

Metatarsalgia is the term used for pain in the front part of the foot — the ball of the foot — located beneath the metatarsal heads. This area sits between the foot arches and the toes and plays a key role in weight‑bearing during walking and running. Metatarsalgia can develop for many reasons, including excessive forefoot loading, abnormal weight distribution, foot deformities, overuse injuries, inflammatory conditions, or neurological disorders.
Although metatarsalgia is not usually a serious condition, it can interfere with daily activities, cause discomfort while walking or standing, and significantly reduce mobility.
Treatment depends on the underlying cause. In many cases, simple measures such as changing footwear, reducing high‑impact activities, resting the foot, or losing excess body weight can provide meaningful relief.
In this article, I will explain the most common causes of metatarsalgia, why they occur, the typical symptoms, available treatment options, and practical strategies to relieve pain and prevent recurrence.
Key Clinical Points – Metatarsalgia
- Metatarsalgia is pain and tenderness in the ball of the foot caused by increased pressure on the metatarsal heads.
- Symptoms typically worsen with weight‑bearing (walking, running, standing) and improve with rest.
- Common contributing factors include foot deformities (hallux valgus, hammertoes), Morton’s neuroma, overuse, and excess body weight.
- Sports and impact activities such as running and jumping often aggravate forefoot pain.
- Redness, warmth, or marked swelling suggest inflammatory conditions like arthritis or gout rather than isolated metatarsalgia.
- Most cases improve with footwear modification, orthotic support, activity adjustment, and physical therapy.
What Is Metatarsalgia?
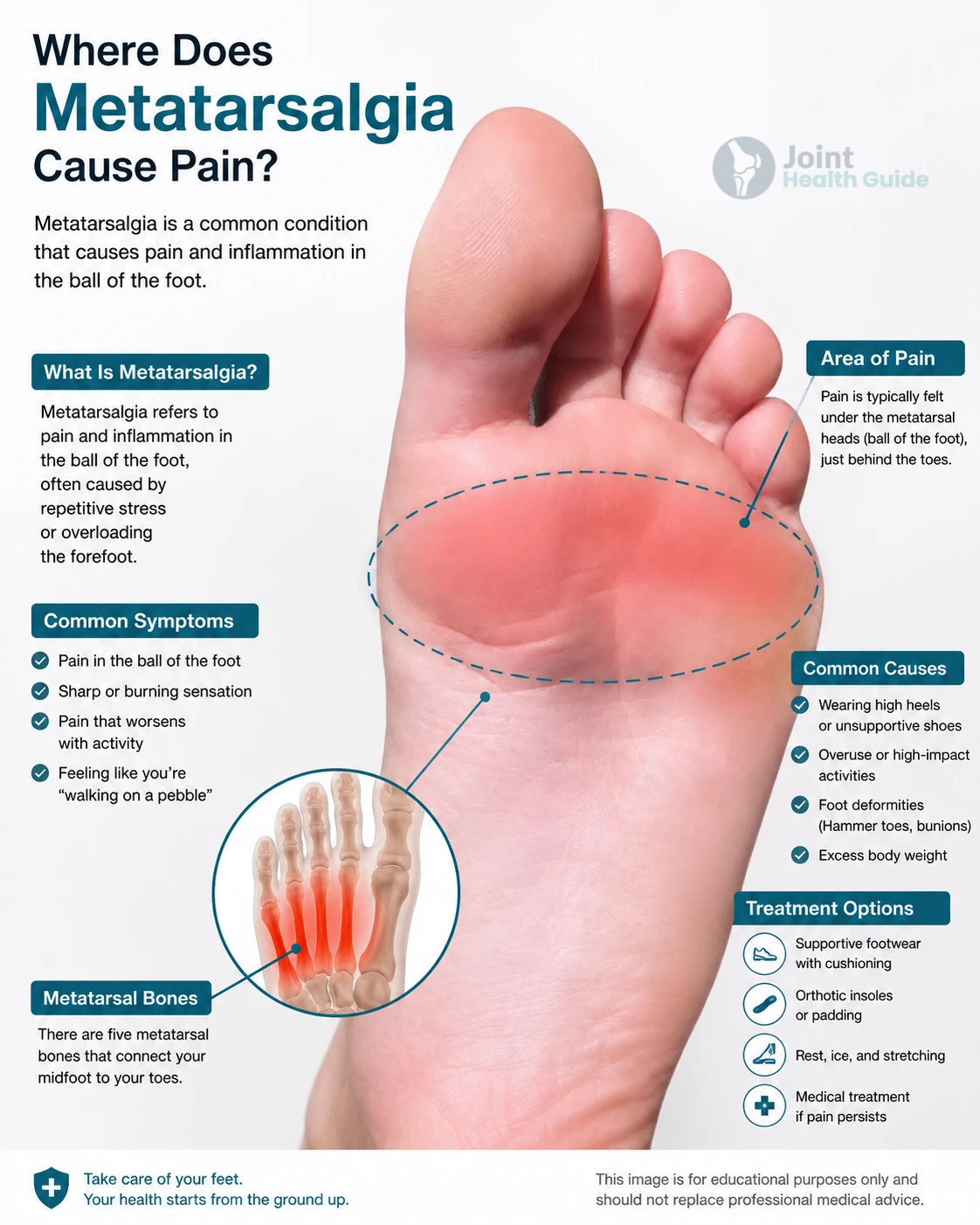
Metatarsalgia is the medical term for pain in the front part of the foot, beneath the heads of the metatarsal bones — the area commonly known as the ball of the foot.Patients often describe it as pain under the toes or pain in the forefoot. The painful area is located on the underside of the foot between the arch and the toes, directly beneath one or more metatarsal heads.
