

Knee pain is one of the most common musculoskeletal symptoms, affecting people of all ages — from active adolescents to older adults. The knee is a large, complex joint, and because many structures work together, knee pain can develop from multiple sources — injuries, overuse, biomechanical stress, inflammation, or degenerative changes like osteoarthritis.
In younger individuals and physically active people, knee pain most often results from overuse syndromes, sports injuries, or biomechanical overload. In contrast, among adults over the age of 50, knee osteoarthritis becomes the leading cause of persistent knee pain.
In this article, I will systematically present the 14 most common causes of knee pain, grouped by age, mechanism of injury, and the typical location of pain. You will learn how knee pain develops, how each condition is diagnosed, and which modern, evidence‑based treatment options are available. Because knee pain has many potential causes, the article is extensive — feel free to use the table of contents to navigate directly to the sections most relevant to you.
Anatomy of the Knee
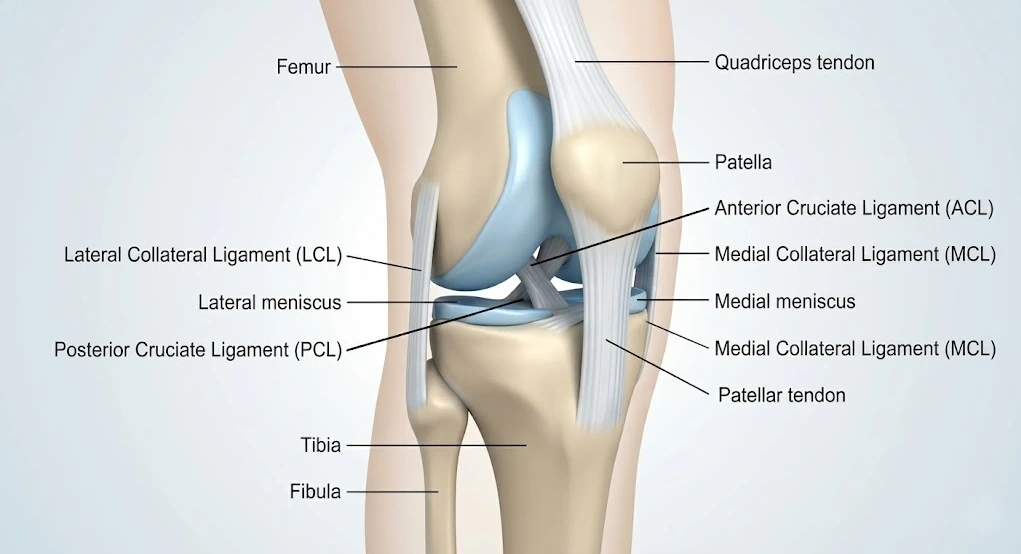
The knee is a complex joint that connects the femur (thigh bone) with the two bones of the lower leg — the tibia and the fibula. On the front of the joint sits the patella (kneecap), which glides within a groove on the femur called the trochlea. Together, they form the patellofemoral joint.
The ends of all joint‑forming bones are covered with smooth articular cartilage, which reduces friction and allows fluid, pain‑free movement. Knee motion is powered by the surrounding muscles, while ligaments and tendons provide stability.
Two major muscle groups control knee movement:
- the quadriceps, located at the front of the thigh, which straighten the knee
- the hamstrings, located at the back of the thigh, which bend the knee
Tendons connect these muscles to bone, while ligaments connect bone to bone and are essential for joint stability.
The knee also contains two important shock‑absorbing structures — the menisci. These C‑shaped fibrocartilage pads sit between the femur and tibia. Their main roles are to:
- distribute load
- absorb impact
- improve joint stability
- protect the articular cartilage from excessive wear
Healthy menisci are crucial for long‑term knee function and play a major role in preventing degenerative changes.
Symptoms of Knee Pain
Knee pain symptoms vary depending on the underlying cause. Pain may appear at the front, back, inner, or outer side of the knee — or be diffuse and difficult to localize. The location and character of pain often provide important diagnostic clues.
Common Knee Pain Characteristics
- Knee pain can be sharp, dull, or stabbing depending on the cause.
- Pain may start suddenly (injury) or gradually (overuse, arthritis).
- Symptoms often worsen with walking, standing, bending, or prolonged sitting.
- Pain may radiate up the thigh or down the shin.
- Many patients can point to a specific painful spot, which helps narrow the diagnosis.
- Discomfort may be constant or triggered only by certain movements.
- Night pain is common in inflammatory conditions such as arthritis.
- Reduced range of motion often appears in knee osteoarthritis.
- Patients may change their gait to reduce pain, resulting in antalgic limping or limping due to joint stiffness.
Associated Signs and Clinical Findings
- Swelling — fluid buildup (knee effusion) from injury (sprain, meniscus tear, ACL tear) or inflammation (arthritis).
- Stiffness and limited mobility — common in osteoarthritis and rheumatoid arthritis; morning stiffness is typical. Meniscus tears may cause locking, preventing full extension.
- Clicking, popping, or grinding sounds — may occur with cartilage injuries, meniscus tears, ligament instability, or osteoarthritis. Not all sounds indicate disease; some are harmless.
- Knee instability — the feeling that the knee “gives way,” often linked to ACL or MCL injury.
- Warmth and redness — suggest inflammation, infection, gout, or acute arthritis.
- Tenderness to touch — may indicate tendinitis, bursitis, or meniscus injury.
- Visible deformity — such as knock‑knees (valgus) or bow‑legs (varus), often due to osteoarthritis, rheumatoid arthritis, or chronic joint damage.
Causes of Knee Pain
Knee pain is one of the most common musculoskeletal symptoms and can arise from a wide range of conditions — from acute injuries and overuse syndromes to chronic degenerative changes and systemic inflammatory diseases. It can significantly reduce function, limit daily activities, and affect overall quality of life.
To make this complex topic easier to understand, the causes of knee pain can be grouped in several clinically useful ways: by pain location, by mechanism of injury, and by patient age. Each of these perspectives provides valuable diagnostic clues.
Pain Location as a Diagnostic Clue
The location of knee pain often helps narrow down the underlying cause:
- Anterior knee pain (front of the knee) — common in patellofemoral pain syndrome or patellar tendinopathy (“jumper’s knee”).
- Medial knee pain (inner side) — frequently associated with MCL injuries, medial meniscus tears, or knee osteoarthritis.
- Lateral knee pain (outer side) — often caused by iliotibial band syndrome or lateral meniscus injuries.
- Posterior knee pain (back of the knee) — may indicate a Baker’s cyst or a tear of the posterior horn of the medial meniscus.
Understanding where the pain is felt is often the first step toward identifying the correct diagnosis.
Causes Based on Mechanism
Knee pain can also be classified according to the underlying process:
- Acute injuries — such as ligament tears, meniscus tears, fractures, or dislocations, typically caused by sudden trauma.
- Chronic overuse syndromes — common in athletes and active individuals; examples include jumper’s knee and patellofemoral pain syndrome.
