

Plantar fasciitis is the leading cause of heel pain in adults and one of the most frequent musculoskeletal conditions of the foot encountered in clinical practice. It is a condition characterized by degenerative irritation of the plantar fascia at its attachment to the heel bone, most often as a result of repetitive mechanical overload.
Although the term suggests inflammation, current evidence shows that plantar fasciitis is, in most cases, a degenerative rather than an inflammatory condition. It is frequently confused with a heel spur, even though a spur is usually only an accompanying finding and not the true source of pain.
Plantar fasciitis most commonly occurs between the ages of 40 and 60, affecting both physically active and sedentary individuals, with a slightly higher prevalence in women.
In this article, you will learn what plantar fasciitis is, why it develops, the key risk factors and symptoms, how it is diagnosed, and which treatment options are supported by current clinical practice.
Key Clinical Points – Plantar Fasciitis
- Plantar fasciitis is the most common cause of heel pain and is primarily a degenerative overuse condition of the plantar fascia.
- The condition results from repetitive mechanical overload at the plantar fascia insertion on the calcaneus, leading to microtrauma and tissue degeneration.
- The hallmark symptom is sharp heel pain, typically worst with the first steps in the morning or after periods of rest.
- Diagnosis is mainly clinical, based on history and physical examination; imaging is used only to exclude other causes of heel pain.
- First-line treatment includes activity modification, footwear changes, stretching exercises, and orthotic support.
- Most patients improve with conservative treatment within 6–12 months, although symptoms may persist longer in chronic cases.
What is plantar fasciitis?
Plantar fasciitis is a degenerative overuse condition affecting the plantar fascia at its insertion on the calcaneus (heel bone). It is most commonly caused by repetitive mechanical stress rather than a single traumatic event.
Although traditionally described as an inflammatory disorder, current evidence shows that plantar fasciitis is primarily a degenerative process involving microtears, collagen degeneration, and failed tissue repair at the fascia–bone interface.
Plantar fascia – structure and function
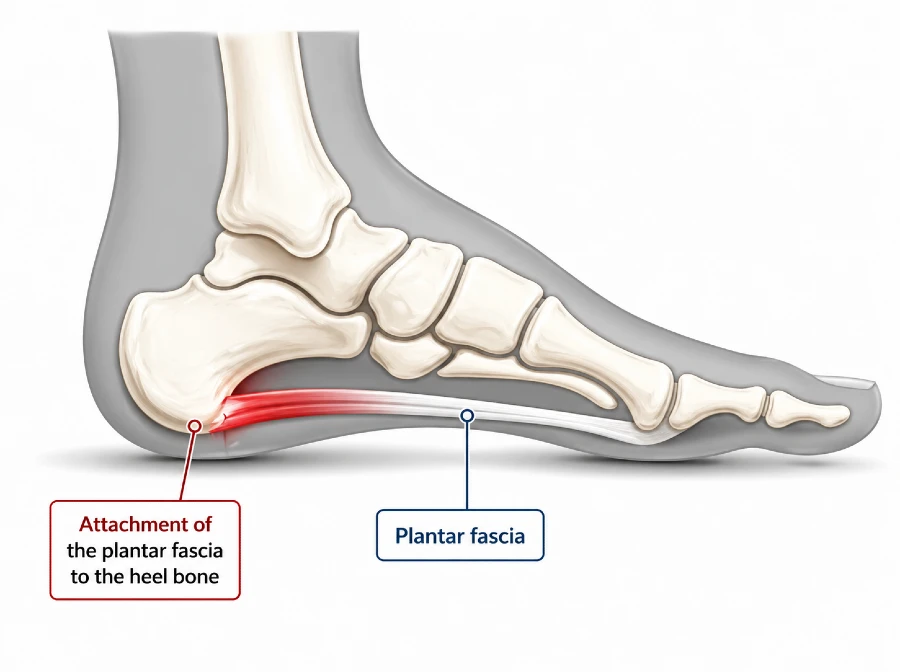
The plantar fascia is a strong, fibrous band of connective tissue located on the underside of the foot. It is anatomically designed to withstand high mechanical loads during standing, walking, and running.