Metatarsalgia is a symptom, not a diagnosis.
It develops when one or more of the five metatarsal heads become overloaded or irritated. The pain is usually concentrated beneath one or several metatarsal bones, depending on the underlying cause.
Anatomically, the metatarsal heads form the main weight‑bearing platform of the forefoot during walking and running, which explains why even small biomechanical changes can trigger significant discomfort.
Metatarsalgia Symptoms
Metatarsalgia most commonly causes pain and discomfort in the ball of the foot, especially during activities that increase pressure on the forefoot. Symptoms usually develop gradually and tend to improve with rest.
Typical Symptoms
- Pain under the metatarsal heads (ball of foor pain) — often described as aching, sharp, or bruised‑like.
- Pain that worsens with weight‑bearing — walking, running, jumping, or standing for long periods.
- Relief during rest — symptoms usually decrease when sitting or lying down.
- Sensitivity when walking barefoot — especially on hard surfaces.
- Feeling of walking on a pebble — a common description in forefoot pain conditions.
Less Common Symptoms
- Mild swelling in the front of the foot.
- Tenderness when pressing the area beneath the metatarsal heads.
Symptoms That Suggest Another Condition
- Tingling or numbness → more typical for Morton’s neuroma than for metatarsalgia.
- Redness, warmth, or significant swelling → may indicate arthritis or gout rather than isolated metatarsalgia.
Causes of Metatarsalgia
Metatarsalgia most commonly develops due to biomechanical overload of the forefoot. In 85–90% of cases, the primary problem is an abnormal distribution of pressure across the metatarsal heads during walking or running. Foot structure, gait abnormalities, inappropriate footwear, excess body weight, and certain medical conditions can all contribute to pain beneath the toes.
