

Cuboid syndrome is an underrecognized cause of lateral foot pain, particularly among runners. Although stress fractures, tendon pathology, and ligamentous injuries are more commonly considered, dysfunction of the cuboid bone can represent a clinically relevant and often overlooked diagnosis.
This condition involves a subtle disturbance in the mechanics of the cuboid bone, a small but biomechanically significant structure located on the lateral side of the midfoot. When its normal alignment or motion is disrupted—commonly following repetitive strain or an inversion-type ankle mechanism—it may result in pain, altered gait mechanics, and reduced running performance.
Cuboid syndrome remains frequently underdiagnosed, in part because it rarely presents with clear findings on imaging and can mimic other causes of lateral foot pain. For runners, this often translates into persistent symptoms, delayed diagnosis, and suboptimal management.
Key Clinical Points – Cuboid Syndrome
- Cuboid syndrome is a functional foot disorder and a recognized cause of lateral foot pain, particularly in runners.
- It involves dysfunction of the cuboid bone and the calcaneocuboid joint, leading to altered midfoot mechanics rather than structural damage.
- The condition is often associated with overuse, ankle inversion injuries, and training load errors.
- Symptoms typically include localized lateral midfoot pain, tenderness over the cuboid region, and pain during the push-off phase of running.
- Diagnosis is primarily clinical, as imaging is usually unremarkable and findings can mimic other foot pathologies.
- Management is conservative, combining manual therapy, taping, load modification, and strengthening exercises for optimal recovery and prevention of recurrence.
What Is Cuboid Syndrome?
Definition and clinical concept
Cuboid syndrome refers to a functional disturbance involving the cuboid bone, typically described as a loss of normal congruency or mobility at the calcaneocuboid joint. In clinical terms, it is not a clearly defined structural lesion but rather a mechanical dysfunction within the lateral column of the foot. This dysfunction may involve a subtle positional fault or altered arthrokinematics of the cuboid, leading to localized lateral foot pain and impaired load transfer during gait.
The cuboid plays a key role as a stabilizing structure and a pulley for the peroneus longus tendon, contributing to efficient force transmission during the push-off phase. Even minor disturbances in this region can therefore produce disproportionate symptoms, particularly in runners exposed to repetitive loading.
Functional vs structural pathology
A key feature of cuboid syndrome is that it is primarily considered a functional disorder rather than a structural injury. Unlike fractures, ligament tears, or overt joint dislocations, there is usually no visible damage on standard imaging. Instead, the pathology is thought to involve:
- Altered joint mechanics at the calcaneocuboid articulation
- Transient subluxation or positional fault of the cuboid
- Soft tissue contributions, including irritation of surrounding ligaments or the peroneal tendons
This distinction is clinically important. Because the issue is functional, symptoms can often respond rapidly to appropriate manual therapy and load modification—something less typical for true structural injuries.
Why it’s often missed
Cuboid syndrome is frequently overlooked due to its nonspecific presentation. Symptoms can mimic other causes of lateral foot pain, including stress fractures and tendon-related conditions.
In addition, imaging studies are typically normal, and there is no single definitive diagnostic test. As a result, the condition is often underrecognized—particularly in runners with persistent lateral foot pain that does not follow the expected course of more common injuries.
Anatomy and Biomechanics of the Cuboid Bone
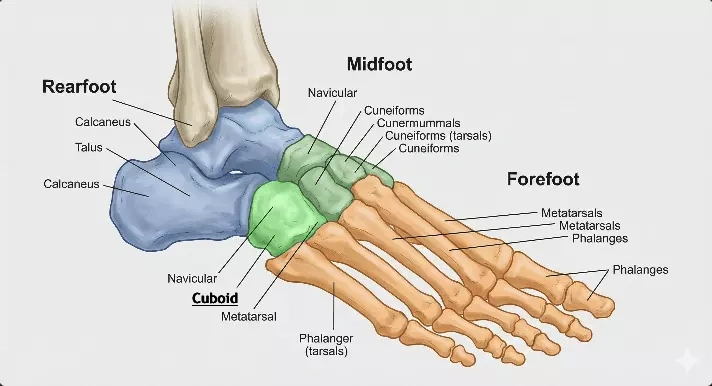
The cuboid bone is located on the lateral aspect of the midfoot, forming an important link between the hindfoot and forefoot. It articulates proximally with the calcaneus at the calcaneocuboid joint and distally with the fourth and fifth metatarsals, while also connecting medially with the lateral cuneiform and occasionally the navicular. This anatomical position places the cuboid at the center of the lateral column of the foot, where it contributes to both structural integrity and controlled mobility.