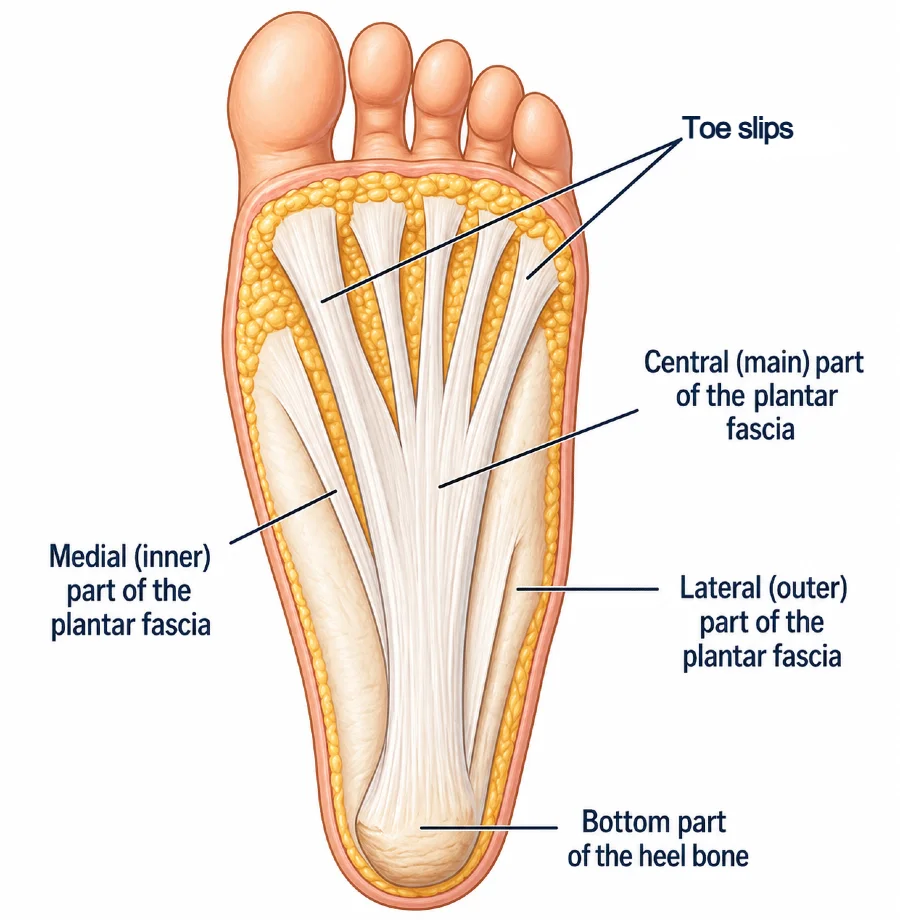
It originates from the inferior aspect of the calcaneus (heel bone) and extends forward toward the forefoot, where it fans out and attaches to the bases of the toes through multiple fibrous bands.
The central portion of the plantar fascia is the thickest and strongest, playing the key role in maintaining the longitudinal arch of the foot. The medial and lateral portions are thinner and follow the natural contour of the foot.
Function of the plantar fascia
Functionally, the plantar fascia plays a crucial role in supporting the arch of the foot and absorbing mechanical stress. With every step, it helps distribute load away from bones, joints, and muscles.
During gait—especially in the push-off phase—it acts like a spring, storing and releasing elastic energy. This mechanism improves movement efficiency and contributes to stable, energy-efficient walking and running.
Why this structure is prone to injury
Due to its essential biomechanical role and constant exposure to repetitive stress, the plantar fascia is highly susceptible to overuse and microtrauma. Over time, this repetitive loading can lead to degenerative changes, which are the underlying cause of plantar fasciitis.
What causes plantar fasciitis?