Because metatarsalgia is a symptom rather than a diagnosis, identifying the underlying cause is essential for effective treatment and long‑term prevention.
| Cause Category | Examples | How It Causes Metatarsalgia |
|---|---|---|
| Mechanical & Biomechanical Factors |
Excessive pronation High arches (pes cavus) Flat feet (pes planus) Long second metatarsal Hammer toes Claw toes Tight Achilles tendon |
Uneven weight distribution increases pressure beneath one or more metatarsal heads, leading to irritation and pain. |
| Footwear |
High heels Hard-soled shoes Minimalist shoes Poorly fitting shoes |
Inadequate cushioning or altered foot position concentrates pressure on the ball of the foot. |
| Structural & Medical Conditions |
Hallux valgus (bunion) Hallux rigidus Morton’s neuroma Freiberg disease Osteoarthritis Rheumatoid arthritis Gout |
Pain, deformity, inflammation, or nerve irritation alter gait mechanics and overload the metatarsal heads. |
| Sports & Overuse |
Running Jumping sports Sudden increase in training Excess body weight |
Repetitive impact and excessive loading exceed the forefoot’s ability to absorb stress, resulting in chronic irritation. |
| Post-Surgical (Iatrogenic) |
Hallux valgus surgery Metatarsal osteotomy (Weil) Hammer toe correction |
Surgical changes in bone alignment or metatarsal length may redistribute pressure and cause persistent forefoot pain. |
1. Mechanical Causes (Most Common)
Mechanical or biomechanical metatarsalgia occurs when the forefoot experiences uneven or excessive loading. This is by far the most frequent cause of ball of the foot pain and accounts for the majority of cases. The condition develops when one or more metatarsal heads absorb more pressure than they are designed to handle, leading to irritation, inflammation, and pain beneath the toes.
Biomechanical metatarsalgia arises from an uneven distribution of pressure across the forefoot. This imbalance may result from abnormalities in either the functional mechanics of the foot or its structural anatomy. In practice, these two factors are closely linked: long‑standing functional issues can gradually lead to permanent structural changes in the bones and joints of the forefoot, further increasing overload on the metatarsal heads.
The most common mechanical contributors include:
- Excessive pronation — inward collapse of the foot increases pressure on the central metatarsals.
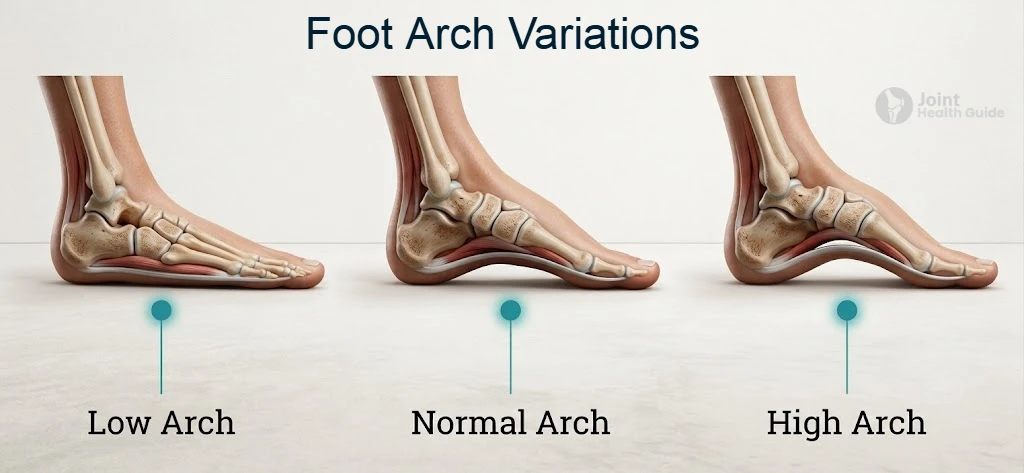
- High arches (pes cavus) — a rigid, elevated arch shifts weight to the metatarsal heads.
- Flat feet — reduced arch support leads to instability and overload.
- Long second metatarsal — increases pressure under the second metatarsal head.
- Hammer toes or claw toes — alter weight distribution and reduce shock absorption.
- Limited ankle mobility or a tight Achilles tendon — shifts load forward onto the metatarsal heads.