Functionally, the lateral column—comprising the calcaneus, cuboid, and lateral metatarsals—is designed to provide a balance between stability and adaptability. Unlike the more rigid medial column, which is optimized for propulsion, the lateral side allows the foot to accommodate uneven surfaces and absorb load during gait. Within this system, the cuboid serves as a mechanical bridge, facilitating efficient transfer of forces from the hindfoot to the forefoot, particularly during the transition from initial contact to push-off in running.
A key biomechanical feature of the cuboid is its interaction with the peroneus longus tendon, which passes through a groove on its plantar surface. In this role, the cuboid acts as a pulley, optimizing tendon function and contributing to stabilization of the foot during dynamic activities. This relationship is especially relevant in runners, where repetitive loading places continuous demand on lateral foot structures.
Disruption of normal cuboid mechanics—even if subtle—can alter load distribution and affect overall midfoot function. These changes may contribute to inefficient gait patterns and are often associated with the development of lateral foot pain, highlighting the clinical importance of this small but functionally significant structure.
Causes and Risk Factors for Cuboid Syndrome
Cuboid syndrome is typically multifactorial, with contributing factors related to training load, injury mechanisms, and individual biomechanics. In runners, the condition often develops in the context of repetitive stress applied to the lateral column of the foot.
- Overuse and training errors
Sudden increases in running volume, intensity, or frequency can overload the lateral foot structures. This is particularly relevant during marathon preparation or return-to-running phases, where cumulative stress may exceed tissue capacity. - Ankle inversion injuries
A common mechanism involves a prior ankle sprain, especially involving inversion. Even mild injuries can disrupt the normal mechanics of the cuboid bone, leading to persistent dysfunction despite apparent recovery. - Biomechanical predispositions
Certain foot mechanics may increase susceptibility, including overpronation, excessive foot mobility, or conversely, a relatively stiff lateral column. These factors can alter load distribution and place additional stress on the cuboid region. - Footwear factors
Worn-out running shoes, inadequate lateral support, or abrupt changes in footwear (e.g. transitioning to minimalist shoes) may contribute to altered foot mechanics and increased strain on the lateral midfoot. - Running surface and terrain
Uneven terrain, cambered roads, and trail running can increase lateral loading of the foot, particularly over longer distances. This may predispose runners to developing lateral foot pain associated with cuboid dysfunction. - Interaction with peroneal tendons
Increased tension or dysfunction in the peroneal tendons may influence cuboid mechanics, given their close anatomical and functional relationship.
In most cases, cuboid syndrome does not arise from a single cause but rather from a combination of these factors, making a thorough clinical assessment essential for identifying the primary contributors.
Symptoms: Recognizing Cuboid Syndrome
The clinical presentation of cuboid syndrome is often subtle and can easily be mistaken for other causes of lateral foot pain, particularly in runners. Symptoms are typically activity-related and tend to worsen with continued loading.
A key feature is lateral foot pain, which is usually localized to the midfoot region on the outer side of the foot. Patients often describe a deep, aching, or sometimes sharp discomfort rather than a clearly defined point of injury. The pain may be intermittent at first but can become more persistent with ongoing training.
Common clinical findings include:
- Pain during the push-off phase of running
Symptoms are often most noticeable during propulsion, when the cuboid and peroneus longus complex are under increased mechanical demand. - Tenderness over the cuboid region
Palpation of the dorsal or plantar aspect of the cuboid bone typically reproduces symptoms. This localized tenderness is an important clinical clue, especially when imaging is unremarkable. - Functional limitations and gait changes
Runners may unconsciously alter their gait to offload the lateral foot. This can manifest as reduced push-off strength, shortened stride length, or a subtle shift in weight-bearing mechanics to the medial side of the foot.
In some cases, patients also report a sensation of “something being out of place” in the foot, although this is not consistently present. Importantly, symptoms often fluctuate with activity level, improving with rest and worsening with return to running.
Overall, the symptom pattern is typically mechanical in nature, closely linked to loading and movement, which helps distinguish cuboid syndrome from more static or inflammatory conditions.
Other Conditions That Can Mimic Cuboid Syndrome
Several musculoskeletal conditions can present with similar symptoms to cuboid syndrome, particularly in athletes and runners with lateral foot pain. Because clinical findings often overlap, careful differential diagnosis is essential.
- Stress fractures (5th metatarsal)
A common overuse injury in runners, typically presenting with more focal, bony tenderness and pain that worsens progressively with impact loading. - Peroneal tendinopathy
Characterized by pain along the course of the peroneal tendons, often aggravated by resisted eversion and repetitive loading. Unlike cuboid syndrome, symptoms are usually more posterior and tendon-focused. - Lisfranc injuries
Involve the tarsometatarsal joints and may present with midfoot pain, swelling, and difficulty bearing weight. These injuries are generally more acute and functionally limiting. - Sinus tarsi syndrome
Presents with pain on the anterolateral aspect of the hindfoot, often associated with a feeling of instability, particularly on uneven terrain.
