

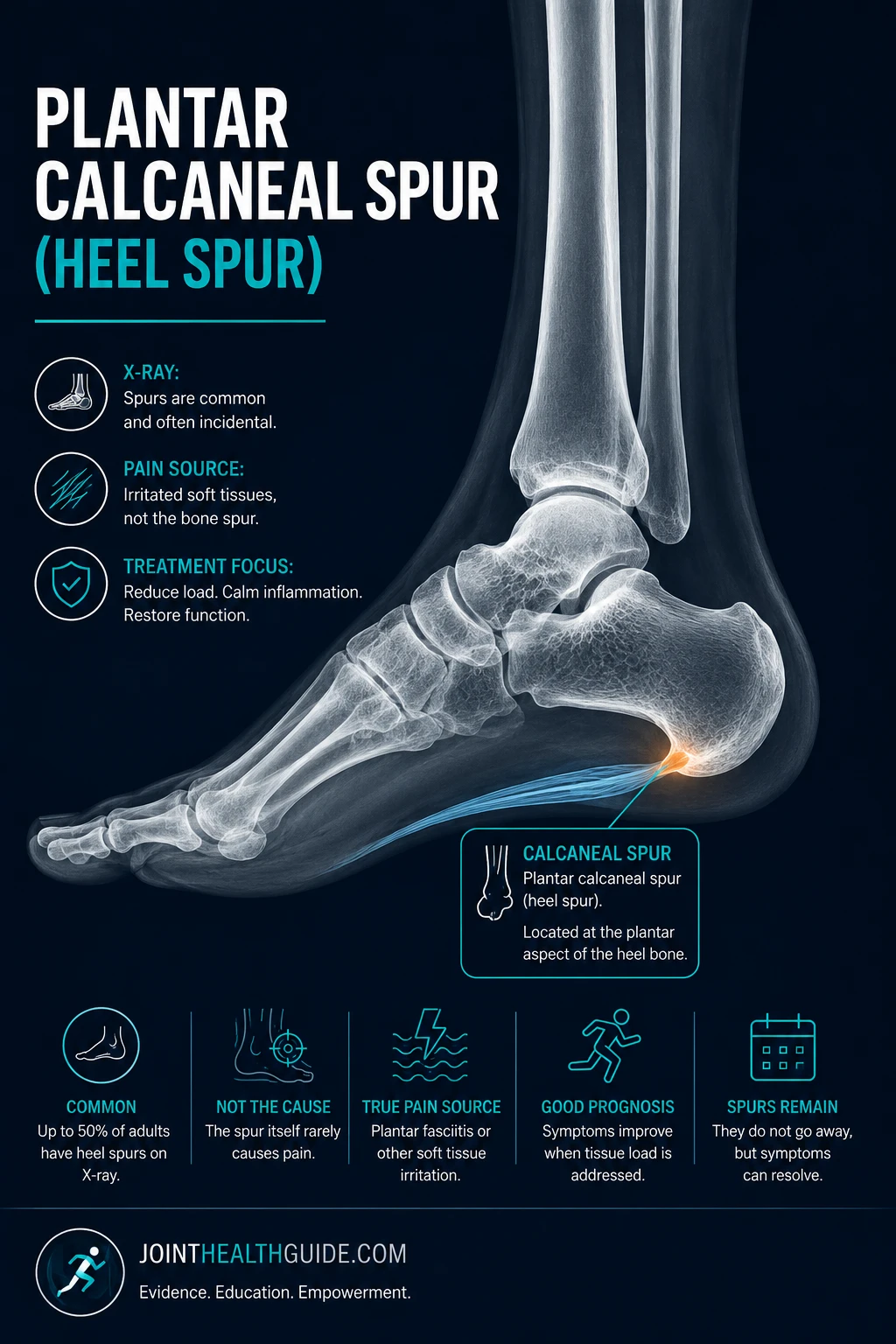
A heel spur (calcaneal spur) is a small bony outgrowth on the underside of the heel bone. In medical terminology, this structure is also called a plantar calcaneal spur or plantar calcaneal enthesophyte. It develops as an adaptive response to increased mechanical load on the heel and plantar fascia and is often found incidentally on X‑ray.
Although commonly mentioned together with plantar fasciitis, a heel spur is not the same condition. Plantar heel spurs are widespread and usually asymptomatic, but when painful, they cause localized discomfort on the bottom of the heel during weight‑bearing.