Excessive Pronation
Excessive pronation refers to an inward collapse or excessive inward rotation of the foot during stance and push‑off. When the foot remains too far in this position while walking or running, the forefoot becomes unstable, causing increased pressure on the central metatarsal heads and contributing to metatarsalgia.
In normal gait, the foot should realign and stabilize before push‑off. With excessive pronation, this stabilization does not occur, leading to overload of various structures in the forefoot. The condition may result from ligamentous laxity, malalignment of the foot bones, previous injuries, or differences in leg length.
Excessive pronation is commonly seen in people with flat feet, but it can also occur in individuals with normal or even high arches. Regardless of foot type, prolonged abnormal mechanics can gradually lead to structural changes in the forefoot, further increasing pressure beneath the metatarsal heads.

Pes Cavus (High Arches)
Pes cavus refers to a naturally high medial arch that concentrates weight on the heel and the metatarsal heads. Many people have high arches as a normal anatomical variant, and in many cases it does not represent a medical problem. However, when the arch is rigid or lacks adequate shock absorption, the forefoot is exposed to increased loading, which can contribute to metatarsalgia.
Because a high‑arched foot typically has reduced contact area with the ground, pressure becomes focused on fewer points. This often leads to forefoot pain, callus formation, and increased stress beneath the central metatarsals. Individuals with pes cavus may also experience reduced stability during walking or running, which further amplifies forefoot overload.
In the context of metatarsalgia, pes cavus is relevant primarily due to its biomechanical effect—not because it is inherently pathological. Treatment focuses on improving shock absorption and redistributing pressure, most commonly through cushioned orthotic insoles and footwear modifications. Only severe, rigid deformities require surgical consideration.
Flat Feet (Pes Planus)
Flat feet are characterized by a lowered or collapsed medial arch, which reduces the foot’s natural ability to absorb shock. When the arch does not provide adequate support, the forefoot becomes less stable during stance and push‑off, leading to increased loading beneath the metatarsal heads and contributing to metatarsalgia.
People with flat feet often exhibit excessive pronation, a functional pattern that shifts pressure toward the central forefoot. Over time, this abnormal loading can cause pain, callus formation, and irritation of the soft tissues around the metatarsal joints.
In the context of metatarsalgia, flat feet are relevant primarily because of their biomechanical effect—not because they are inherently problematic. Treatment focuses on improving arch support and redistributing pressure through orthotic insoles, supportive footwear, and targeted strengthening of the intrinsic foot muscles.
Long Second Metatarsal
A long second metatarsal is a common anatomical variant in which the second metatarsal bone extends slightly farther than the others. Although this is often a normal structural feature, it can increase pressure beneath the second metatarsal head during walking and running. Because the second ray becomes the primary load‑bearing point in the forefoot, even small increases in length can lead to localized overload, irritation, and pain characteristic of metatarsalgia.
People with a long second metatarsal often develop calluses under the second metatarsal head and may experience discomfort during activities that involve forefoot push‑off. The issue is biomechanical rather than pathological: the longer bone simply absorbs more force.