Plantar fasciitis most commonly develops as a result of repetitive mechanical overload that exceeds the tissue’s ability to recover.
With every step, especially during heel strike, the plantar fascia is exposed to significant mechanical stress. When this stress becomes excessive or repetitive—such as during prolonged standing, increased body weight, improper footwear, or changes in physical activity—it can lead to microtears in the tissue. Over time, these small injuries accumulate and result in a degenerative process, which is responsible for heel pain and tissue sensitivity.
Key risk factors
Not everyone exposed to mechanical stress will develop symptoms. Certain factors significantly increase the likelihood of plantar fasciitis:
- Increased mechanical load
Sudden increases in activity level, intensive running or jumping, prolonged standing, or heavy physical work can overload the plantar fascia. - Foot biomechanics
Structural variations such as flat feet (pes planus), high arches (pes cavus), or excessive pronation alter load distribution and increase strain on the fascia. - Muscle tightness and imbalance
Tight calf muscles (gastrocnemius and soleus) reduce ankle mobility and increase stress on the heel and plantar fascia. - Inappropriate footwear
Shoes with minimal cushioning or support, as well as flat footwear such as ballet flats, canvas sneakers, or worn-out running shoes, can increase fascial strain. - Body weight
Increased body weight leads to higher repetitive load on the foot with every step, increasing the risk of microinjury. - Age-related changes
With aging, the plantar fascia loses elasticity and becomes less resistant to stress, increasing susceptibility to injury. - Changes in activity patterns
Sudden changes in sport type, intensity, or training volume are a common trigger, especially when progression is too rapid.
Who is most likely to develop plantar fasciitis?
Plantar fasciitis is not limited to athletes or individuals with physically demanding occupations. Although repetitive physical activity increases the risk, the condition can affect a wide range of people, including runners, dancers, office workers, and individuals with low levels of physical activity. Epidemiological data suggest that it accounts for approximately 10–15% of all foot-related complaints, while up to 22% of runners may experience symptoms during their lifetime.
The condition most commonly occurs between the ages of 40 and 60 and is slightly more frequent in women. In about one-third of cases, symptoms are present in both feet, indicating that plantar fasciitis is often a bilateral overuse condition rather than an isolated injury.
Excess body weight increases mechanical stress on the plantar fascia, making the condition more common in individuals with higher body mass. In combination with age-related changes, footwear choices, and daily activity patterns, even small lifestyle factors can significantly influence the overall load on the foot and contribute to symptom development.
What are the symptoms of plantar fasciitis?
Symptoms of plantar fasciitis typically develop gradually and without a clear triggering injury. The condition most often presents as a characteristic pattern of heel pain related to load-bearing and periods of rest.
The main clinical features include:
- Sharp pain in the heel, most commonly located on the bottom or inner side
- Pain with the first steps in the morning, often described as the most intense symptom
- Pain after periods of rest, such as sitting or lying down for a longer time
- Temporary improvement with movement, followed by recurrence with prolonged walking, standing, or running
- Local tenderness at the inner heel, where the plantar fascia attaches to the calcaneus
- Occasional radiation of pain along the inner arch of the foot
A characteristic feature of plantar fasciitis is that symptoms are typically most pronounced during the first steps after rest, especially in the morning, and may partially ease with light activity before worsening again with continued loading throughout the day.
Diagnosis
The diagnosis of plantar fasciitis is primarily based on a combination of clinical history and physical examination. In most cases, a specialist evaluates the duration, pattern, and characteristics of heel pain, along with potential contributing risk factors.
A key part of the assessment includes gait analysis, which helps identify biomechanical abnormalities such as excessive foot pronation and reduced muscle strength. Physical examination typically involves palpation of the heel bone and specific tests that reproduce the patient’s pain at the site of plantar fascia insertion.
Plantar fasciitis is, in most cases, a clinical diagnosis, and additional imaging studies are not routinely required. However, when the clinical presentation is unclear or when alternative diagnoses are suspected, imaging such as X-ray or ultrasound may be indicated.