- Degenerative conditions — such as knee osteoarthritis, which become more common with age and are not usually linked to a specific injury.
- Inflammatory and systemic diseases — including rheumatoid arthritis and gout, which can cause pain, swelling, and stiffness.
Age‑Related Patterns
Age can also influence the likely cause of knee pain:
- Younger individuals more often experience injuries and overuse syndromes.
- Older adults more commonly develop degenerative conditions such as osteoarthritis.
Recognizing these age‑related trends helps guide clinical reasoning and patient expectations.
How This Article Is Organized
In the following sections, the 14 most common causes of knee pain are presented according to mechanism of injury and pain location. This structure helps readers quickly identify which conditions may be responsible for their symptoms and understand how each condition develops, how it is diagnosed, and which treatment options are supported by current evidence.
Acute Knee Injuries
Acute knee injuries are a common cause of sudden pain and loss of function. They typically occur during sports, accidents, or falls, when a sudden impact, twist, or overload damages one or more structures within the knee. These injuries often require prompt assessment to prevent long‑term joint damage and to guide appropriate treatment.
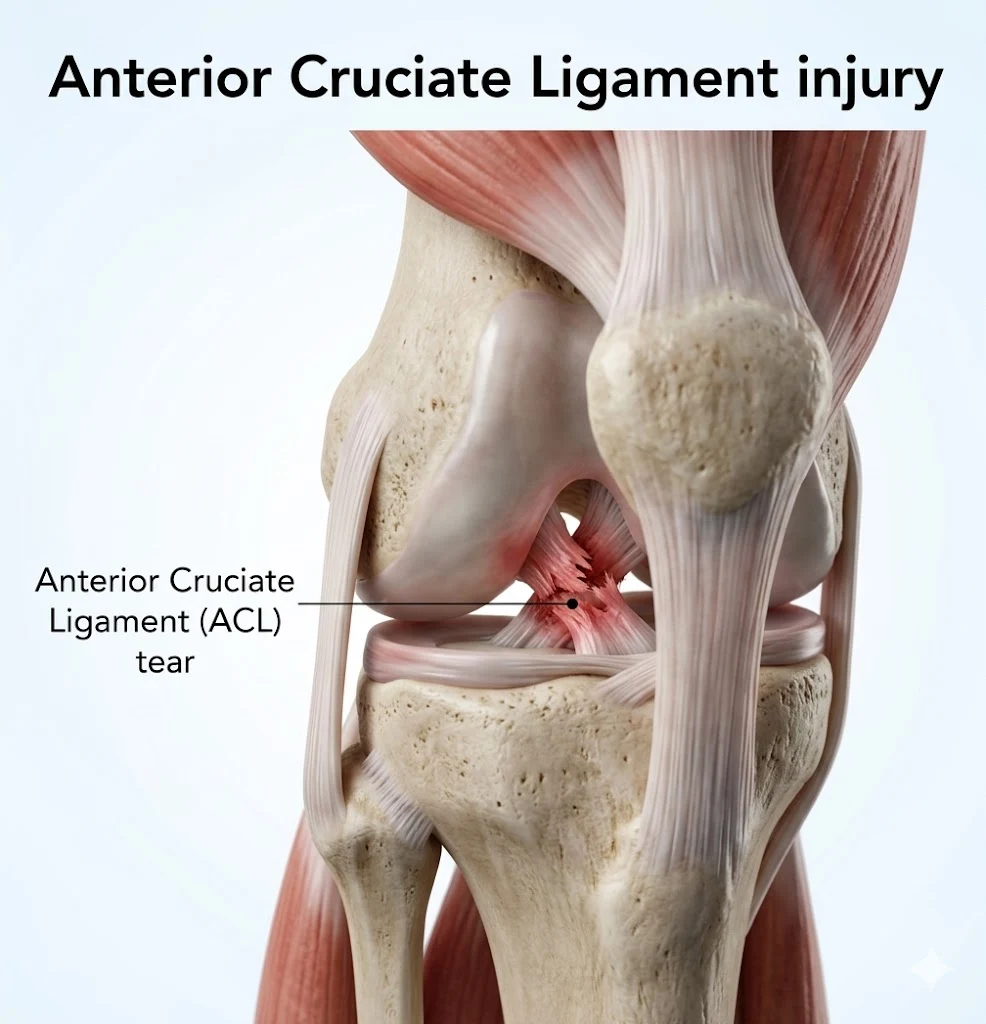
1. ACL Injury (Anterior Cruciate Ligament)
The anterior cruciate ligament (ACL) is one of the two cruciate ligaments that stabilize the knee by preventing excessive forward movement of the tibia relative to the femur. It is the most commonly injured knee ligament, especially among athletes such as football players, skiers, handball players, and basketball players.
Typical age group: younger and middle‑aged active individuals
Typical pain location: diffuse pain throughout the knee
Mechanism of Injury
Most ACL tears occur without direct contact, during sudden changes of direction, pivoting, rapid deceleration, or awkward landings. A direct blow to the outer side of the knee can also cause injury, particularly in football.
Symptoms
Patients often report a sudden “pop”, followed by immediate pain and inability to continue activity. Swelling usually develops within the first two hours. Later, patients may experience knee instability, difficulty walking, and reduced range of motion.
Diagnosis
Clinical tests such as the Lachman test and anterior drawer test help assess ligament integrity. MRI is used to confirm the diagnosis and evaluate associated injuries.
Treatment
Management may be non‑operative (physical therapy) in patients with mild instability or lower activity demands. Surgical reconstruction is recommended for complete tears in active individuals, especially athletes, or when instability persists despite rehabilitation.
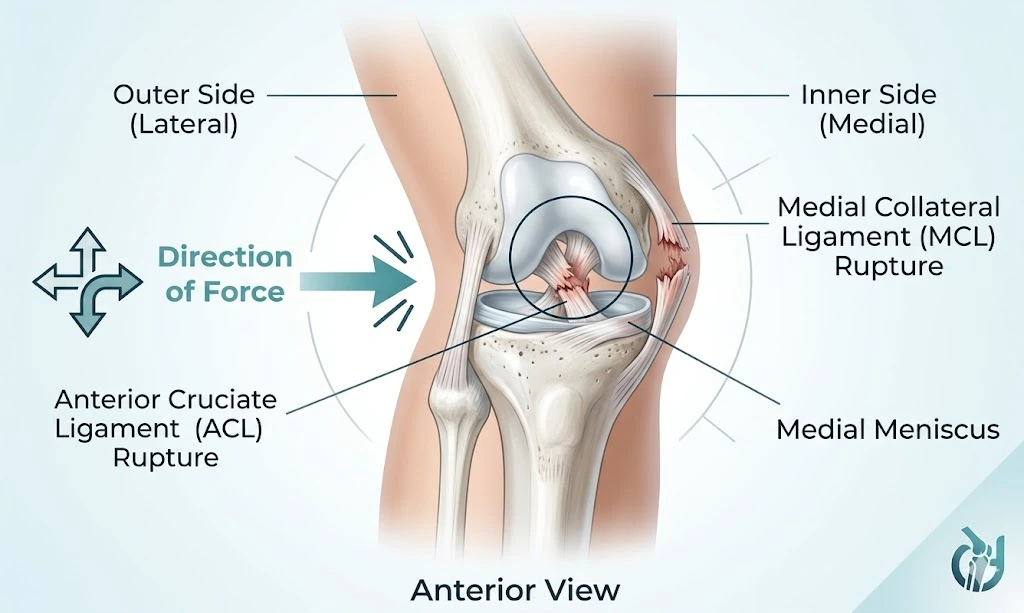
2. Medial Collateral Ligament (MCL) Injury
The medial collateral ligament (MCL) is a flat band of connective tissue located on the inner side of the knee, connecting the femur to the tibia. Its main role is to provide medial stability and prevent the lower leg from bending outward (valgus stress). MCL injuries are the second most common ligament injuries in the knee, frequently occurring in sports such as skiing, football, and handball.
