strain. High arches increase pressure on the heel and metatarsal heads, contributing to metatarsalgia and stress fractures.
When should I worry about toe deformities?
Hammer toe, claw toe, or mallet toe become concerning when they cause pain, shoe irritation, calluses, or difficulty walking. Progressive deformities should be evaluated to prevent worsening.
Can foot pain spread to the ankle or knee?
Yes — altered gait from foot pain can overload the ankle, knee, or even hip. Chronic foot pain often leads to compensatory movement patterns that affect other joints.
Hill CL, Gill TK, Menz HB, Taylor AW. Prevalence and correlates of foot pain in a population-based study: the North West Adelaide Health Study. Journal of Foot and Ankle Research. PubMed: Population-based study on foot pain prevalence and associated risk factors
Greenberg L, Davis H. Foot problems in the US: The 1990 National Health Interview Survey. Journal of the American Podiatric Medical Association. PubMed: National survey of foot disorders in the United States
Garrow AP, Silman AJ, Macfarlane GJ. The Cheshire Foot Pain and Disability Survey: a population survey assessing prevalence and associations. Pain. PubMed: Population study of foot pain prevalence and disability
Gates LS, Arden NK, Hannan MT, Roddy E, Gill TK, Hill CL, Dufour AB, Rathod-Mistry T, Thomas MJ, Menz HB, Bowen CJ, Golightly YM. Prevalence of Foot Pain Across an International Consortium of Population-Based Cohorts. Arthritis Care & Research. PubMed: International analysis of foot pain prevalence across population cohorts
Patel J, Swords M. Hallux Rigidus. StatPearls. NCBI Bookshelf. Evidence-based review: Hallux rigidus diagnosis and management
Fenando A, Rednam M, Gujarathi R, et al. Gout. StatPearls. NCBI Bookshelf. Evidence-based review: Gout diagnosis, clinical presentation, and treatment
Goransson M, Constant D. Hammertoe. StatPearls. NCBI Bookshelf. Evidence-based review: Hammertoe evaluation and management
