X-ray imaging cannot directly confirm plantar fasciitis because it does not visualize soft tissues like the plantar fascia. It is mainly used to exclude other causes of heel pain, such as stress fractures or degenerative joint changes. A heel spur is often visible on X-rays, but in most cases it represents an incidental finding rather than the true source of pain.
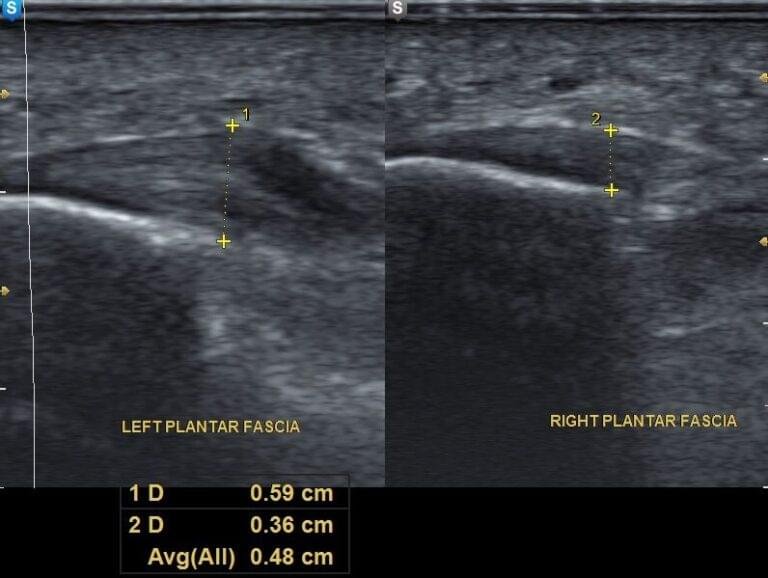
Ultrasound is a highly useful diagnostic tool for evaluating soft tissue structures of the foot. It can demonstrate thickening of the plantar fascia, local swelling, and calcifications at its attachment to the calcaneus, as well as monitor changes during treatment.
Plantar Fasciitis Treatment – What actually works?
The treatment of plantar fasciitis depends on symptom severity and individual patient factors. In most cases, management begins with conservative, non-invasive approaches.
The primary goal of treatment is to reduce pain and address the underlying biomechanical factors that contribute to tissue overload. Even with appropriate therapy, symptom resolution may take several weeks or months. During this period, patients often need to temporarily reduce or modify high-impact physical activities.
Current evidence-based recommendations support a stepwise approach to management, although in clinical practice treatment is always individualized and elements from later stages may be introduced earlier when necessary.
| Treatment level | Main interventions | Clinical goal |
|---|---|---|
| First-line treatment | Activity modification, footwear changes, orthotic insoles, plantar fasciitis exercises and stretches, ice, weight management, NSAIDs | Reduce mechanical overload and pain, promote tissue recovery |
| Second-line treatment | Night splints, physical therapy (strengthening + manual therapy), shockwave therapy (ESWT) | Reduce persistent pain, improve function and tissue healing |
| Third-line treatment | Corticosteroid injections, dextrose prolotherapy, PRP injections | Target chronic degenerative changes and stimulate regeneration |
| Surgical treatment | Gastrocnemius lengthening, partial plantar fascia release (fasciotomy) | Last-resort option to reduce tension and improve biomechanics |
First-line treatment – what to start immediately
In the majority of cases, symptoms can be significantly improved with basic conservative measures applied consistently over a period of approximately six weeks. These interventions are often used in combination and can be performed at home.
First-line treatment for plantar fasciitis:
Activity modification and load reduction
The first and most important step is reducing mechanical load on the plantar fascia. This does not require complete rest, but rather avoidance of activities that trigger pain, such as prolonged standing, walking on hard surfaces, running, and jumping. Athletically active individuals are advised to temporarily modify training and gradually return to activity based on symptom response.
