

Anterior knee pain (AKP) is one of the most common reasons why active young individuals seek medical attention in sports injury clinics. Studies show that it affects up to 40% of adolescent athletes, making it one of the leading causes of reduced participation in sports and physical activity. When anterior knee pain persists, it can lead to varying levels of disability — limiting exercise, daily activities, and even work performance.
Although AKP is a single clinical term, it represents a heterogeneous group of conditions. Some problems are closely linked to adolescence and rapid growth, such as Osgood–Schlatter disease or Sinding–Larsen–Johansson syndrome. Others are primarily overuse‑related, including patellofemoral pain syndrome and patellar tendinopathy, which develop when the patellofemoral joint or patellar tendon is repeatedly exposed to high loads without adequate recovery. A third group is associated with occupational stress, such as prolonged kneeling, which can irritate the prepatellar bursa and lead to prepatellar bursitis.
Despite different mechanisms, these conditions share a common feature: pain in the anterior aspect of the knee, typically aggravated by activities that increase patellofemoral load — squatting, stair climbing, running, or jumping.
Typical Symptoms of Anterior Knee Pain
Patients with anterior knee pain most commonly report pain in the front of the knee, often described as kneecap pain, pain below the kneecap, or pain around the kneecap. Swelling and instability may occur, but they are less frequent and usually depend on the underlying condition. Each symptom provides important diagnostic clues, and a detailed history is essential for identifying the underlying pathology.
Pain Characteristics and Onset
The onset of anterior knee pain is usually insidious, with symptoms progressing gradually. Many patients describe a waxing and waning pattern rather than a sudden onset. A history of trauma is uncommon, except in cases of post‑traumatic patellar instability, where the mechanism of injury is diagnostically important.
Although anterior knee pain is often described as a dull, aching kneecap pain, patients may also experience sharp pain during deep squatting or when bending the knee. These sharper episodes typically occur when the knee is loaded in high flexion, such as during deep squats, lunges, stair descent, or rising from a seated position.
Pain Location as a Diagnostic Clue
