

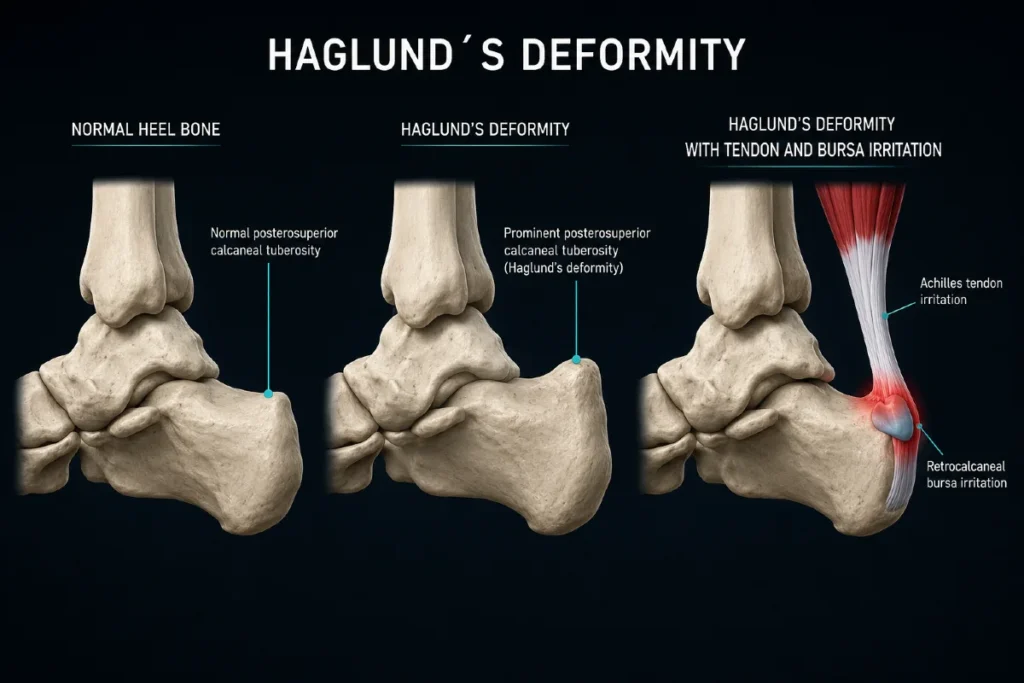
Haglund’s deformity is a bony prominence on the upper back part of the heel bone. When this prominence irritates the surrounding soft tissues, it creates a visible and painful swelling known as a pump bump. Although the terms are often used interchangeably, they describe different things: the deformity refers to the bone, while the pump bump refers to the external lump caused by bone and inflamed tissues.
This condition most often affects adults in mid‑life and is more common in women, especially those who wear shoes with a stiff heel counter. Mechanical irritation from footwear can inflame the retrocalcaneal bursa, the superficial bursa, and even the Achilles tendon insertion. Typical symptoms include pain at the back of the heel, a firm bump that becomes irritated in shoes, and localized redness or swelling.
In this article, we explain what Haglund’s deformity is, why the pump bump develops, and how to diagnose and treat this common source of heel pain.
Key Clinical Points – Haglund’s Deformity
- Haglund’s deformity is a clinical condition often referred to as a “pump bump” in everyday language, caused by a bony enlargement on the posterosuperior calcaneus.
- The condition commonly presents with heel pain, swelling, and irritation from footwear, especially shoes with a stiff heel counter.
- It is frequently associated with high arches, tight Achilles tendon, and repetitive mechanical stress.
- Diagnosis is based on clinical examination and lateral X‑ray showing the characteristic bony prominence.
- Conservative treatment includes footwear modification, heel lifts, physiotherapy, NSAIDs, and activity adjustment.
- Surgery is considered only when symptoms persist despite prolonged non‑operative management.
What Is Haglund’s Deformity and What Is a Pump Bump?
Haglund’s deformity is a bony prominence on the upper back part of the heel bone (posterior–superior calcaneus). It is a structural change of the bone itself and is clearly visible on X‑ray. The prominence sits exactly where shoes often press against the heel, making it prone to irritation.
The term pump bump refers to the external, visible swelling at the back of the heel. It is not the bone itself, but the clinical appearance created by the bony prominence plus inflamed soft tissues — most commonly the retrocalcaneal bursa, superficial bursa, and the Achilles tendon insertion. The name comes from classic women’s “pump” shoes, whose stiff heel counter often triggered this painful bump.
Although the two terms are often used interchangeably, they describe different components of the same problem:
- Haglund’s deformity — the bone (true anatomical prominence)
- Pump bump — the visible lump caused by bone + irritated soft tissues
This distinction matters because symptoms arise not from the bone alone, but from mechanical irritation of the surrounding tissues — especially in shoes with a stiff or tight heel counter.