Footwear modification
Footwear plays a central role in reducing stress on the plantar fascia. Shoes with a firm but cushioned sole, adequate arch support, and a stable heel counter are recommended.
Flat and minimally cushioned footwear—such as ballet flats, canvas shoes, or court-style sneakers—should be avoided, as well as walking barefoot on hard surfaces. Worn-out footwear should be replaced promptly. In some cases, rocker-bottom shoes may provide additional symptom relief.
From a practical standpoint, wearing well-cushioned running shoes during daily activities is often a simple yet highly effective intervention.
Orthotic insoles and heel cushions
Orthotic insoles help reduce load on the plantar fascia by supporting the medial longitudinal arch. They may be prefabricated or custom-made depending on foot morphology and biomechanical needs. Their function includes correcting excessive pronation and improving load distribution across the foot.
Silicone heel pads provide additional shock absorption and reduce direct pressure on the heel. However, insoles should always be used as part of a broader treatment strategy rather than as a standalone therapy.
Stretching exercises
Reduced flexibility of the calf muscles and Achilles tendon is a key risk factor for plantar fasciitis. Stretching exercises therefore represent an essential component of treatment.
Stretching of the gastrocnemius is performed with an extended knee, while soleus stretching is done with a flexed knee. Combining both techniques ensures balanced flexibility of the entire posterior chain of the lower leg.
Targeted stretching of the plantar fascia itself can be performed manually by pulling the toes toward the body or by rolling the foot over a small ball. These techniques reduce fascial tension and often provide rapid symptom relief, particularly in the morning.
Regular daily exercise, ideally performed multiple times per day, is recommended for optimal results.
Adjunctive measures: ice, body weight, and medication
Local ice application to the heel for 5–10 minutes may reduce pain and hypersensitivity, particularly during symptom flare-ups.
Maintaining a healthy body weight is important, as excess weight increases mechanical stress on the plantar fascia with every step.
Non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen or diclofenac, may be used short-term for pain control. Their use should be limited to the lowest effective dose for the shortest possible duration.
Second-line treatment – when first-line measures are not sufficient
If symptoms persist despite consistent conservative treatment for approximately six weeks, additional therapeutic options are considered. These interventions are typically performed under the supervision of a physiatrist and aim to reduce pain, improve function, and promote tissue healing.
Second-line treatment for plantar fasciitis:
1. Plantar Fasciitis Night Splints
Night splints are prefabricated or custom-made orthoses designed to maintain the ankle in a neutral position during sleep, preventing plantar flexion. During sleep, the foot naturally rests in plantar flexion, which leads to shortening of the plantar fascia and Achilles tendon.
By keeping the foot at approximately 90 degrees relative to the lower leg, night splints reduce nocturnal tightening of soft tissues. This decreases tension on the plantar fascia and significantly reduces the characteristic morning heel pain.
Night splints are particularly effective for patients who experience severe pain with the first steps in the morning. They are typically used daily for a period of 1 to 3 months, depending on symptom severity and clinical response.
2. Physical therapy for plantar fasciitis
In many cases, plantar fasciitis is not only a local tissue problem but also a result of altered biomechanics of the foot and lower limb. Weakness of the intrinsic foot muscles and calf musculature, combined with impaired movement control, can lead to increased stress on the plantar fascia.
For example, excessive foot pronation is often associated with weakness of the tibialis posterior muscle, further increasing mechanical load on the plantar fascia.
Physical therapy therefore includes not only stretching exercises, but also progressive strengthening of the foot and calf muscles, particularly the posterior chain. The goal is to improve foot stability, normalize gait mechanics, and reduce recurrence risk.