Diagnosis is typically confirmed with X‑ray, and treatment is conservative, focusing on reducing mechanical stress on the heel and plantar fascia. This article provides a clear overview of the causes, symptoms, and treatment options for plantar heel spurs.
Key Clinical Points – Heel Spur (Calcaneal Spur)
- Heel spur is a bony outgrowth on the underside of the heel, most often found incidentally on X‑ray.
- It develops as an adaptive response to long‑term mechanical load, traction from the plantar fascia, or compression forces on the calcaneus.
- Most heel spurs are asymptomatic; when pain occurs, it usually comes from overloaded soft tissues, not the spur itself.
- Risk factors include age, excessive pronation, high body weight, prolonged standing, plantar fasciitis, and inflammatory arthropathies.
- Diagnosis is confirmed with X‑ray; ultrasound and MRI are used to assess soft‑tissue causes of heel pain.
- Treatment is conservative: load modification, supportive footwear, orthotics, stretching, and shockwave therapy.
- Heel spurs do not regress, but symptoms often resolve once soft‑tissue irritation is treated.
What Is a Heel Spur and Why It Forms
A heel spur is a small bony outgrowth on the underside of the heel bone. In medical litterature is often described as a calcaneal spur, plantar calcaneal spur, or plantar calcaneal enthesophyte. It typically appears as a short, triangular shaped projection extending toward the heel fat pad.
The exact reason a heel spur forms is not completely understood, but most evidence suggests it develops as a natural adaptation to increased mechanical stress. One explanation is that repeated traction forces from the plantar fascia and small foot muscles pull on their attachment to the heel bone. Over time, this constant tension can stimulate the bone to thicken and form a spur. This mechanism is more common in people with excessive pronation, higher body weight, or long periods of standing and walking, all of which increase strain on the plantar fascia.
Another explanation focuses on direct compression of the heel bone during weight‑bearing. Bone remodels in response to load. Repeated pressure on the underside of the calcaneus can trigger a reaction in the periosteum, leading to gradual bone growth. This is similar to how osteophytes form in other joints exposed to chronic stress.
Most researchers agree that both mechanisms—traction and compression—likely work together. Today it is well understood that a heel spur can originate not only from the attachment of the plantar fascia, but also from the entheses of several intrinsic foot muscles.
Regardless of the exact source, a heel spur represents the body’s attempt to reinforce an area exposed to long‑term mechanical load.
How Common Is a Plantar Calcaneal Enthesophyte?
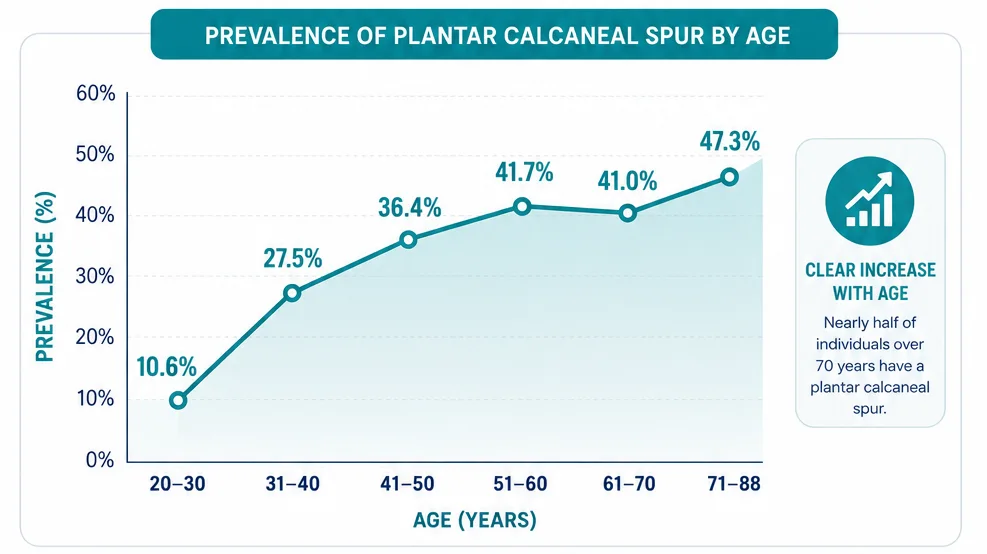
A plantar heel spur (calcaneal spur) becomes increasingly common with age. Younger adults rarely show this finding on X‑ray, but its prevalence rises steadily across decades of life. In the 20–30 age group, only about 10% of people have a plantar heel spur. By ages 31–40, the rate increases to 27%, and by 41–50 it reaches more than 36%. The trend continues upward in older adults: around 42% of individuals in their 50s and early 60s have a spur, and nearly half of people over 70 show a calcaneal spur on imaging.