Causes of Haglund’s Deformity
Haglund’s deformity develops when the upper back edge of the heel bone is repeatedly exposed to pressure, friction, or abnormal loading. Although the condition was historically linked to women’s pump shoes, the deformity can form with any footwear that is tight, rigid, or has a stiff heel counter.
This includes men’s dress shoes, work boots, ice‑skating boots, and ski boots. A hard heel counter that presses against the back of the heel during walking or activity creates constant mechanical stress, which stimulates the bone to thicken and form a prominence.
Several factors increase the likelihood of developing Haglund’s deformity by altering heel mechanics or increasing tension on the Achilles tendon:
- Genetic foot structure — some people naturally have a heel shape that predisposes them to bony prominence formation.
- High arches — a high‑arched foot tilts the heel backward, increasing pressure on the Achilles insertion.
- Tight Achilles tendon — excessive tension pulls the heel upward and increases friction against footwear.
- Walking on the outer heel — this gait pattern wears down the outer sole and rotates the heel inward, increasing irritation.
- Increased body weight — adds load to the heel and Achilles complex.
- Improper or tight shoes — especially those with a rigid heel counter.
- Overuse in runners — repetitive uphill running or high‑volume training increases compression and traction forces.
- Altered foot biomechanics — such as a shifted subtalar joint position.
The presence of the bony deformity does not automatically cause symptoms. Pain develops when the prominence irritates surrounding soft tissues, including the retrocalcaneal bursa, superficial bursa, Achilles tendon insertion, and the protective fat pad.
This combination of bone and soft‑tissue inflammation is what produces the painful pump bump.

Symptoms of Haglund’s Deformity and the Pump Bump
Symptoms do not come from the bony prominence alone. Many people have Haglund’s deformity without any pain. Problems begin when the prominence irritates the surrounding soft tissues — the bursae, the Achilles tendon insertion, and the overlying skin. This combination creates the painful, swollen pump bump, and symptoms often appear on both heels.
Key symptoms include:
- Visible bump on the back of the heel — a firm, well‑defined prominence that becomes irritated in shoes.
- Pain at the Achilles insertion — discomfort at the point where the Achilles tendon attaches to the heel bone, worse with walking, running, or uphill activity.
- Swelling behind the heel — soft‑tissue inflammation around the bony prominence.
- Redness and warmth — especially around the irritated bump, indicating active inflammation.
- Pain with pressure — symptoms worsen when stiff or tight shoes press on the area.

Diagnosis
Diagnosis is based on a combination of medical history, clinical examination, and imaging. Patients typically report pain and swelling at the back of the heel, especially when starting activity after rest or during longer walks. During the exam, the clinician looks for risk factors such as a high‑arched foot, tight Achilles tendon, or altered heel mechanics. A tender, warm, or visibly swollen bump on the back of the heel is a common finding.
Imaging Methods Used in Diagnosis
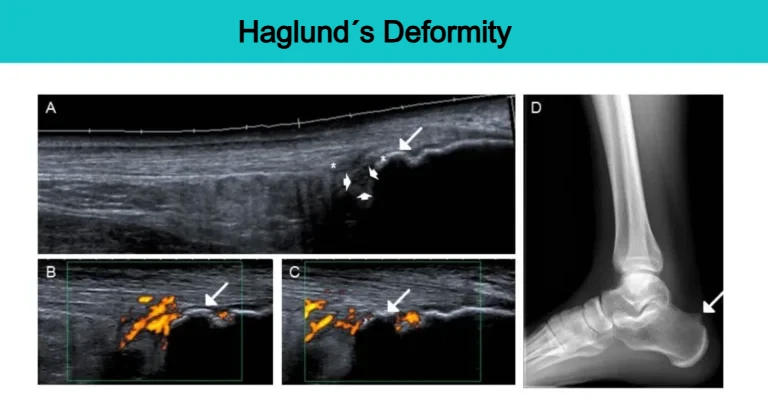
- X‑ray — A lateral (side‑view) foot X‑ray is essential for confirming the bony prominence characteristic of Haglund’s deformity. X‑ray does not show soft‑tissue inflammation well, so it is mainly used to assess bone shape and prominence.
- Ultrasound — Ultrasound is an excellent, accessible, and radiation‑free method for evaluating soft tissues. It can show inflammation of the retrocalcaneal and superficial bursae, thickening or degeneration of the Achilles tendon, and signs of active inflammation such as neovascularization.
- MRI — MRI provides the most detailed view of soft tissues, including the Achilles tendon, bursae, and surrounding fat pad. However, due to cost and availability, it is used less frequently when high‑quality ultrasound is available.