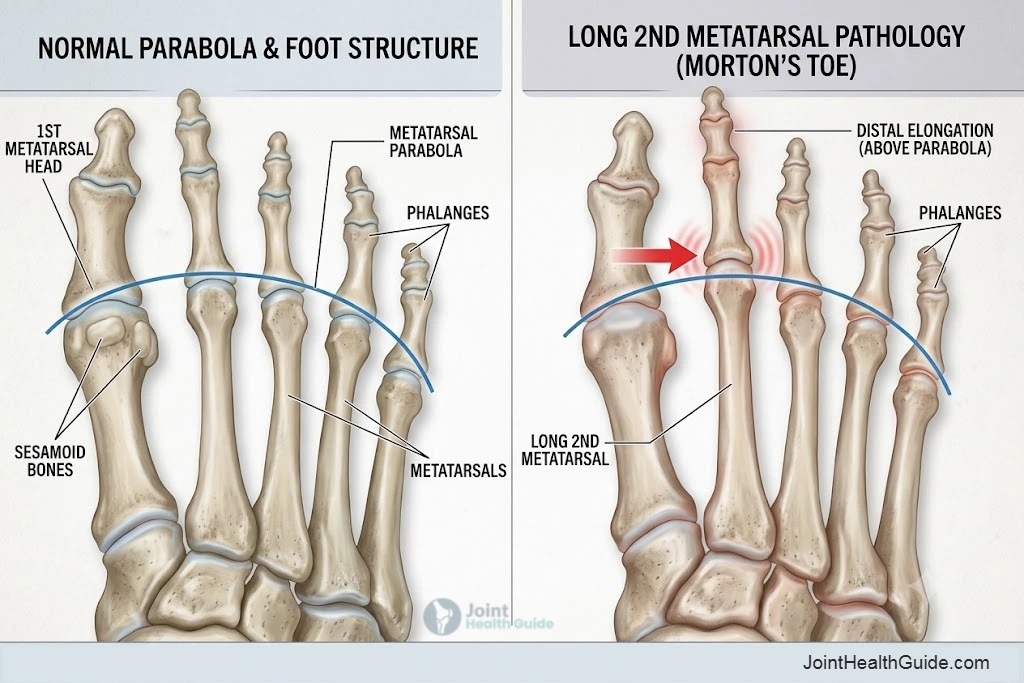
Treatment focuses on redistributing pressure through orthotic insoles, metatarsal pads, and footwear with adequate cushioning, while persistent or severe cases may require more advanced offloading strategies.
Hammer Toes and Claw Toes
Hammer toes and claw toes are deformities in which the toes bend abnormally, reducing their ability to stabilize the forefoot and absorb shock during walking. In claw toe deformity, all three joints of the toe are affected: the metatarsophalangeal joint bends upward, while the middle and distal joints bend downward, creating a claw‑like shape.
In hammer toe deformity, the toe is permanently flexed at the middle joint, giving it a characteristic “hammer” appearance.

These deformities may be congenital or develop over time due to tight footwear, high heels, muscle imbalance, nerve injury, or structural foot issues. When the toes lose their normal alignment and function, they can no longer assist in distributing load during push‑off.
As a result, more pressure is transferred to the metatarsal heads, increasing the risk of metatarsalgia, callus formation, and localized forefoot pain. The key problem is the biomechanical effect—reduced toe function leads to increased forefoot overload.
2. Footwear‑Related Causes
Footwear plays a major role in forefoot loading, and certain shoe types can significantly increase pressure beneath the metatarsal heads. Shoes with hard soles reduce natural shock absorption, causing impact forces to transfer directly to the forefoot. Over time, this leads to irritation, callus formation, and pain characteristic of metatarsalgia.
High heels shift body weight forward, placing the majority of load on the central metatarsals and shortening the Achilles tendon, which further increases forefoot pressure during walking.
Minimalist shoes, although popular in sports, offer very little cushioning and require strong intrinsic foot muscles to maintain proper mechanics. When used excessively or without adequate adaptation, they can increase forefoot stress and contribute to overload. In all three cases, the problem is biomechanical: reduced cushioning, altered foot position, or insufficient support leads to excessive pressure on the forefoot, making footwear a common and modifiable contributor to metatarsalgia.
3. Medical, Structural & Systemic Causes
Inflammatory disorders such as arthritis and gout cause joint swelling, pain, and reduced mobility, which disrupt normal load distribution during walking. Nerve‑related conditions like Morton’s neuroma create localized irritation between the metatarsals, further amplifying discomfort in the forefoot.
Structural deformities—including hallux valgus, hallux rigidus, and Freiberg disease—shift load away from the big toe and toward the central metatarsals. Although each condition has a different origin, they share a common biomechanical consequence: impaired forefoot function and increased localized pressure that can lead to metatarsalgia.