Gender and side (left vs. right foot) do not appear to significantly influence prevalence, as rates are similar between men and women and between both feet.
The chart below illustrates the prevalence of heel spurs across different age groups, showing a clear increase in frequency with advancing age.
Risk Factors and Associated Conditions in Heel Spur Formation
Several factors increase the likelihood of developing a heel spur (plantar calcaneal enthesophyte). These factors influence how much mechanical stress the heel bone and plantar fascia are exposed to, as well as how the body responds to long‑term loading. The most important contributors include:
- Older age — connective tissues lose elasticity over time, making the plantar fascia and Achilles tendon less effective at absorbing load. Aging also increases the tendency toward calcification at tendon and ligament insertions. Gait patterns change as well, with longer heel contact and shorter steps, all of which increase stress on the heel. Studies show that heel spurs are present in more than half of individuals over 62.
- Increased body weight — excess weight places continuous load on the longitudinal arch, plantar fascia, and heel bone. Research indicates that nearly half of people with heel spurs are overweight, highlighting the strong link between body mass and spur formation.
- Excessive foot pronation — too much inward rolling of the foot during walking increases tension on the plantar fascia. This is common in people with flat feet, and up to 62% of patients with heel spurs show excessive pronation.
- Foot structure — flat feet, low arches, or altered biomechanics can increase traction forces on the plantar fascia and intrinsic foot muscles, promoting spur development.
- Plantar fasciitis — chronic inflammation and overload of the plantar fascia increase traction at its attachment to the heel bone, making spur formation more likely. Although the two conditions are not the same, they frequently coexist.
- Inflammatory arthropathies — conditions such as ankylosing spondylitis, psoriatic arthritis, and reactive arthritis cause inflammation at entheses, which can lead to enthesophyte formation, including heel spurs.
- Osteoarthritis — people with osteoarthritis and osteophytes in other joints have a much higher likelihood of developing heel spurs. This suggests a general predisposition toward bone spur formation throughout the body.
Heel Spur vs. Plantar Fasciitis: What’s the Difference?
People often assume that any pain on the bottom of the heel must be caused by a heel spur, even though plantar fasciitis is by far the more common source of symptoms. This misunderstanding happens because both conditions affect the same anatomical region and frequently coexist, but they are not the same disorder.
Research shows that plantar calcaneal spurs are present in 45–85% of people with plantar fasciitis, and the two share several major risk factors—such as obesity, prolonged standing, flat feet, and advancing age—suggesting that they may be linked in their development.
Still, their underlying mechanisms differ: plantar fasciitis is a degenerative‑inflammatory problem of the plantar fascia itself, typically causing sharp pain with the first steps in the morning or after rest. On the other hand heel spur is a bony outgrowth at the fascial insertion that is often completely asymptomatic. Many individuals have a spur visible on X‑ray without any heel pain at all, and the size of the spur does not predict symptom severity.
In clinical practice, heel pain is much more commonly caused by plantar fasciitis than by the spur, and discomfort attributed to a “spur” is usually the result of fascial overload rather than the bone itself.
Do Heel Spurs Cause Pain?
Many people with a plantar calcaneal enthesophyte never develop symptoms, even though the spur sits exactly where heel pain often appears. Still, research shows those who do have a spur experience heel pain more often than people without one.
The relationship between spurs and painful heels appears true, but a clear pattern remains: a large subgroup of patients with a spur feel no pain at all.
When symptoms do occur, they usually involve heel pain during walking, especially in hard shoes or when walking barefoot on firm surfaces. The discomfort often feels sharp or bruised under the heel. A heel spur can cause pain when it compresses nearby soft tissues or nerves, especially during weight‑bearing. It may also trigger discomfort if inflammation develops around the spur, making the surrounding structures sensitive during walking or standing.
Other conditions explain heel pain far more often, including plantar fasciitis, small tears of the plantar fascia, calcaneal stress fractures, and fat pad atrophy. These problems can irritate the tissues around the spur and make the area sensitive. Because of this overlap, people with a spur may report pain more frequently, but the spur is usually not the true cause.
Clinical Insight
In practic,e other soft‑tissue or bone conditions are more common drivers of heel pain than the spur itself, and many individuals with a visible spur remain completely asymptomatic.