The location of pain is one of the most valuable elements of the clinical history. Patients often describe their symptoms as kneecap pain, pain below the kneecap, or pain around the kneecap, and this localization strongly guides the differential diagnosis.
Pain Patterns and Likely Diagnoses
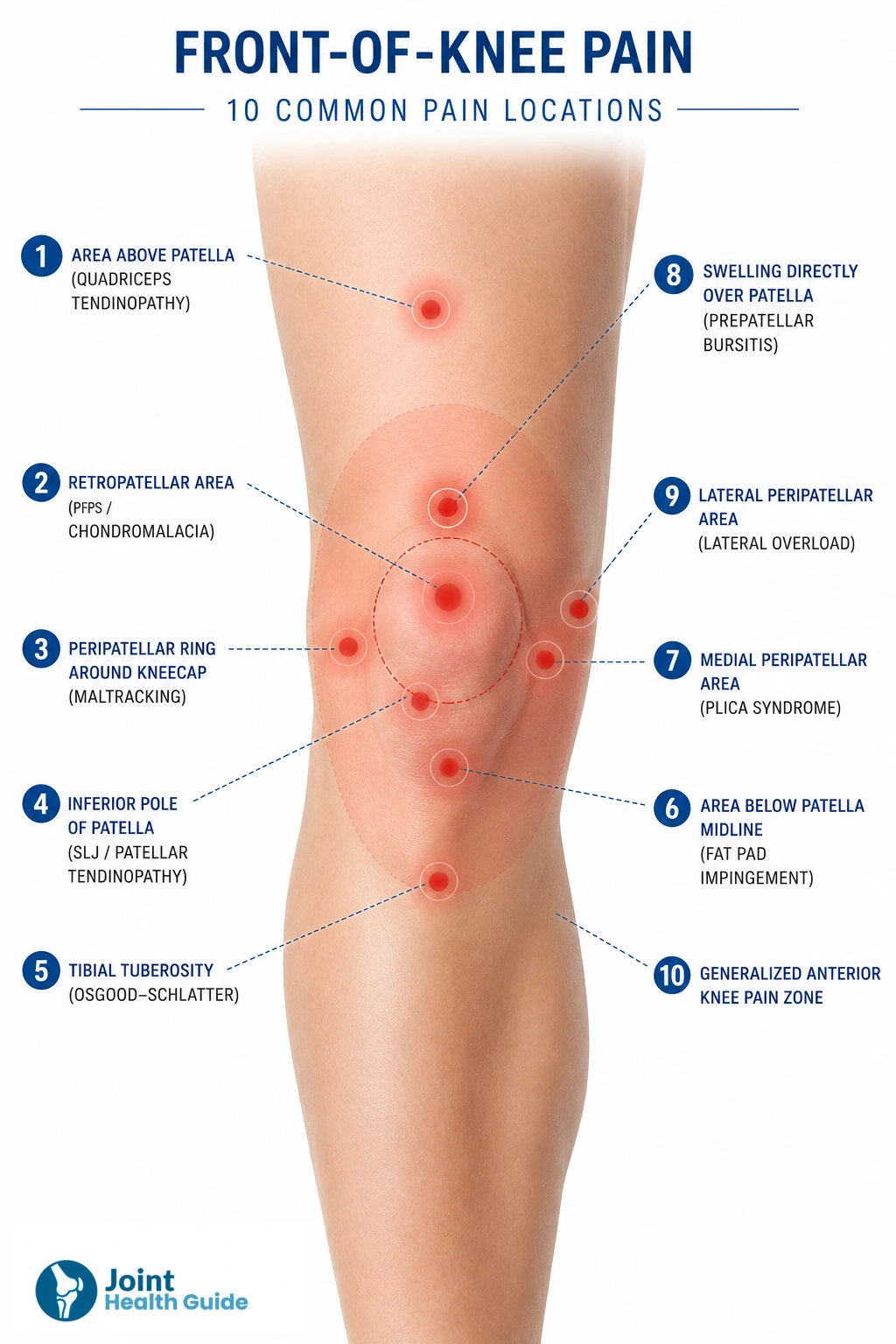
- Pain at the tibial tuberosity — suggests Osgood–Schlatter disease
- Pain at the inferior pole of the patella — suggests Sinding–Larsen–Johansson syndrome in children and adolescents or patellar tendinopathy (“jumper’s knee”) in athletes
- Retropatellar kneecap pain — typical for patellofemoral pain syndrome or chondromalacia patellae
- Peripatellar pain around the kneecap — common in patellofemoral overload and maltracking
- Pain below the kneecap — characteristic of patellar tendinopathy (“jumper’s knee”)
- Localized swelling directly over the kneecap — suggests prepatellar bursitis, often related to occupational kneeling
Activity‑Related Symptom Aggravation
Anterior knee pain typically worsens with activities that increase patellofemoral joint stress:
- Stair climbing or descending
- Squatting
- Kneeling
- Running or jumping
- Prolonged sitting — the classic movie theater sign
Pain often improves with knee extension, which points toward pathology of the extensor mechanism rather than the femorotibial joint.
Associated Symptoms of Anterior Knee Pain
- Swelling — Swelling is not a dominant feature of anterior knee pain, but it may appear after trauma (suggesting patellar instability), after periods of overuse (typically resolving with rest), or recur intermittently in cases of chronic overload or synovial irritation.
- Instability or “Giving Way” — Some patients report a sensation of the knee “giving way,” most often due to reflex quadriceps inhibition or quadriceps atrophy in chronic cases. This is usually not true mechanical instability but a neuromuscular response to pain around the kneecap.
- Painfull Giving Way — A painfull giving‑way episode may indicate transient patellar maltracking or subluxation, irritation of a synovial plica, an unstable cartilage flap, or—less commonly—meniscal or ACL pathology, especially when the giving way occurs during rotational movements.
- Crepitus — Many patients report crepitus or “crackling” sensations around the kneecap, but this finding is usually not clinically significant and rarely correlates with structural damage.