Arthritis
Arthritis, including osteoarthritis and rheumatoid arthritis, can cause inflammation, cartilage damage, and stiffness in the metatarsophalangeal joints. When these joints lose mobility or become painful, the forefoot cannot absorb load efficiently during walking. This altered gait pattern increases pressure on the metatarsal heads and may lead to metatarsalgia, especially during prolonged standing or push‑off.
Gout
Gout is an inflammatory joint condition caused by the deposition of monosodium urate crystals. It most commonly affects the big toe, producing sudden, severe pain, swelling, and warmth. During an acute attack, patients often avoid loading the affected joint, shifting weight toward the central metatarsals. This compensatory gait increases forefoot pressure and can trigger or worsen metatarsalgia.
Freiberg Disease
Freiberg disease is a condition in which the head of a metatarsal bone—most commonly the second—undergoes avascular necrosis. The loss of blood supply leads to collapse, fragmentation, and degeneration of the joint surface.
This process causes pain, swelling, and stiffness in the front part of the foot, and it is most frequently seen in adolescent girls, although adults can also develop symptoms later in life.
As the affected metatarsal head becomes damaged and loses its normal shape, the joint becomes painful during weight‑bearing activities. This discomfort often makes walking difficult and can lead to increased sensitivity in the ball of the foot. Because the metatarsal head is structurally weakened, everyday activities such as standing, walking, or pushing off the ground can trigger or worsen pain, making Freiberg disease a recognized cause of metatarsalgia.
Morton’s Neuroma
Morton’s neuroma is a thickening of the interdigital nerve, most commonly located between the third and fourth toes. It develops as a result of prolonged pressure or irritation of the nerve and typically causes burning pain, tingling, or the sensation of “walking on a pebble.” Symptoms often worsen when wearing tight or narrow shoes, or when walking barefoot on hard surfaces.
Because the irritated nerve sits in the ball of the foot, pain can become more noticeable during weight‑bearing activities such as standing, walking, or running. Many patients instinctively shift their weight to avoid the painful area, which can increase sensitivity in the forefoot and contribute to metatarsalgia.
Diagnosis is based on clinical examination and may be supported by imaging such as ultrasound or MRI. Treatment options include footwear modification, orthotic inserts, physical therapy, corticosteroid injections, or, in more persistent cases, surgical removal of the neuroma.
Hallux Rigidus
Hallux rigidus is a degenerative condition of the big toe’s metatarsophalangeal (MTP) joint that leads to reduced mobility and pain. It develops due to osteoarthritis, which causes cartilage wear, joint inflammation, and the formation of painful bony spurs (osteophytes).
Over time, movement of the big toe becomes increasingly limited, making walking difficult and often uncomfortable, especially during activities that require bending the toe.
As the joint stiffens and loses its normal range of motion, patients may change the way they walk to avoid pain. This altered gait can shift pressure toward the ball of the foot, increasing sensitivity and contributing to metatarsalgia. Because the big toe plays a key role in normal push‑off during walking, any restriction in its movement can lead to overload of nearby structures and persistent forefoot discomfort.
Hallux Valgus (Bunion)
Hallux valgus is a deformity of the big toe’s metatarsophalangeal (MTP) joint in which the toe gradually shifts toward the second toe. This inward deviation creates a visible bump on the inner side of the foot, commonly referred to as a bunion. The skin and soft tissues around the joint often become thickened and irritated, leading to inflammation, swelling, and pain, especially when wearing tight or narrow shoes.
As the deformity progresses, the big toe becomes less effective during walking, and patients may unconsciously shift weight away from the painful joint. This change in load distribution can increase pressure in the ball of the foot, making everyday activities such as standing or walking more uncomfortable. For many individuals, hallux valgus becomes a contributing factor to metatarsalgia due to the added strain placed on the central metatarsals.