Typical age group: younger and middle‑aged active individuals
Typical pain location: inner (medial) side of the knee
Mechanism of Injury
MCL injuries usually occur during sudden twisting, cutting, or changes of direction. A direct blow to the outer side of the knee can also cause excessive valgus stress and tear the ligament — a common scenario in contact sports. MCL injuries may be isolated but often occur together with other injuries, such as the “unhappy triad” (MCL + ACL + medial meniscus).
Symptoms
Patients typically report sharp medial knee pain, especially after a specific injury event. Swelling and tenderness along the inner knee are common. Some patients feel a “pop” at the moment of injury, followed by difficulty walking and a sense of instability. Complete tears often cause more pronounced swelling on the medial side.
Diagnosis
Diagnosis is based on clinical examination and imaging. The valgus stress test is the key clinical test for assessing MCL integrity. Injuries are classified into Grade I–III depending on joint opening. MRI is the most accurate method for evaluating the ligament and detecting associated injuries. Ultrasound is a useful, accessible alternative that can visualize the ligament and assess valgus stress in real time.
Treatment
Most MCL injuries — especially Grade I and II — are treated conservatively with short‑term immobilization, pain control, and structured physical therapy to restore strength and stability. Grade III injuries may require surgical reconstruction.
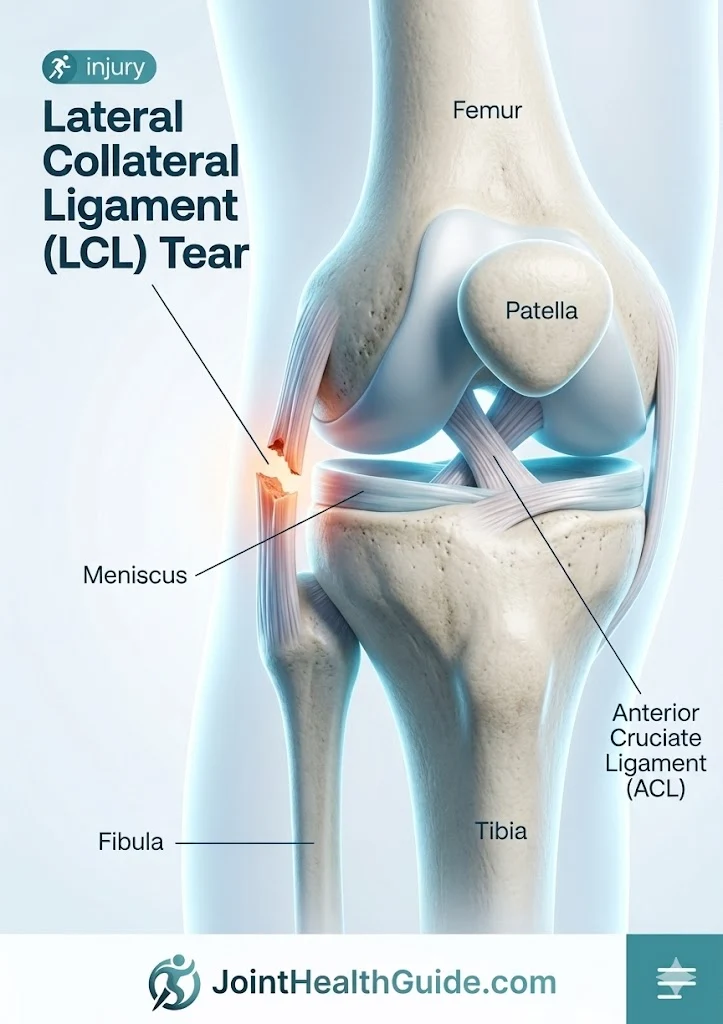
3. Lateral Collateral Ligament (LCL) Injury
The lateral collateral ligament (LCL) is a rope‑like structure located on the outer side of the knee, connecting the femur to the head of the fibula. It provides lateral stability and prevents the lower leg from collapsing inward (varus stress). LCL injuries are much less common than MCL injuries and often occur together with other ligament or meniscus injuries.
Typical age group: younger and middle‑aged active individuals (but can occur at any age after falls or accidents)
Typical pain location: outer and posterolateral side of the knee
Mechanism of Injury
LCL injuries usually occur after a direct blow to the inner side of the knee, forcing the joint outward into varus. This mechanism is common in contact sports such as football, handball, and basketball. Outside of sports, LCL tears may occur during falls from height or traffic accidents. Because the LCL is part of the posterolateral corner (PLC), injuries often involve multiple structures.
Symptoms
Patients typically experience sharp pain on the outer side of the knee, often accompanied by swelling and bruising. In some cases, tingling or weakness in the foot may occur, suggesting involvement of the peroneal nerve. Instability may be present, especially in higher‑grade injuries.
Diagnosis
Diagnosis is based on clinical examination and imaging. The varus stress test is the key clinical test for assessing LCL integrity. Injuries are classified into Grade I–III depending on joint opening and end‑feel. MRI is the preferred imaging method because it can evaluate the LCL and detect associated injuries (ACL, PCL, PLC, meniscus). Ultrasound is a useful alternative for real‑time assessment.
Treatment
Treatment depends on injury severity and associated damage. Unlike MCL injuries, LCL tears do not heal reliably on their own.
- Grade I–II isolated injuries may be treated conservatively with bracing and structured rehabilitation.
- Grade III injuries or those involving PLC, ACL, or PCL typically require early surgical reconstruction to restore stability. Rehabilitation focuses on gradual loading, strengthening, and restoring full function.
4. Posterior Cruciate Ligament (PCL) Injury
The posterior cruciate ligament (PCL) is one of the four major ligaments of the knee. Together with the ACL, it forms an “X” inside the joint and prevents the tibia from moving backward relative to the femur. The PCL is thicker and up to twice as strong as the ACL, which is why PCL injuries are the least common of all major knee ligament injuries.