Learn more about other conditions that can cause heel pain in the full article “Heel Pain: 11 Most Common Causes and Effective Treatments” .
Diagnosis
Calcaneal spurs — plantar calcaneal enthesophytes — are diagnosed mainly through imaging. Because large proportion of them are asymptomatic, imaging helps confirm their presence and evaluate nearby soft tissues that may actually cause pain.
- X‑ray is the first‑line and most accurate method. It clearly shows the size and shape of the spur.
- Ultrasound is less reliable for plantar spurs but excellent for assessing soft‑tissue conditions such as plantar fasciitis.
- MRI is rarely needed. It’s reserved for atypical heel pain, suspected stress fractures, or complex soft‑tissue pathology.

Treatment of Heel Spurs (Calcaneal Spurs)
In many cases, conservative care can effectively reduce heel pain linked to heel spurs. These treatments focus on lowering strain on the plantar fascia and calming irritated soft tissues. It is important to understand the factors that contribute to spur formation, including repetitive load, biomechanical abnormalities, improper footwear, and excess body weight. Addressing these factors helps reduce symptoms and prevents recurrence.
Heel spurs themselves cannot shrink or disappear with conservative treatment. Spurs remain visible on X‑ray even after symptoms resolve, because the pain usually comes from overloaded soft tissues, not the bone.
First‑Line Treatment (Conservative Care)
These non‑invasive strategies are the foundation of heel spur management. Most patients improve within several weeks when they apply them consistently.
- Load modification — reduce standing and walking on hard surfaces; avoid barefoot walking.
- Footwear changes — use cushioned, supportive shoes with a stable heel counter.
- Orthotic insoles — support the arch and reduce pressure on the plantar fascia.
- Stretching exercises — stretch the calf muscles and plantar fascia to reduce tension.
- Ice and short‑term NSAIDs — help reduce pain during flare‑ups.
- Weight management — lowers mechanical stress on the heel with every step.
These measures target the true source of pain, which is usually soft‑tissue overload rather than the spur itself.
Advanced Treatment Options (When Pain Persists)
If symptoms remain after several weeks of conservative care, additional therapies may help.
- Physical therapy — strengthens foot and calf muscles and improves gait mechanics.
- Night splints — reduce morning pain by preventing overnight tightening.
- Shockwave therapy (ESWT) — stimulates tissue healing and reduces chronic pain.
- Injection therapies — corticosteroids, dextrose prolotherapy, or PRP may help in resistant cases.
- Surgery – heel spur removal — rarely required; considered only when severe symptoms persist despite all other treatments.
Heel spurs usually remain visible on X‑ray, but symptoms often resolve once soft‑tissue irritation is controlled and biomechanical load improves.
Prognosis
Most people with a heel spur have no symptoms. Among those who do feel pain, symptoms usually improve with conservative treatment and better load management. Spurs remain visible on X‑ray, but pain often resolves once soft‑tissue irritation settles.
FAQ
Can a heel spur cause pain?
Sometimes, but pain usually comes from soft‑tissue overload, not from the spur itself.
Can a calcaneal spur go away?
No. Heel spurs do not regress, but symptoms can fully resolve.
Is surgery needed?
Rarely. Heel spur surgery is considered only when severe pain persists despite all conservative options.
Is a plantar calcaneal enthesophyte dangerous?
No. A plantar calcaneal enthesophyte is a benign adaptive bone change.
Velagala VR, Velagala NR, Kumar T, Singh A, Mehendale AM. Calcaneal Spurs: A Potentially Debilitating Disorder. Cureus. 2022 Aug 28;14(8):e28497. DOI: Calcaneal spur pathology and clinical overview
Allam AE, Chang KV. Plantar Heel Pain. StatPearls [Internet]. Updated 2024 Jan 4. Clinical review: diagnosis and management of plantar heel pain
Mohseni M, Mousavi E, Alebouyeh MR. Key Considerations When Targeting a Heel Spur. Anesth Pain Med. 2023 Oct 1;13(5):e139326. DOI: Clinical considerations in heel spur interventions
Kirkpatrick J, Yassaie O, Mirjalili SA. The plantar calcaneal spur: a review of anatomy, histology, etiology and key associations. J Anat. 2017 Jun;230(6):743–751. Wiley: Anatomy and pathology of plantar calcaneal spur

