Conditions That Can Mimic Haglund’s Deformity
Pain at the back of the heel is not always caused by Haglund’s deformity. Several other conditions can present with similar symptoms, and a careful clinical exam is essential to distinguish them. Below are the most common disorders that may resemble a pump bump or posterior heel pain.
1. Insertional Achilles Tendinopathy
Although insertional Achilles tendinopathy is part of the Haglund’s syndrome triad, it far more often appears as an isolated condition. It is an overuse‑related disorder characterized by tendon degeneration, thickening, and sometimes small bone spurs at the tendon insertion.
Key difference: Haglund’s deformity always includes a bony prominence, while isolated insertional tendinopathy may occur without any bony enlargement.
2. Retrocalcaneal Bursitis
Retrocalcaneal bursitis can occur independently, especially in runners or after sudden increases in training volume. It is also common in inflammatory rheumatic diseases such as rheumatoid arthritis or ankylosing spondylitis.
Key difference: Pain is often deeper and more localized between the Achilles tendon and the heel bone, sometimes without a visible external bump.
3. Inflammatory Arthropathies
Conditions such as rheumatoid arthritis, ankylosing spondylitis, reactive arthritis, and psoriatic arthritis can cause bursitis and enthesitis (inflammation of tendon insertions). Key difference: Symptoms may be bilateral, associated with morning stiffness, and accompanied by other joint or systemic signs.
4. Plantar Fasciitis
Plantar fasciitis is caused by degenerative irritation of the plantar fascia at its insertion on the heel bone. Key difference: Pain is located on the bottom of the heel, not the back, and there is never a visible bump. A careful exam easily distinguishes it from Haglund’s deformity.
Treatment of Pump Bump Heel Pain
Treatment for Haglund’s deformity is primarily conservative. The goal is to reduce inflammation of the bursae and surrounding soft tissues. Conservative care can significantly reduce pain, but it cannot remove the bony prominence. Surgery is considered only when symptoms persist despite prolonged non‑operative management.
| Conservative (Non-Surgical) Treatment | |
| NSAID Medications | Non-steroidal anti-inflammatory drugs such as ibuprofen or diclofenac help reduce pain and inflammation around the Achilles tendon and bursae. |
| Topical Treatments | Anti-inflammatory gels, herbal creams, and cryotherapy gels may provide localized pain relief and a cooling effect. |
| Ice Therapy | Applying ice helps reduce swelling, pain, and inflammatory activity in irritated tissues around the heel. |
| Stretching Exercises | Stretching the calf muscles and Achilles tendon improves flexibility and decreases pressure on the heel. |
| Strengthening Exercises | Strengthening exercises improve Achilles tendon load tolerance and support long-term function. |
| Heel Pads and Orthotics | Heel lifts, soft heel pads, and orthotic insoles reduce friction and improve foot biomechanics during walking and standing. |
| Footwear Modification | Shoes with soft heel counters or mild heel elevation reduce irritation caused by pressure on the bony prominence. |
| Physical Therapy | Ultrasound, LASER therapy, electrotherapy, iontophoresis, and sonophoresis may reduce inflammation and promote tissue healing. |
| Short-Term Immobilization | Temporary immobilization with a walking boot or cast may allow irritated tissues to rest in severe cases. |
| Corticosteroid Injection | Injection into the inflamed bursa may significantly reduce pain and swelling when conservative care is insufficient. |
| Surgical Treatment | |
| Open Surgery | An open surgical approach removes the Haglund deformity through a direct incision and allows treatment of associated tendon pathology. |
| Endoscopic Surgery | A minimally invasive approach using small portals and a camera to remove the bony prominence with less soft-tissue disruption. |
Conservative (Non‑Surgical) Treatment
1. Medications
Non‑steroidal anti‑inflammatory drugs (NSAIDs) such as ibuprofen or diclofenac may help reduce pain and inflammation. They should be used at the lowest effective dose and for the shortest necessary duration due to potential side effects.
2. Topical Treatments
- Anti‑inflammatory gels/creams (NSAID‑based) applied directly to the painful area
- Herbal or essential‑oil creams (peppermint, eucalyptus, arnica) for cooling relief
- Cryotherapy gels for a cooling, numbing effect
3. Ice Therapy
Apply ice wrapped in a cloth for 10 minutes, then allow at least an hour before repeating. Cold reduces pain, swelling, and metabolic activity in inflamed tissues.
4. Rehabilitation and Exercises
- Stretching Exercises. Tightness of the Achilles tendon and calf muscles increases pressure on the heel. Stretching the gastrocnemius, soleus, and the Achilles tendon improves flexibility and reduces irritation.
- Strengthening Exercises. Strengthening the Achilles tendon and calf complex helps improve load tolerance and reduces symptoms over time.
5. Footwear and Orthotic Interventions
Raising the heel reduces pressure between the bony prominence and the Achilles tendon or bursa. This is especially helpful in patients with high arches.