Typical age group: younger and middle‑aged active individuals (but can occur at any age after falls or accidents)
Typical pain location: back (posterior) side of the knee
Mechanism of Injury
PCL injuries occur when a strong force pushes the tibia backward while the knee is bent. This often happens during car accidents when the knee hits the dashboard, or during falls onto a flexed knee. In sports, PCL injuries are seen in football, skiing, and baseball. Overall, the most common causes are traffic accidents (≈45%) and sports injuries (≈40%).
Symptoms
Patients typically report sudden posterior knee pain, swelling, and a feeling of instability. A “pop” may or may not be present — unlike ACL injuries, where it is more common. Walking downhill or descending stairs may worsen symptoms due to increased posterior tibial translation.
Diagnosis
Diagnosis is based on clinical examination and MRI. The posterior drawer test is the key clinical test for assessing PCL integrity. MRI provides a highly accurate assessment of the ligament and can identify associated injuries to other knee structures.
Treatment
The PCL has a greater ability to heal compared to the ACL.
- Isolated low‑grade injuries with minimal instability are typically treated conservatively with physical therapy focused on strengthening and neuromuscular control.
- Surgical treatment is considered for combined injuries, chronic instability, or in highly active individuals with significant functional demands. Rehabilitation aims to restore stability, strength, and full knee function.
5. Acute Meniscus Tear
The meniscus is a C‑shaped cartilage structure located between the femur and tibia. Each knee has a medial and lateral meniscus, which together cover about 70% of the tibial surface. Their main roles are load distribution, shock absorption, and joint stability. Meniscus tears are common in sports such as football, rugby, basketball, skiing, and wrestling, and are more frequent in the medial than the lateral meniscus.
Typical age group: younger and middle‑aged active individuals
Typical pain location: inner side (medial tear) or outer side (lateral tear)
Mechanism of Injury
Meniscus tears occur due to rotational or shear forces on a loaded, flexed knee — for example during squatting, kneeling, lifting heavy loads, or sudden changes of direction. In football, a typical mechanism is a sharp pivot or stop with the knee bent. Meniscus tears may occur in isolation or together with MCL or ACL injuries.
Symptoms
Symptoms vary depending on tear type and location. Patients commonly report medial or lateral knee pain, often accompanied by gradual swelling over 24 hours and a feeling of stiffness. Mechanical symptoms such as clicking, catching, locking, or difficulty fully straightening the knee are characteristic of meniscus injury.
Diagnosis
Clinical examination usually reveals joint‑line tenderness and swelling. Special tests such as the Thessaly test, McMurray test, and Apley test help identify meniscus pathology. MRI is the most accurate imaging method for confirming a tear. Ultrasound is generally not useful for diagnosing meniscus injuries.
Treatment
Initial management includes rest, elevation, ice, and short‑term pain relief. After symptoms settle, physical therapy is recommended to restore strength and mobility. If pain, swelling, or mechanical symptoms persist despite rehabilitation, surgical treatment may be considered. Options include meniscus repair (preferred when possible) or partial meniscectomy. Repair is favored because removing meniscus tissue increases the long‑term risk of knee osteoarthritis.
If you want to understand meniscus injuries in more detail, explore our dedicated guide here: Meniscal Tears – Symptoms, Diagnosis, and Recovery.
Overuse Syndromes (Grouped by Pain Location)
Overuse syndromes of the knee are a group of conditions caused by repetitive stress and overload of knee structures, most commonly during sports activities. The location of pain usually corresponds to the anatomical structure that is irritated or inflamed, which helps narrow down the likely cause.
Anterior Knee Pain (Front of the Knee)
Anterior knee pain is typically felt at the front of the knee, either below the kneecap or around the kneecap, and is especially common in active individuals. It typically arises from irritation of structures around the patella and is closely linked to activities involving squatting, running, jumping, or prolonged sitting.
6. Patellofemoral Pain Syndrome (“Runner’s Knee”)
Patellofemoral pain syndrome is one of the most common causes of anterior knee pain, especially in adolescents, young adults, and active individuals. It develops when the tissues around or behind the patella become irritated due to overload, poor movement mechanics, or training errors. Chondromalacia patellae refers specifically to cartilage softening or damage on the back side of the patella — i.e., a structural finding — and should not be used as a synonym for patellofemoral pain syndrome.
Typical age group: adolescents, young adults, active women
Typical pain location: front of the knee
Cause
There is no single universally accepted cause. Instead, several contributing factors increase the likelihood of developing patellofemoral pain:
- Lower‑limb alignment issues — altered patellar tracking or anatomical variations
- Muscle imbalance or tightness — quadriceps, hip abductors, hamstrings, IT band
- Overuse and training errors — sudden increases in running, jumping, or squatting
- Trauma — direct impact or fall onto the knee
Symptoms
The main symptom is pain at the front of the knee, typically aggravated by squatting, running, climbing stairs, or prolonged sitting (“movie sign”). The pain is often diffuse and discribed as pain around or behind the kneecap. Swelling is uncommon.
Diagnosis
Diagnosis is clinical, based on characteristic symptoms and physical examination. Imaging is usually not required but may be used to rule out other causes of anterior knee pain such as patella bipartita, occult fractures, loose bodies, or early osteoarthritis.
Treatment
Management is primarily conservative and focuses on:
- Physical therapy — strengthening hip and quadriceps muscles, improving patellar tracking
- Activity modification — reducing aggravating loads and correcting training errors
The goal is to reduce pain, normalize patellar movement, and restore full activity. Surgical treatment is rarely required.