- Motion Limitations — Some individuals experience limited knee extension, particularly when synovial irritation, mechanical obstruction, or pain below the kneecap restricts full movement.
Causes of Anterior Knee Pain
Anterior knee pain can arise from several different structures around the patella, which is why patients may describe their symptoms as kneecap pain, pain below the kneecap, or pain around the kneecap. These conditions range from growth‑related problems in adolescents to overuse injuries and occupational disorders, each producing a characteristic pattern of anterior knee pain.
1. Patellofemoral Pain Syndrome
What it is: Patellofemoral pain syndrome is an overuse‑related condition caused by irritation of the patellofemoral joint. It is the most common cause of anterior knee pain in adolescents and young adults.
Who gets it: Active individuals, runners, cyclists, and patients with altered lower‑limb biomechanics or hip muscle weakness.
Typical symptoms: Diffuse retropatellar kneecap pain or pain around the kneecap, especially during stair climbing, squatting, running, or prolonged sitting (movie theater sign).
Why it causes anterior knee pain: Increased compressive forces between the patella and femur during knee flexion irritate the joint surfaces and surrounding soft tissues.
2. Chondromalacia Patellae
What it is: Softening or degeneration of the cartilage on the posterior surface of the patella.
Who gets it: Young adults, athletes, and individuals with patellar maltracking or previous trauma.
Typical symptoms: Diffuse anterior knee pain, crepitus around the kneecap, and sharp pain during deep knee flexion.
Why it causes anterior knee pain: Damaged cartilage increases retropatellar pressure and irritates subchondral bone during movement.
Important Note: PFPS vs. Chondromalacia Patellae
Although patellofemoral pain syndrome and chondromalacia patellae often produce very similar symptoms, they are not the same condition.
- PFPS can occur without any cartilage damage — it is a functional overload syndrome.
- Chondromalacia involves structural cartilage changes, but symptoms may be indistinguishable from PFPS.
In practice, many patients with anterior knee pain have PFPS‑type symptoms even when imaging shows no cartilage injury.
If your anterior knee pain feels like deep kneecap pain or discomfort during squatting and stair use, you may be dealing with early cartilage irritation. For a detailed guide on symptoms, causes, and treatment options, read our full article on chondromalacia patella.
3. Patellar Tendinopathy (“Jumper’s Knee”)
What it is: A degenerative overload injury of the patellar tendon, typically at its origin on the inferior pole of the patella.
Who gets it: Jumping athletes (basketball, volleyball), sprinters, and individuals with sudden increases in training load.
Typical symptoms: Localized pain below the kneecap, tenderness at the inferior pole, and sharp pain during jumping, sprinting, or deep squatting.
Why it causes anterior knee pain: High tensile forces on the patellar tendon overload the tendon fibers and produce localized anterior knee pain.
4. Quadriceps Tendinopathy
What it is: Overuse injury of the quadriceps tendon at the superior pole of the patella.
Who gets it: Athletes performing repeated acceleration, deceleration, or heavy resistance training.
Typical symptoms: Pain above the kneecap, discomfort during resisted knee extension, and tenderness at the quadriceps tendon insertion.
Why it causes anterior knee pain: Excessive traction forces at the superior patellar pole irritate the tendon and surrounding tissues.
5. Osgood–Schlatter Disease
What it is: Traction apophysitis of the tibial tuberosity during growth.
Who gets it: Adolescents during rapid growth spurts, especially those active in running and jumping sports.
Typical symptoms: Pain at the tibial tuberosity, swelling, and pain during running, jumping, or kneeling.
Why it causes anterior knee pain: Repetitive traction from the patellar tendon stresses the immature growth plate.
6. Sinding–Larsen–Johansson Syndrome
What it is: Traction injury at the inferior pole of the patella.
Who gets it: Children and adolescents, particularly jumping athletes.
Typical symptoms: Pain at the inferior pole of the patella or pain below the kneecap during activity.