Heel pads placed inside the shoe soften contact with the heel counter and reduce friction.
Orthotic insoles, whether custom or semi‑custom, improve foot biomechanics, reduce heel pressure, and increase comfort during walking and standing.
Footwear modification includes choosing shoes with no heel counter or a soft heel counter, wearing running shoes with mild heel elevation, and avoiding tight shoes or those with stiff backs such as dress shoes, work boots, or ski boots.
6. Physical Therapy
Physiotherapy plays an important role in managing Haglund’s deformity because it helps reduce inflammation, relieve pain, and improve tissue healing around the Achilles tendon and bursae. These modalities are typically used alongside footwear modification, stretching, and load management.
Modalities commonly used:
- Therapeutic ultrasound — decreases inflammation and improves local circulation.
- LASER therapy — helps reduce pain and promotes tissue repair.
- Electrotherapy — reduces pain and muscle tension around the heel.
- Sonophoresis and iontophoresis — enhance penetration of topical anti‑inflammatory medications into the inflamed tissues.
7. Short‑Term Immobilization
In more severe cases, temporary immobilization with a boot or cast may reduce irritation and allow tissues to calm down.
8. Corticosteroid Injection
A corticosteroid injection into the inflamed bursa can significantly reduce swelling and pain. Note: Injections must be performed with caution due to proximity to the Achilles tendon.
Surgical Treatment of Haglund’s Deformity
Surgical treatment is considered when symptoms persist despite at least six months of structured conservative therapy. There is no universal “gold standard,” and both open and endoscopic techniques are used in clinical practice. The choice depends on surgeon experience, severity of deformity, and associated tendon pathology.
Surgical Approaches
- Open surgical approach — involves a skin incision that provides direct access to the bony prominence. The surgeon removes the Haglund deformity under direct visualization.
- Endoscopic surgical approach — uses small portals and a camera to remove the bony prominence with minimal soft‑tissue disruption. This technique generally results in less postoperative pain and faster recovery.
What the Procedure Typically Includes
- Removal of the inflamed retrocalcaneal bursa
- Resection of the bony prominence (Haglund’s deformity)
- Debridement of degenerative Achilles tendon tissue when necessary
Both open and endoscopic techniques show similar effectiveness, but the risk of complications is reported to be almost twice as high with the open approach.
Frequently Asked Questions
What is the best footwear for Haglund’s deformity?
The best choice is footwear with a soft heel counter or no heel counter at all, such as sandals or running shoes. Running shoes are ideal because they offer good overall foot support, a cushioned heel, and slight heel elevation that reduces irritation. Avoid shoes with a stiff back, including ballet flats, dress shoes, and formal leather shoes.
Can I continue running if I have Haglund’s deformity?
Yes. The deformity itself does not prevent running. If pain appears, reduce activity, apply ice, and stretch the calf muscles and Achilles tendon. If pain interferes with running or daily activities, a medical evaluation is recommended.
Will the bony prominence go away over time?
No. Once formed, the bony prominence does not disappear on its own. However, symptoms can significantly improve or resolve with proper treatment.
Can Haglund’s deformity lead to Achilles tendon rupture?
It is uncommon, but long‑standing irritation and inflammation can weaken the tendon. Managing symptoms early helps reduce this risk.
How can I “get rid of” the bony prominence on my heel?
The only way to remove the bony prominence of Haglund’s deformity is surgery. Conservative treatment can reduce pain and inflammation but cannot eliminate the bone itself.
How can I prevent symptoms of Haglund’s deformity?
You can reduce the risk of symptoms by wearing proper footwear (avoid stiff heel counters and tight shoes), using arch‑supporting insoles if you have high arches, performing regular calf and Achilles stretching, and avoiding running on hard surfaces or uphill.
Vaishya R, Agarwal AK, Azizi AT, Vijay V. Haglund’s Syndrome: A Commonly Seen Mysterious Condition. Cureus. PubMed: Clinical review of Haglund’s syndrome and associated pathology
Radiopaedia. Haglund Deformity. Radiology reference: Imaging features of Haglund deformity
Radiopaedia. Retrocalcaneal Bursitis. Radiology guide: Retrocalcaneal bursitis imaging and diagnosis
Pringels L et al. Effectiveness of reducing tendon compression in the rehabilitation of insertional Achilles tendinopathy: a randomised clinical trial. British Journal of Sports Medicine. BJSM clinical trial: Tendon compression reduction in insertional Achilles tendinopathy rehabilitation
Kutzer K, Morrissette K, Wu K, et al. Descriptive Epidemiology of Haglund’s Syndrome: A Large Retrospective Cohort Study. Foot & Ankle Orthopaedics. Epidemiology study: Haglund’s syndrome prevalence and patient characteristics

