4. Sports & Overuse Factors
Sports and repetitive activities can place significant stress on the ball of the foot and contribute to metatarsalgia. Running and jumping repeatedly load the forefoot, especially during push‑off, which can irritate the metatarsal heads and surrounding soft tissues.
Sudden increases in training volume or intensity—such as starting a new exercise program, switching surfaces, or rapidly increasing mileage—may overwhelm the foot’s ability to adapt, leading to pain and inflammation in the front part of the foot.
Excess body weight is another important factor. Overweight and obesity increase the overall load placed on the feet, with the metatarsal heads absorbing a large portion of this pressure during standing and walking. Over time, this added stress can make everyday activities uncomfortable and significantly raise the risk of developing metatarsalgia.
Together, high‑impact sports, sudden training changes, and increased body weight represent common overuse‑related contributors to forefoot pain.
5. Post‑Surgical Bal of Foot Pain (Iatrogenic Metatarsalgia)
Iatrogenic metatarsalgia refers to pain in the ball of the foot that develops after surgical procedures affecting the forefoot. It occurs when an operation changes the natural relationships between the bones, joints, or soft tissues, leading to altered pressure distribution during standing and walking.
This type of pain most commonly appears after surgeries such as hallux valgus correction, metatarsal osteotomies (including Weil osteotomy), or procedures performed to correct toe deformities like hammer or claw toes.
Following these interventions, some patients experience increased sensitivity or discomfort beneath the metatarsal heads. This may happen if the operated bone heals in a slightly different position, if the length of a metatarsal changes, or if the forefoot mechanics are unintentionally altered.
As a result, everyday activities such as walking, standing, or wearing certain types of footwear can become painful. Post‑surgical forefoot pain is a recognized cause of metatarsalgia and may require footwear adjustments, orthotic support, physical therapy, or, in rare cases, additional medical evaluation.
Metatarsalgia Treatment
Treatment for metatarsalgia depends on the underlying cause of ball of foot pain. Most patients benefit from general measures that reduce pressure on the forefoot, while specific treatments are used for conditions such as Morton’s neuroma, hallux valgus, or structural deformities. Conservative care is usually effective, and surgery is considered only when symptoms persist despite appropriate management.
General Measures
- Rest with elevated feet — reducing daily load often decreases pain and swelling.
- Weight reduction — lowering body weight decreases pressure on the metatarsal heads and can significantly reduce symptoms.
- Comfortable footwear — shoes with a wide toe box, low heel, and good fit help minimize forefoot irritation.
- Physical therapy — modalities such as laser therapy, ultrasound, or radiofrequency treatments may reduce pain. Gentle ankle range‑of‑motion exercises, Achilles tendon stretching, and strengthening of foot and lower‑leg muscles can support normal movement patterns.
- Pain relief medications — paracetamol and non‑steroidal anti‑inflammatory drugs (NSAIDs) such as ibuprofen may help reduce discomfort.
- Orthotic support — custom or prefabricated insoles can redistribute pressure away from the metatarsal heads. They are useful in conditions such as flat feet, pes cavus, or general forefoot overload.
Condition‑Specific Treatments
- Morton’s neuroma — foot orthotics or an ultrasound‑guided corticosteroid injection often relieve nerve‑related pain.
- Hallux valgus or hallux rigidus — footwear modification, padding, or orthotics may help; persistent deformities sometimes require surgical correction.
- Structural deformities or instability — targeted physical therapy, supportive footwear, or orthotic devices can improve comfort.
Surgical Options
Surgery is considered when conservative treatment does not provide sufficient relief or when a structural problem is clearly responsible for forefoot pain.
- Metatarsal osteotomy — shortening or repositioning a metatarsal bone to improve pressure distribution.
- Hallux valgus correction — reducing bunion deformity can relieve excess load on the lesser metatarsals.