Common physiotherapy modalities include:
- Laser therapy, used as an adjunct in both acute and chronic cases (typically 3–5 sessions per week for ~3 weeks)
- Phonophoresis, where ultrasound enhances transdermal delivery of NSAID gels (e.g., ibuprofen, diclofenac, ketoprofen)
- Electrotherapy (TENS, interferential currents) for pain modulation, although clinical evidence remains limited
- Therapeutic ultrasound, which lacks strong evidence for routine use in plantar fasciitis
- Manual therapy, including joint mobilization and soft tissue techniques to reduce pain and improve mobility
3. Shockwave therapy (ESWT)

Extracorporeal shockwave therapy (ESWT) plays a key role in second-line management. It is often introduced after failure of standard physiotherapy, although some clinicians use it earlier in the treatment pathway.
Shockwave therapy uses high-energy acoustic waves delivered via a handheld applicator applied directly to the skin over the affected area. It is used in both acute and chronic plantar fasciitis as a non-invasive method to stimulate tissue regeneration and reduce pain.
Clinical studies report improvement rates of approximately 45–80%, with both short- and long-term benefits. Although the exact mechanism is not fully understood, proposed effects include neovascularization, neuromodulation, and increased cellular permeability, all of which may enhance tissue healing.
Treatment is usually performed once weekly for 3–5 weeks. Some patients experience improvement after the first session, although most notice significant benefit after the second or third treatment. The procedure is generally safe but may cause temporary discomfort during application.
Third-line treatment – advanced and regenerative options
If symptoms of plantar fasciitis fail to improve despite well-conducted first- and second-line conservative treatment, more advanced and targeted interventions may be considered. These therapies are typically performed by a physician and include various injection-based and regenerative approaches.
Third-line treatment for plantar fasciitis:
1. Corticosteroid injections
Corticosteroids are potent anti-inflammatory medications that have been widely used in the management of plantar fasciitis to reduce pain and local irritation. Although traditionally considered anti-inflammatory agents, current evidence suggests that chronic plantar fasciitis is not primarily an inflammatory condition. Their beneficial effect is therefore likely related to modulation of local tissue activity and pain pathways rather than true anti-inflammatory action.
Injections are usually performed under ultrasound guidance to ensure precise placement at the site of maximal pathology. They are most effective when used as part of a broader treatment plan rather than as a standalone therapy. The duration of symptom relief varies significantly, ranging from several weeks to several months.
Potential risks include plantar fascia rupture and fat pad atrophy of the heel, which is why corticosteroid injections should be used cautiously and in the lowest effective dose.
2. Dextrose prolotherapy
Dextrose prolotherapy is a regenerative injection technique used in the treatment of chronic musculoskeletal pain conditions, including plantar fasciitis. Under ultrasound guidance, a concentrated dextrose solution (typically 15–20%) is injected into the affected tissue.
The proposed mechanism involves a local healing response that stimulates tissue repair and strengthens the affected enthesis (tendon-bone junction). Clinical studies suggest that its effectiveness is comparable to shockwave therapy, with a favourable safety profile and minimal adverse effects.
Treatment is usually performed as a series of 1 to 3 injections, spaced 7–14 days apart.
3. Platelet-rich plasma (PRP) therapy
Platelet-rich plasma (PRP) is a regenerative treatment that uses a concentrated preparation of the patient’s own platelets, injected into the affected area of the plantar fascia. PRP contains growth factors that may promote tissue healing and modulate chronic degenerative changes.
Compared to corticosteroid injections, PRP has shown promising results and may provide comparable or potentially superior outcomes in some studies particularly in chronic cases, without the associated risk of tissue weakening. Reported clinical benefits can last up to one year in some patients.
PRP is typically administered under ultrasound guidance in a series of three injections, usually spaced one week apart.
Surgical treatment of plantar fasciitis
Surgical treatment is considered a last-resort option for chronic plantar fasciitis, reserved for cases in which prolonged and well-conducted conservative and minimally invasive treatments have failed to provide adequate symptom relief.
It is important to emphasize that surgery does not guarantee complete resolution of symptoms and carries potential risks. Possible complications include nerve injury, plantar fascia rupture, and flattening of the medial longitudinal arch of the foot, which may result in persistent functional impairment.