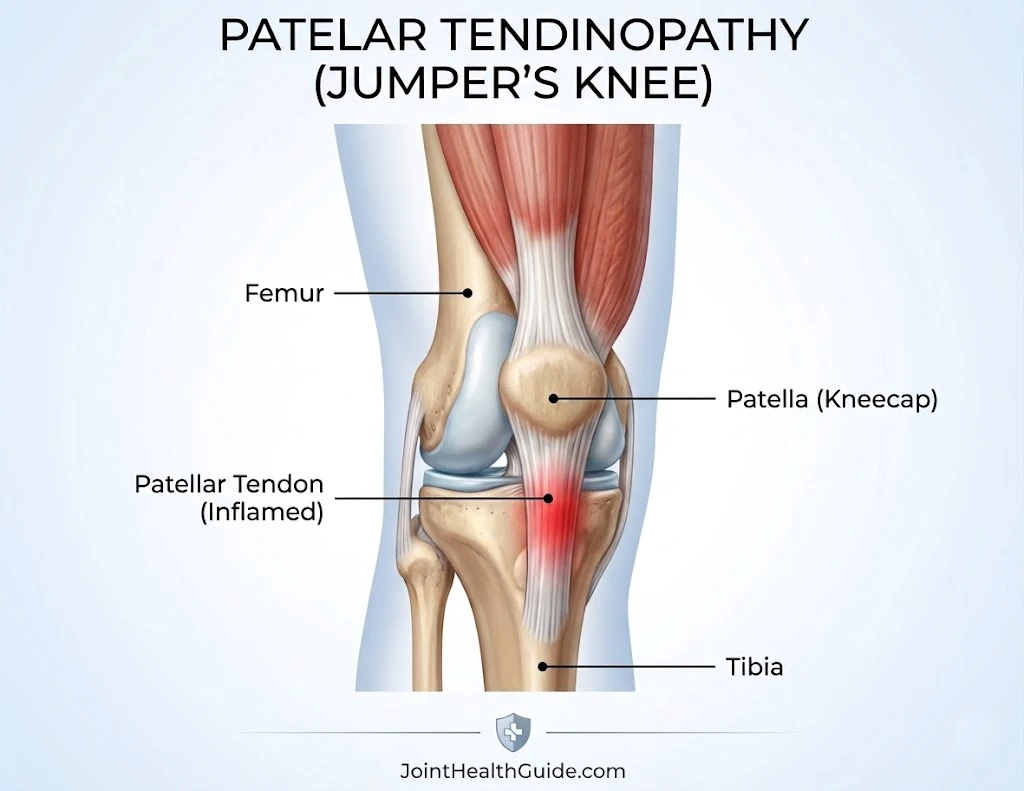
7. Patellar Tendinopathy (“Jumper’s Knee”)
Patellar tendinopathy, commonly known as jumper’s knee, is an overuse condition caused by irritation and excessive loading of the patellar tendon. It occurs in both professional and recreational athletes and is a frequent source of anterior knee pain, especially in sports involving repetitive jumping such as volleyball and basketball.
Typical age group: adolescents, young adults, active athletes (more common in males)
Typical pain location: front of the knee, below the kneecap (patellar tendon)
Cause
Patellar tendinopathy develops due to repetitive overload of the patellar tendon during activities such as jumping, landing, accelerating, decelerating, and rapid direction changes. Key contributing mechanisms include:
- High repetitive load on the patellar tendon during jumping sports
- Micro‑tears at the tendon insertion on the inferior pole of the patella
- Chronic overload leading to tendon degeneration (tendinosis)
- Biomechanical factors such as weak gluteal muscles, tight quadriceps, or altered landing mechanics
Over time, degenerative changes weaken the tendon and reduce its ability to tolerate load.
Symptoms
The main symptom is pain at the front of the knee, especially pain below the kneecap, which worsens with squatting, stair climbing, jumping, or sprinting. During sports, athletes often feel a sharp, localized pain during explosive movements. After training, pain may persist for hours or even days.
Diagnosis
Diagnosis is based on history and clinical examination. Typical findings include:
- Tenderness directly over the patellar tendon
- Local swelling or thickening of the tendon
- Pain on resisted knee extension
Ultrasound is very useful for assessing tendon structure and the degree of degeneration. MRI is rarely required.
Treatment
Patellar tendinopathy can be challenging to treat because symptoms may persist for months. Evidence‑based management includes:
- Relative rest (not full immobilization) to prevent muscle and tendon weakening
- Ice and load reduction in early phases
- Specific exercise therapy — especially eccentric and heavy‑slow resistance training, which are the cornerstone of recovery
- PRP injections under ultrasound guidance for chronic cases
Corticosteroid injections are not recommended. Surgery is considered only when conservative treatment fails and involves removing degenerated tendon tissue.
If you want to explore anterior knee pain in more detail, visit our full guide here: Anterior Knee Pain: 10 Conditions That Cause Kneecap Pain and Their Key Symptoms .
Medial Knee Pain (Pain on the Inside of the Knee)
Medial knee pain refers to discomfort felt along the inner side of the knee, where several key structures absorb load during walking, running, and twisting movements. Pain in this region is most commonly linked to irritation or overload of structures such as the medial plica, pes anserine bursa, or the medial collateral ligament.
8. Plica Syndrome
A plica is a fold of synovial tissue inside the knee joint. It is a normal anatomical structure present in many people, but when irritated or thickened due to overuse, it can become painful and inflamed. Although a plica itself is harmless, repetitive stress can cause it to rub between the femur and the patella, leading to medial or anterior knee pain.
Typical age group: adolescents, young adults, and active individuals
Typical pain location: front or inner side of the knee
Cause
Plicae develop during fetal growth and normally regress before birth, but in up to 50% of people, remnants persist into adulthood. A plica does not cause symptoms unless it becomes irritated. Repetitive knee flexion and extension — common in running, cycling, and sports involving frequent bending — can cause the plica to become inflamed and thickened, leading to pain as it gets caught between the patella and femur.
Symptoms
Patients typically report:
- Pain at the front or inner side of the knee
- A sensation of clicking, snapping, or catching during movement
- Pain during activities such as rising from a chair, squatting, or climbing stairs
- Occasional swelling or tenderness along the medial side of the patella
Diagnosis
On examination, the plica may sometimes be felt as a tender band of tissue along the inner side of the knee. Ultrasound and MRI can visualize the plica, but they are not always necessary. A definitive diagnosis can be made with arthroscopy, although this is reserved for persistent or unclear cases.
Treatment
Most cases are treated conservatively, focusing on reducing irritation and improving knee mechanics:
- Stretching and strengthening exercises for the lower limb
- NSAIDs and ice to reduce inflammation
- Activity modification to avoid repetitive stress
If symptoms persist, corticosteroid injections into the plica may help reduce inflammation. In rare, resistant cases, arthroscopic removal
9. Pes Anserine Bursitis
Pes anserine bursitis is an inflammatory condition affecting the pes anserine bursa, a small fluid‑filled sac located about 5 cm below the inner side of the knee. This bursa lies between the hamstring tendons (semitendinosus, gracilis, sartorius) and the medial collateral ligament, allowing smooth gliding during movement. When irritated, the bursa becomes inflamed and swollen, causing medial knee pain.
Typical age group: middle‑aged adults, more common in women with excess body weight Typical pain location: inner side of the knee, slightly below the joint line
Cause
Pes anserine bursitis most often occurs in individuals who already have underlying knee issues. Unlike many overuse syndromes, it is less common in highly active athletes, though physical activity can still trigger irritation. Common contributing factors include:
- Knee osteoarthritis
- Medial meniscus pathology
- Valgus knee alignment (knock‑knees)
- Excess body weight increasing stress on the medial knee
- Hamstring tightness or altered gait mechanics
These factors increase friction between the hamstring tendons and the bursa, leading to inflammation.
Symptoms
Typical symptoms include:
- Sharp pain on the inner side of the knee, especially when climbing stairs, standing up, or sitting cross‑legged
- Localized tenderness about 5 cm below the medial joint line
- Mild swelling or redness over the bursa
- Pain that worsens with repetitive knee flexion or prolonged walking
Diagnosis
Diagnosis is primarily clinical, based on characteristic pain location and tenderness. Ultrasound or MRI may be used in unclear cases to visualize the bursa and hamstring tendons, but imaging is not always necessary.