- Soft‑tissue reconstruction — repairing ligaments or joint structures in cases of chronic instability or significant deformity.
When to See a Doctor
Forefoot pain is often manageable with home measures, but certain symptoms suggest that medical evaluation is needed.
- Severe pain — intense discomfort that limits walking or daily activities.
- Swelling or redness — may indicate inflammation, arthritis, or gout.
- Pain lasting longer than 2–3 weeks — persistent symptoms should be assessed by a clinician.
- Suspected fracture — sudden sharp pain after injury, difficulty weight‑bearing.
- Neuropathic symptoms — tingling, numbness, or burning may suggest nerve involvement such as Morton’s neuroma.
Prognosis
Most cases of metatarsalgia improve with conservative treatment, especially when footwear, activity patterns, and load distribution are addressed. Chronic or recurrent cases may require more structured interventions, including orthotics or targeted therapy. Surgery is rarely necessary and is reserved for situations where a clear structural problem continues to cause pain despite appropriate non‑surgical care.
FAQ – Metatarsalgia
1. What is metatarsalgia?
Metatarsalgia refers to pain in the ball of the foot, usually caused by increased pressure on the metatarsal heads.
2. Can metatarsalgia develop suddenly?
Yes — especially after intense activity, sudden training changes, or wearing tight shoes.
3. Is metatarsalgia the same as Morton’s neuroma?
No. Morton’s neuroma is a nerve condition, while metatarsalgia is a general term for forefoot pain. They can occur together.
4. Does footwear matter?
Absolutely. Shoes with a wide toe box and low heel reduce pressure on the forefoot and often relieve symptoms.
5. Can being overweight cause metatarsalgia?
Yes. Excess body weight increases pressure on the metatarsal heads and is a common contributing factor.
6. Are tingling or numbness typical symptoms?
Not usually. These symptoms more commonly suggest nerve irritation, such as Morton’s neuroma.
7. How long does recovery take?
Many patients improve within several weeks of conservative care, though structural causes may require longer treatment.
8. Can metatarsalgia return?
Yes — especially if underlying factors such as footwear, activity load, or deformities are not addressed.
Conclusion
Metatarsalgia is a common source of forefoot pain, often linked to increased pressure on the metatarsal heads. Most people improve with simple measures such as footwear changes, activity modification, and supportive insoles. Recognizing symptoms early and addressing contributing factors helps prevent chronic discomfort. If pain persists or is accompanied by swelling, redness, or nerve‑related symptoms, a medical evaluation is recommended to identify the underlying cause and guide appropriate treatment.
Besse JL. Metatarsalgia. Orthopaedics & Traumatology: Surgery & Research. 2017. Comprehensive review: Metatarsalgia classification, biomechanics, diagnosis, and treatment
An TW, Kish A, Varacallo M, Aiyer AA, Vulcano E. Metatarsalgia. In: Orthopedic Surgery Clerkship. Springer. 2017. Orthopedic textbook chapter: Clinical evaluation and management of metatarsalgia
Park CH, Chang MC. Forefoot Disorders and Conservative Treatment. Yeungnam University Journal of Medicine. 2019. Evidence-based review: Conservative treatment of forefoot disorders and metatarsalgia
Cooke R, Manning C, Palihawadana D, Zubairy AI, Khan SH. Metatarsalgia: Anatomy, Pathology and Management. British Journal of Hospital Medicine. 2021. Clinical review: Forefoot anatomy, causes of metatarsalgia, and current management strategies
Bardelli M, Turelli L, Scoccianti G. Definition and Classification of Metatarsalgia. Foot and Ankle Surgery. Foundational review: Definition, classification, and pathophysiology of metatarsalgia
Pelly T, Holme T, Tahir MA, Kunasingam K. Forefoot Pain. BMJ. 2020. BMJ clinical review: Assessment, differential diagnosis, and treatment of forefoot pain
