In clinical practice, two main surgical approaches are most commonly used, either alone or in combination:
1. Gastrocnemius muscle lengthening
Tightness of the calf muscles increases mechanical load on the plantar fascia. Gastrocnemius lengthening is indicated in patients with persistent restriction of ankle dorsiflexion despite adequate and prolonged stretching therapy.
By surgically lengthening the calf muscle, ankle mobility is improved, which reduces excessive strain on the plantar fascia during walking and weight-bearing activities.
2. Partial plantar fascia release (fasciotomy)
Partial fasciotomy involves releasing a portion of the plantar fascia at its attachment to the calcaneus in order to reduce excessive tension within the tissue. This procedure is often combined with gastrocnemius lengthening in selected cases.
If a prominent heel spur is present, it may be removed during the same surgical procedure, although it is not typically the primary source of pain.
Given the potential complications and unpredictable outcomes, the decision to proceed with surgery should be made cautiously and only after all other treatment options have been thoroughly exhausted.
Frequently Asked Questions
1. I have plantar fasciitis – what can I expect?
Although treatment can be prolonged and sometimes frustrating, the overall prognosis is good. Symptoms may last from several weeks to several months, and in some cases longer. However, most patients experience significant improvement within 6 to 12 months with appropriate management. Consistency in treatment and load modification are key factors in recovery.
2. Can plantar fasciitis be prevented?
In many cases, the risk can be significantly reduced with proper habits:
- wearing supportive footwear with good arch support
- regular stretching of the calf and foot (plantar fasciitis stretches)
- gradual increase in training load
- proper warm-up before activity
- maintaining a healthy body weight
- early response to heel pain
3. Is plantar fasciitis a serious condition?
It is not considered a serious or dangerous condition, but it can significantly affect quality of life. Persistent heel pain may limit walking, work, and sports activities, and without treatment, symptoms can become chronic.
4. How long does recovery take?
Recovery varies between individuals. Some patients improve within a few weeks, while others may experience symptoms for several months. With appropriate treatment, most patients achieve significant improvement within 6–12 months.
5. Can I exercise or run with plantar fasciitis?
During the acute phase, activities that provoke pain—especially running and jumping—should be reduced or temporarily avoided. Pain-free activities are generally allowed, and return to sport should be gradual and symptom-guided.
6. Is a heel spur the cause of plantar fasciitis?
No. A heel spur is often an incidental radiographic finding. Pain in plantar fasciitis is caused by degenerative changes in the plantar fascia itself, not by the bony spur.
7. When should I see a doctor?
If heel pain persists for more than a few weeks, progressively worsens, or interferes with daily activities, a medical evaluation is recommended. Early treatment can shorten symptom duration and reduce the risk of chronic pain.
Lemont H, Ammirati KM, Usen N. Plantar fasciitis: a degenerative process (fasciosis) without inflammation. Journal of the American Podiatric Medical Association. DOI: 10.7547/87507315-93-3-234 – Degenerative nature of plantar fasciitis
Allam AE, Chang KV. Plantar Heel Pain. StatPearls [Internet]. NCBI StatPearls: Clinical overview of plantar heel pain
Martin RL, Davenport TE, Reischl SF, et al. Heel Pain–Plantar Fasciitis: Revision 2014 Clinical Practice Guidelines. Journal of Orthopaedic & Sports Physical Therapy. JOSPT guideline: Evidence-based management of plantar fasciitis
Thomas JL, Christensen JC, Kravitz SR, et al. The diagnosis and treatment of heel pain: a clinical practice guideline (revision 2010). Journal of Foot & Ankle Surgery. Clinical guideline: Diagnosis and management of heel pain
Morrissey D, Cotchett M, Said J’Bari A, et al. Management of plantar heel pain: a best practice guide. British Journal of Sports Medicine. Best practice guide: Evidence-based treatment of plantar heel pain
Modern Foot & Ankle. Heel Spur vs Plantar Fasciitis. Educational review: Heel spur and plantar fasciitis differences

