Treatment
Most cases improve with conservative management, including:
- Rest and activity modification
- Ice and analgesics to reduce pain and inflammation
- Physical therapy focusing on hamstring stretching and strengthening
- Therapeutic modalities such as ultrasound, LASER, or shockwave therapy
If symptoms persist, corticosteroid injection under ultrasound guidance may provide relief. Surgery is rarely required.
If you want to explore inner knee pain in more detail, visit our dedicated guide here: Medial (Inner) Knee Pain: A Guide to Possible Diagnoses and Treatments.
Lateral Knee Pain (Pain on the Outside of the Knee)
Lateral knee pain refers to discomfort felt along the outer side of the knee, most often caused by irritation of structures such as the iliotibial band, lateral collateral ligament, or lateral meniscus, especially during running, downhill walking, or repetitive bending and straightening of the knee.
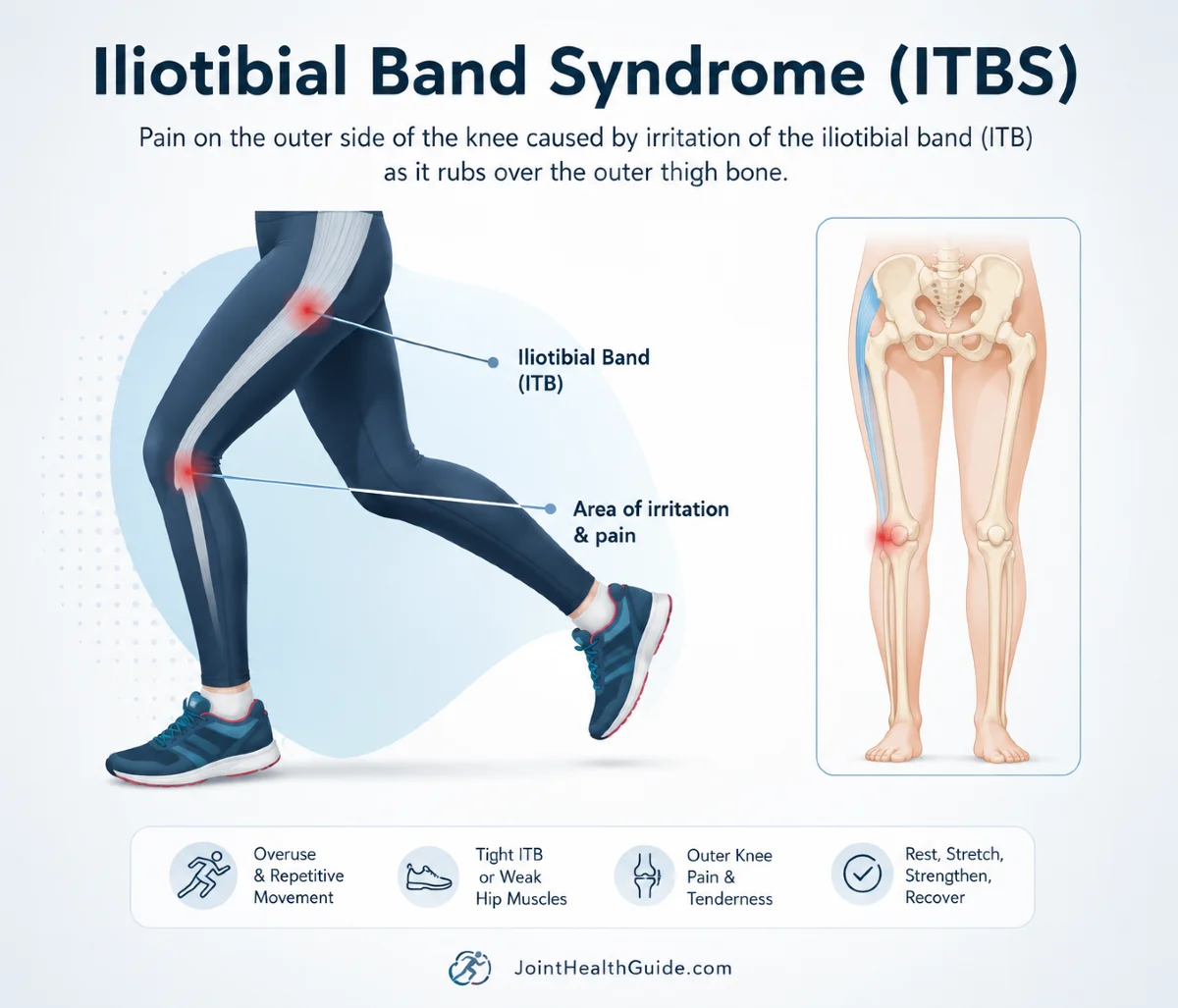
10. Iliotibial Band Syndrome (ITB Syndrome)
Iliotibial Band Syndrome is an overuse injury and the most common cause of pain on the outside (lateral side) of the knee. It is frequently seen in runners and cyclists, but also in athletes involved in sports such as tennis, football, skiing, and weightlifting.
Typical age group: young and middle‑aged active individuals (especially runners and cyclists)
Typical pain location: outer (lateral) side of the knee
Cause
ITB Syndrome is believed to occur due to repetitive friction between the iliotibial band (ITB) and the lateral femoral epicondyle during knee flexion and extension. The ITB is a thick band of connective tissue running along the outside of the thigh from the hip to the shin.
Repetitive rubbing during activities like running or cycling leads to irritation, inflammation, and pain at the point where the ITB crosses the outer femur.ITB Syndrome is also associated with altered hip biomechanics and increased ITB tension, and often coexists with greater trochanteric pain syndrome.
Symptoms
Patients typically report:
- Sharp or burning pain on the outer side of the knee, a few centimeters above the joint line
- Pain that worsens with activity, especially running downhill, climbing stairs, or prolonged cycling
- Tenderness over the lateral femoral epicondyle
- Occasionally mild soft‑tissue swelling without true joint effusion
Diagnosis
Diagnosis is usually clinical, based on typical symptoms and physical examination. Findings may include:
- Localized tenderness about 3 cm above the lateral joint line
- Pain reproduced during single‑leg squat or running‑specific tests
- Soft‑tissue swelling over the ITB insertion
Ultrasound or MRI may show thickening and inflammation of the ITB at the point of friction, but imaging is not always required.
Treatment
Management begins with rest from aggravating activities. Running or cycling should be avoided as long as pain persists during activity or palpation.
Effective treatment strategies include:
- Physical therapy focused on ITB stretching and hip strengthening
- Manual therapy such as myofascial release
- Activity modification and gradual return to sport
If symptoms do not improve with conservative therapy, a corticosteroid injection may be considered. Surgical treatment is rarely necessary.
Degenerative & Inflammatory Conditions
Degenerative and inflammatory knee conditions typically develop gradually, often due to age‑related cartilage wear, chronic overload, or immune‑mediated inflammation. These disorders commonly cause stiffness, swelling, and deep aching pain, and may affect multiple knee structures at once, making them a frequent source of persistent knee discomfort.