Although these conditions differ in pathology, their clinical presentation can overlap significantly with cuboid-related pain. This is particularly true in runners, where repetitive loading patterns can blur the clinical picture, making thorough assessment and localization of symptoms critical for accurate diagnosis.
Diagnosis
Diagnosis of cuboid syndrome is primarily clinical and relies on a combination of patient history and targeted physical examination. A detailed history often reveals a recent increase in running load or a preceding inversion-type ankle injury associated with the onset of lateral foot pain.
Clinical examination typically focuses on localized tenderness over the cuboid region and reproduction of symptoms with palpation or midfoot manipulation. Functional testing may reveal pain during weight-bearing activities, particularly during push-off in gait. Imaging is often inconclusive, as standard radiographs, ultrasound, or MRI usually fail to demonstrate specific abnormalities, reinforcing the importance of clinical assessment.
Cuboid Syndrome Treatment Options
Management of cuboid syndrome is primarily conservative and focuses on restoring normal mechanics of the lateral foot while addressing contributing load and biomechanical factors. In most cases, symptoms can improve relatively quickly when appropriate interventions are applied.
- Manual therapy (cuboid manipulation)
A commonly used approach involves targeted mobilization or manipulation of the cuboid bone to restore normal joint alignment and reduce lateral foot pain. When indicated, this can produce rapid symptom relief, although it should always be combined with load management. - Taping techniques
Taping the lateral midfoot can provide short-term support to the cuboid region, helping to stabilize the area during walking and running while symptoms settle. - Load management and activity modification
Reducing running volume, intensity, or impact loading is often essential in the early phase. Temporary substitution with low-impact activities can help maintain fitness without aggravating symptoms. - Strengthening and mobility work
Rehabilitation should address intrinsic foot strength, calf complex function, and peroneal muscle control. Improving overall foot and ankle mobility and stability reduces recurrence risk and supports gradual return to running. - Padding and offloading support. Padding placed beneath the plantar aspect of the cuboid is commonly recommended in cuboid syndrome. The pad is typically positioned under the medial portion of the cuboid and adjusted in thickness (approximately 3–6 mm) to help prevent excessive cuboid eversion during weight-bearing activities.
- Lateral wedge placed under the calcaneus may also be used to modify hindfoot loading and reduce lateral foot pain during walking and running.
Overall, treatment is most effective when manual techniques are combined with structured load progression and corrective exercise, rather than used in isolation.
Return to Running
Return to running should be criteria-based rather than time-based, with progression guided by symptom response and load tolerance.
- Gradual progression strategies
Running should be reintroduced in a stepwise manner, starting with short, low-intensity intervals and gradually increasing volume before intensity. - Monitoring symptoms
Mild transient discomfort may be acceptable, but increasing lateral foot pain during or after running indicates excessive load and requires regression. - Preventing recurrence
Addressing contributing factors such as biomechanics, training errors, and footwear is essential to avoid recurrence of cuboid syndrome during return to full training.
Prevention Strategies
Preventing cuboid syndrome in runners focuses on optimizing load management and improving foot and ankle resilience. Appropriate running shoes with adequate lateral support and shock absorption may help reduce excessive stress on the cuboid region. Gradual increases in mileage and training intensity are essential, as sudden spikes in load remain one of the most important risk factors for lateral foot pain.
In addition, targeted strength and conditioning—particularly of the intrinsic foot muscles, calf complex, and peroneal musculature—can improve load distribution and enhance midfoot stability.
Key Takeaways
Cuboid syndrome is an underrecognized but clinically relevant cause of lateral foot pain, particularly in runners. It is primarily a functional condition involving the cuboid bone and its role in lateral foot biomechanics.
Diagnosis is largely clinical, as imaging is typically normal and symptoms can mimic other pathologies such as stress fractures or peroneal tendinopathy. Early recognition is important to avoid prolonged symptoms and unnecessary investigations.
Management is conservative and includes manual therapy, taping, load modification, and progressive strengthening. Addressing underlying biomechanical and training-related factors is essential for successful recovery and prevention of recurrence.
Durall CJ. Examination and treatment of cuboid syndrome: a literature review. Sports Health. 2011 Nov;3(6):514-9. PubMed: Cuboid syndrome examination and treatment review
Patterson SM. Cuboid syndrome: a review of the literature. Journal of Sports Science & Medicine. 2006 Dec 15;5(4):597-606. PMC: Review of cuboid syndrome literature
Newell SG, Woodle A. Cuboid Syndrome. Physician and Sportsmedicine. 1981 Apr;9(4):71-76. Journal article: Clinical description of cuboid syndrome
Gill M, Vilella RC. Foot Cuboid Bone Anatomy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026. StatPearls: Cuboid bone anatomy and function

