Why it causes anterior knee pain: Stress on the immature patellar pole during growth leads to localized inflammation and pain.
7. Prepatellar Bursitis
What it is: Inflammation of the prepatellar bursa located directly over the kneecap.
Who gets it: Workers who kneel frequently (floor layers, plumbers, gardeners).
Typical symptoms: Localized swelling over the kneecap, warmth, and tenderness.
Why it causes anterior knee pain: Inflamed bursa produces direct anterior swelling and pressure‑related pain.
8. Patellar Instability
What it is: Abnormal patellar tracking, subluxation, or dislocation.
Who gets it: Adolescents, individuals with trochlear dysplasia, ligamentous laxity, or previous dislocations.
Typical symptoms: Instability, giving‑way, swelling after episodes, and kneecap pain.
Why it causes anterior knee pain: Abnormal patellar motion increases stress on the patellofemoral joint and surrounding tissues.
9. Synovial Plica Syndrome
What it is: Irritation of the medial synovial plica.
Who gets it: Young active individuals, runners, and patients with repetitive knee flexion.
Typical symptoms: Medial peripatellar pain, snapping, and painful giving‑way.
Why it causes anterior knee pain: An inflamed plica rubs against the medial patellar facet, producing localized irritation.
10. Hoffa’s Fat Pad Impingement
What it is: Inflammation or impingement of the infrapatellar fat pad.
Who gets it: Patients with hyperextension injuries or repetitive overload.
Typical symptoms: Pain below the kneecap, pain with full extension, and tenderness around the patellar tendon.
Why it causes anterior knee pain: The fat pad becomes trapped between the patella and femur, causing sharp anterior pain.
Clinical Examination
A clinical examination helps determine which structure around the kneecap is causing pain. The assessment is simple, hands‑on, and focuses on alignment, movement, and specific tender points. Each finding helps narrow down the most likely diagnosis behind kneecap pain, pain around the kneecap, or pain below the kneecap.
1. Posture and Alignment
The examination begins with observing how the legs align when standing and walking. Even small alignment differences can change how the kneecap moves.
- Knees that angle inward (genu valgum) can increase pressure on the outer side of the patella and are often seen in patellofemoral pain syndrome (PFPS) and patellar instability.
- Rotation of the hip or lower leg can alter the path of the patella, contributing to maltracking.
- A higher Q‑angle (the angle of quadriceps pull) may increase the tendency of the patella to shift outward.
Why this matters: If the leg alignment is off, the patella is exposed to higher stress, making anterior knee pain more likely.
2. Palpation (Identifying the Painful Spot)
The clinician gently presses around the kneecap to identify the exact source of pain. This is one of the most useful parts of the exam.
- Pain below the kneecap → often patellar tendinopathy or Sinding–Larsen–Johansson syndrome in adolescents.
- Pain above the kneecap → may indicate quadriceps tendinopathy.
- Pain on the inner side of the kneecap → common in plica syndrome.
- Pain on the outer side → may suggest lateral retinaculum irritation or Hoffa’s fat pad impingement.
- Pain at the tibial bump (tibial tuberosity) → typical for Osgood–Schlatter disease.
- Soft swelling directly over the kneecap → usually prepatellar bursitis.
Why this matters: The exact location of pain is one of the strongest diagnostic clues.
3. Patellar Tracking (How the Kneecap Moves)
The clinician observes how the patella glides as the knee bends and straightens.
- Patella drifting outward → suggests patellar instability or weak hip muscles.
- A sudden “jump” of the patella during bending (J‑sign) → typical for maltracking or trochlear dysplasia.
- Difficulty lifting the outer edge of the patella → indicates tight lateral structures, often seen in PFPS.
Why this matters: Abnormal patellar motion is one of the most common causes of anterior knee pain.
4. Provocation Tests (Simple Movement Checks)
These tests gently load the kneecap or surrounding tissues to see which structure reproduces the pain.
- Pain when the kneecap is compressed during quadriceps contraction → suggests PFPS or chondromalacia patellae.