11. Knee Osteoarthritis (Gonarthrosis)
Knee osteoarthritis is a degenerative joint disease characterized by the progressive breakdown of knee cartilage, inflammation of the joint, and later the formation of bony spurs (osteophytes). It is the most common form of knee arthritis and the leading cause of knee pain in older adults.
Typical age group: adults over 50
Typical pain location: the whole knee, most commonly the medial (inner) side
Cause
Knee osteoarthritis develops slowly over many years through a combination of mechanical wear and complex biological changes within the joint. Early in the process, inflammatory cytokines disrupt normal cartilage metabolism, leading to loss of proteoglycans, increased water content, and disorganization of collagen fibers.
As cartilage becomes less elastic, it begins to crack and erode. With further progression, the joint loses its ability to absorb shock, causing increased stress on the underlying bone, which responds by thickening and forming osteophytes. At the same time, synovial inflammation accelerates tissue breakdown and contributes to pain, creating a self‑perpetuating cycle of degeneration and inflammation.
Symptoms
- Activity‑related knee pain, especially with walking, kneeling, or climbing stairs
- Pain relief with rest; in later stages, pain may occur even at rest
- Stiffness, especially after inactivity
- Reduced walking tolerance and difficulty with daily activities
- Episodes of swelling (“inflammatory flares”)
- Progressive loss of mobility and function
Diagnosis
Diagnosis is based on symptoms, age, physical examination, and imaging. X‑ray is the standard tool for confirming and grading osteoarthritis, showing joint space narrowing, osteophytes, and subchondral bone changes.
Treatment
- Physical therapy to improve strength and mobility
- Analgesics and NSAIDs for symptom relief
- Knee braces to reduce load and improve stability
- Injections (corticosteroids, hyaluronic acid, PRP) for symptom control
If conservative treatment fails and symptoms significantly impair quality of life, total knee replacement becomes the most effective long‑term solution.
If you want to learn more about knee osteoarthritis (gonarthrosis), including its symptoms, causes, diagnosis, and treatment options, visit our dedicated guide here: Knee Osteoarthritis (Gonarthrosis): Symptoms, Causes, and Treatment.
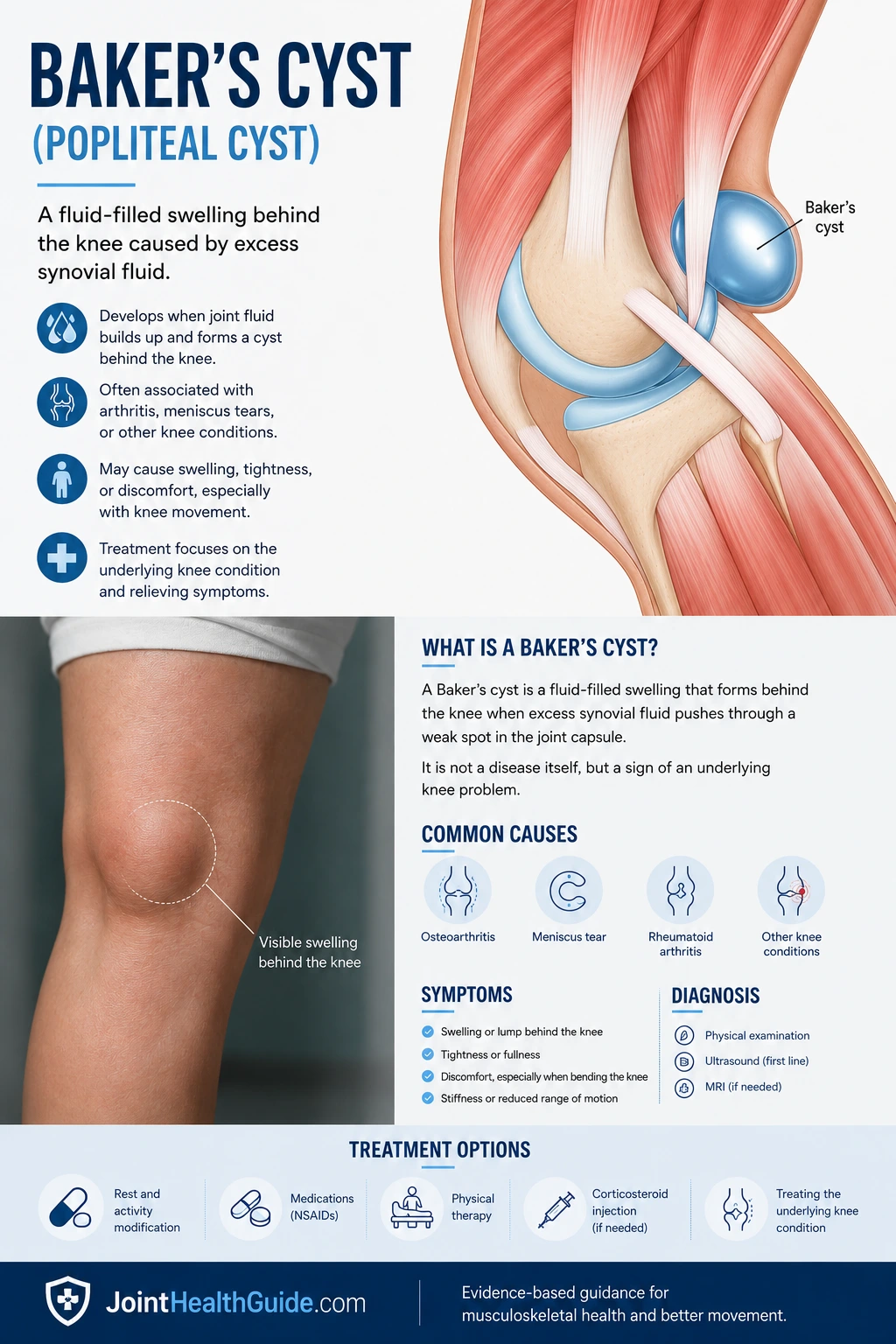
12. Baker’s Cyst (Popliteal Cyst)
A Baker’s cyst, also known as a popliteal cyst, is a fluid‑filled swelling that develops behind the knee. It usually forms due to excess accumulation of synovial fluid within the knee joint, often secondary to conditions such as arthritis or internal knee injury. It is most common in adults over 40 and can cause posterior knee pain or a feeling of tightness.
Typical age group: adults over 50
Typical pain location: back of the knee
Cause
A Baker’s cyst develops when increased intra‑articular pressure forces synovial fluid from the knee joint into the popliteal bursa, creating a one‑way valve effect that traps fluid behind the knee. In some cases, the cyst forms directly from an outpouching of the joint capsule due to elevated pressure. Underlying causes often include knee arthritis, meniscal tears, or other conditions that lead to joint effusion.