- Feeling that the kneecap might “slip out” → indicates patellar instability.
- Pain when pressing the fat pad during knee extension → typical for Hoffa’s fat pad impingement.
- Limited kneecap mobility → may indicate tight lateral tissues or post‑injury scarring.
Why this matters: These tests help distinguish between joint surface pain, instability, and soft‑tissue impingement.
5. Range of Motion
The clinician checks how far the knee can bend and straighten.
- Pain in deep knee flexion → common in PFPS, chondromalacia, and patellar tendinopathy.
- Pain at full extension → often linked to Hoffa’s fat pad impingement.
- Difficulty fully straightening the knee → may suggest plica syndrome or post‑surgical stiffness.
6. Strength and Functional Control
Weakness in the muscles around the hip and knee can significantly affect patellar mechanics.
- Weak gluteal muscles → often lead to inward knee collapse during squatting, strongly associated with PFPS.
- Weak quadriceps → common in patellofemoral pain and may cause a “giving‑way” sensation.
- Single‑leg squat or step‑down test → reveals poor control of the thigh bone, a key factor in PFPS.
- Core weakness → can contribute to poor lower‑limb alignment during movement.
7. Hip and Pelvis Assessment
Because the knee is part of a larger kinetic chain, the hips are always examined.
- Excessive inward rotation of the hip can push the patella outward during movement.
- Weak hip abductors and external rotators are strongly linked to PFPS.
- Hip joint issues can occasionally refer pain to the front of the knee.
Key Clinical Clues by Diagnosis
| Condition | Typical Features |
|---|---|
| Patellofemoral Pain Syndrome (PFPS) | Pain around or behind the kneecap, pain during squatting, stair climbing, prolonged sitting, often associated with hip muscle weakness. |
| Chondromalacia Patellae | Grinding or crepitus behind the patella, pain during deep knee bending or prolonged loading. |
| Patellar Tendinopathy | Pain below the kneecap at the patellar tendon, worsens with jumping, running, and explosive activities. |
| Hoffa’s Fat Pad Impingement | Pain during full knee extension, tenderness below the patella on either side of the tendon. |
| Plica Syndrome | Pain along the inner side of the knee, snapping or catching sensation during movement. |
| Patellar Instability | Feeling that the kneecap slips or moves out of place, positive patellar apprehension test. |
| Osgood–Schlatter Disease | Pain and tenderness over the tibial tuberosity (shinbone bump), common in growing adolescents. |
| Sinding–Larsen–Johansson (SLJ) Syndrome | Pain at the lower pole of the patella, typically affects physically active adolescents. |
| Prepatellar Bursitis | Visible swelling directly over the kneecap, tenderness and discomfort when kneeling. |
- PFPS → pain around the kneecap, pain in squatting, weak hip muscles
- Chondromalacia patellae → crepitus, pain in deep bending
- Patellar tendinopathy → pain below the kneecap, pain during jumping
- Hoffa’s fat pad impingement → pain in full extension, tenderness under the patella
- Plica syndrome → inner‑knee pain, snapping sensation
- Patellar instability → feeling of the kneecap slipping, positive apprehension
- Osgood–Schlatter → pain at the tibial bump
- SLJ syndrome → pain at the lower pole of the patella in adolescents
- Prepatellar bursitis → swelling directly over the kneecap
Imaging Studies for Anterior Knee Pain
In most cases, anterior knee pain is diagnosed based on the patient’s symptoms and physical examination. Imaging tests are usually used to confirm the suspected diagnosis, assess the severity of structural changes, or rule out other causes of knee pain.
X-rays
X-rays are typically the first imaging study performed when anterior knee pain persists or follows an injury. While they do not show cartilage, tendons, ligaments, or other soft tissues, they can reveal fractures, osteoarthritis, patellar malalignment, patella alta, and abnormalities of the trochlear groove that may contribute to patellar instability or maltracking.
A normal X-ray does not rule out many common causes of anterior knee pain.
Ultrasound
Diagnostic ultrasound is a useful and inexpensive tool for evaluating superficial soft tissues around the kneecap. It can identify:
- Patellar tendinopathy (jumper’s knee)
- Quadriceps tendinopathy
- Prepatellar bursitis
- Infrapatellar bursitis
- Hoffa’s fat pad inflammation
- Joint effusions (fluid in the knee)
Ultrasound also allows dynamic assessment during movement and can compare the painful knee with the opposite side in real time.
MRI
MRI is the most comprehensive imaging modality for anterior knee pain because it provides excellent visualization of cartilage, tendons, ligaments, bone marrow, and other soft tissues.
MRI can help diagnose:
- Patellofemoral cartilage damage (chondromalacia patellae)
- Patellofemoral pain syndrome associated with maltracking
- Patellar tendinopathy
- Hoffa’s fat pad impingement
- Plica syndrome
- Patellar instability and MPFL injuries
- Osgood-Schlatter disease
- Sinding-Larsen-Johansson syndrome
- Meniscal tears and other intra-articular pathology
MRI can also evaluate anatomical factors that predispose to patellar maltracking, such as trochlear dysplasia, patella alta, and abnormal patellar alignment.
CT Scan
CT scans are used less frequently but can provide detailed information about bone anatomy and patellar alignment. They are particularly useful when evaluating trochlear dysplasia, rotational abnormalities of the lower limb, or patellar maltracking. CT may also be used for surgical planning in complex cases of patellar instability.
Which Imaging Test Is Best?
There is no single best imaging test for every patient. X-rays are usually the starting point, ultrasound is valuable for tendon and bursa disorders, and MRI provides the most complete assessment of the structures commonly responsible for anterior knee pain. Imaging findings should always be interpreted together with the patient’s symptoms and physical examination findings.
| Condition | Best Imaging Method |
|---|---|
| Patellofemoral Pain Syndrome (PFPS) | Usually diagnosed clinically; MRI may be considered if symptoms persist or the diagnosis is uncertain. |
| Chondromalacia Patellae | MRI |
| Patellar Tendinopathy | Ultrasound or MRI |
| Quadriceps Tendinopathy | Ultrasound or MRI |
| Patellar Instability | X-ray, MRI, or CT (for alignment assessment) |
| Hoffa’s Fat Pad Impingement | MRI or Ultrasound |
| Plica Syndrome | MRI or Ultrasound |
| Osgood–Schlatter Disease | X-ray and Ultrasound |
| Sinding–Larsen–Johansson (SLJ) Syndrome | Ultrasound or MRI |
| Prepatellar Bursitis | Ultrasound |
General Treatment Principles for Anterior Knee Pain
Although each condition causing anterior knee pain has its own specific treatment, most patients benefit from a few general principles that reduce irritation, improve movement quality, and support long‑term recovery.
- 1. Reduce the activities that overload the kneecap Deep squats, lunges, jumping, hill running, and prolonged sitting with bent knees often increase pain. Temporarily reducing these movements helps calm irritated tissues.
- 2. Keep moving — but choose low‑impact options Complete rest is rarely helpful. Activities like cycling, swimming, or walking on flat ground maintain fitness without stressing the patellofemoral joint.
- 3. Strengthen the hip and thigh muscles Weak gluteal and quadriceps muscles are common contributors to anterior knee pain. Strengthening them improves patellar tracking and reduces overload, regardless of the exact diagnosis.
- 4. Improve flexibility where needed Tight quadriceps, hamstrings, calves, or hip flexors can increase pressure on the kneecap. Gentle stretching helps restore normal mechanics.
- 5. Progress training gradually Sudden increases in running distance, jumping volume, or gym intensity often trigger symptoms. A slow, steady progression (10–15% per week) reduces flare‑ups.
- 6. Use symptom‑relief strategies when needed Ice after activity, heat before exercise, and short‑term use of NSAIDs (if appropriate) can help manage pain during recovery.
- 7. Consider taping or bracing for short‑term relief Kinesio taping, patellar straps, or soft braces may reduce pain in PFPS, tendinopathy, or mild instability — but they are supportive tools, not long‑term solutions.
- 8. Address foot mechanics if relevant Supportive footwear or simple orthotics can help patients with overpronation or patellofemoral overload.
- 9. Seek physiotherapy when symptoms persist A tailored exercise program is often the most effective long‑term treatment for AKP, especially in PFPS, tendinopathy, and maltracking.
- 10. Surgery is rarely needed It is reserved for structural problems such as recurrent patellar instability, significant cartilage defects, or symptomatic plica that does not respond to conservative care.
Prognosis & What to Expect
Most people with anterior knee pain recover well with the right combination of activity adjustments, gradual strengthening, and time. The prognosis depends on the underlying condition, but the overall outlook is very good for the majority of patients.
1. Recovery is usually gradual, not instant Anterior knee pain rarely disappears overnight. Most patients notice steady improvement over weeks to months, especially once they start strengthening the hip and thigh muscles and reduce activities that overload the kneecap.
2. Flare‑ups are normal Even when things are improving, occasional flare‑ups can happen — after long walks, deep squats, hill running, or long periods of sitting. These episodes don’t mean something is “damaged”; they simply reflect temporary irritation.
3. Most conditions improve without surgery PFPS, chondromalacia, tendinopathy, plica syndrome, and fat pad irritation almost always respond to conservative treatment. Surgery is reserved for a small number of patients with structural problems like recurrent patellar instability or significant cartilage defects.
4. Adolescents almost always recover fully Growth‑related conditions such as Osgood–Schlatter and SLJ syndrome typically settle as the growth plates mature. Symptoms may come and go for months, but long‑term outcomes are excellent.
5. Strength matters more than rest Rest alone rarely solves anterior knee pain. Patients who commit to hip and quadriceps strengthening tend to recover faster and have fewer recurrences.
6. Imaging findings do not always predict symptoms It’s common for MRI to show “changes” that sound worrying — mild cartilage wear, fat pad edema, or tendon thickening — even in people without pain. What matters most is how the knee behaves, not what the scan shows.
7. When to seek further help A follow‑up with a clinician or physiotherapist is recommended if:
- pain persists longer than 6–8 weeks despite basic treatment
- the knee repeatedly “gives way”
- swelling appears after minor activity
- pain becomes sharp, locking occurs, or weight‑bearing becomes difficult
8. Long‑term outlook With proper management, most patients return to full activity — including running, jumping, and sports — without limitations. The key is learning how to load the knee gradually and maintain good hip and thigh strength.
D’Ambrosi R, Meena A, Raj A, Ursino N, Hewett TE. Anterior Knee Pain: State of the Art. Sports Medicine – Open. Comprehensive review: Modern concepts in anterior knee pain diagnosis and treatment
Bump JM, Lewis L. Patellofemoral Syndrome. StatPearls Publishing. StatPearls review: Patellofemoral pain syndrome diagnosis and management
Mabrouk A, Lee CYM, Sherman AL. Patellar Tendinopathy (Jumper’s Knee). StatPearls Publishing. StatPearls review: Patellar tendinopathy causes, diagnosis, and treatment
Casadei K, Hermena S. Plica Syndrome. StatPearls Publishing. StatPearls review: Plica syndrome diagnosis and management
Nacey NC, Geeslin MG, Miller GW, Pierce JL. Magnetic Resonance Imaging of the Knee: An Overview and Update of Conventional and State-of-the-Art Imaging. Journal of Magnetic Resonance Imaging. MRI review: Modern imaging techniques for knee disorders
Koplas M, Schils J, Sundaram M. The Painful Knee: Choosing the Right Imaging Test. Cleveland Clinic Journal of Medicine. Imaging guide: Selecting appropriate imaging studies for knee disorders
Bunt CW, Jonas CE, Chang JG. Knee Pain in Adults and Adolescents: The Initial Evaluation. American Family Physician. Clinical guide: Initial assessment and differential diagnosis of knee pain

