Symptoms
Baker’s cysts are often asymptomatic, but when symptoms occur, they may include:
- A feeling of fullness or tightness behind the knee
- Pain or stiffness during movement or prolonged standing
- Visible swelling in the popliteal area
- Occasionally, symptoms resembling deep vein thrombosis if the cyst ruptures and fluid leaks into the calf
Diagnosis
Diagnosis is typically made through clinical examination and patient history. Imaging methods such as ultrasound or MRI confirm the presence of the cyst and help rule out other causes of posterior knee swelling.
Treatment
Treatment focuses on managing the underlying knee condition that causes fluid buildup. Conservative measures include:
- Rest and cold compresses
- NSAIDs for pain and inflammation
- Physical therapy to improve joint mechanics
For persistent cases, aspiration of the cyst combined with corticosteroid injection under ultrasound guidance can relieve symptoms, though recurrence is possible. Surgical removal is reserved for chronic or complicated cases unresponsive to conservative therapy.
If you want to learn more about a Baker’s cyst (popliteal cyst), including its symptoms, causes, diagnosis, and treatment options, visit our dedicated guide here: Baker’s Cyst (Swelling Behind the Knee): Symptoms, Causes, and Treatment.
13. Rheumatoid Arthritis (RA)
Rheumatoid arthritis is one of the most well‑known rheumatic diseases. It is a systemic autoimmune disorder characterized by chronic inflammation of the joints and, in many cases, involvement of tissues outside the joints. RA typically begins in the small joints of the hands and feet, but as the disease progresses, larger joints such as the knee may also become affected. Persistent inflammation leads to cartilage loss, bone erosion, joint deformity, and reduced function.
Typical age group: most common between ages 60–80, but can occur at any adult age; more common in women
Typical pain location: the entire knee joint
Cause
Rheumatoid arthritis develops due to a combination of genetic susceptibility and environmental triggers that activate an autoimmune response. The immune system produces autoantibodies that attack the synovial membrane, causing it to thicken and form a destructive tissue called pannus. This pannus invades cartilage and bone, leading to progressive joint destruction. Inflammatory cytokines such as TNF‑α, IL‑1, and IL‑6 stimulate osteoclast activity, resulting in bone erosion and irreversible structural damage. Over time, this process causes pain, swelling, deformity, and loss of joint function.
Symptoms
- Pain, swelling, and warmth in affected joints
- Gradual onset over weeks to months (occasionally sudden)
- Early involvement of small joints of the hands and feet, later spreading to larger joints such as the knee
- Morning stiffness lasting more than 30–60 minutes
- More pronounced and abundant knee effusion compared to osteoarthritis
- Warm skin over the knee due to active inflammation
- Progressive loss of mobility and function if untreated
Diagnosis
Diagnosis is based on a combination of:
- Clinical symptoms (pain, swelling, stiffness)
- Laboratory tests: rheumatoid factor (RF), anti‑CCP antibodies, elevated CRP and ESR
- Imaging: X‑ray, ultrasound, or MRI showing joint erosions, synovitis, and structural damage
Treatment
Treatment focuses on controlling inflammation, preventing joint damage, and maintaining function. Common approaches include:
- DMARDs (e.g., methotrexate) to slow disease progression
- Biologic therapies targeting inflammatory cytokines
- Analgesics and NSAIDs for symptom relief
- Physical therapy to maintain mobility and strength
- Corticosteroid injections
14. Gout (Uric Acid Arthritis)
Gout — also called uric acid arthritis or podagra — is an inflammatory joint disease caused by the deposition of monosodium urate crystals in joints and surrounding tissues. It is the most common form of inflammatory arthritis, characterized by sudden, extremely painful attacks of joint inflammation. If untreated, gout can progress into a chronic form with the development of larger crystal deposits called tophi.
Typical age group: adults of all ages, more common in older adults and men
Typical pain location: the entire knee (when the knee is affected)
Cause
Gout develops when uric acid levels in the blood become elevated (hyperuricemia). Uric acid is a normal metabolic by‑product, but when its concentration exceeds the solubility threshold, needle‑shaped crystals begin to deposit in joints and soft tissues. Hyperuricemia may result from overproduction of uric acid (e.g., high‑purine diet, cell turnover) or, far more commonly (≈90% of cases), from reduced renal excretion. Although hyperuricemia is the main risk factor, not all individuals with high uric acid develop gout, indicating a complex interplay of metabolic, genetic, and environmental factors.
Symptoms
- Sudden onset of severe pain, swelling, redness, and warmth in the affected joint
- Most commonly affects the first MTP joint (big toe), but the knee is also frequently involved
- Symptoms peak within 12–24 hours
- Pain is often so intense that even light touch is unbearable
- Attacks may be accompanied by fever, malaise, and systemic discomfort
- Chronic gout may lead to tophi — visible or palpable urate deposits around joints
Diagnosis
Diagnosis is confirmed by identifying monosodium urate crystals in synovial fluid using polarized light microscopy, where crystals appear as needle‑shaped with strong negative birefringence. Additional supportive findings include:
- Elevated inflammatory markers (CRP, ESR)
- Leukocytosis
- Elevated serum uric acid (often measured after the acute attack resolves)
Treatment
Management has two goals:
- Control inflammation during acute attacks
- Lower uric acid levels long‑term to prevent future attacks and dissolve tophi
Treatment strategies include:
- NSAIDs, colchicine, or systemic corticosteroids for acute flare control
- Urate‑lowering therapy (e.g., allopurinol, febuxostat) for long‑term management
- Preventive therapy during initiation of urate‑lowering treatment (often low‑dose colchicine or NSAIDs)
- Lifestyle adjustments such as reducing purine‑rich foods, alcohol moderation, and weight management
Conclusion
A few practical takeaways to wrap things up. This guide has hopefully helped you orient yourself and better understand the possible causes of knee pain. Some conditions — especially early‑stage overuse syndromes — can often be managed at home with activity modification, cold packs, and over‑the‑counter pain relief.
For an accurate diagnosis and a targeted treatment plan, it’s important to see a medical professional. If you’ve experienced a knee injury or trauma, an orthopaedic surgeon or traumatologist should evaluate whether surgical treatment is needed. For non‑surgical knee injuries, a physiatrist is the right specialist to guide rehabilitation and create an individualized recovery plan — including after knee surgery.
For knee pain not caused by trauma (such as overuse syndromes, knee osteoarthritis, or gout), consulting a physiatrist is the best next step, as they can determine the underlying issue and guide you toward effective treatment.
Casadei K, Hermena S. Plica Syndrome. StatPearls Publishing. StatPearls review: Plica syndrome diagnosis and management
Raj MA, Bubnis MA. Knee Meniscal Tears. StatPearls Publishing. StatPearls review: Meniscal tear evaluation and treatment
Yaras RJ, O’Neill N, Mabrouk A, et al. Lateral Collateral Ligament Knee Injury. StatPearls Publishing. StatPearls review: LCL injury diagnosis and rehabilitation
Nacey NC, Geeslin MG, Miller GW, Pierce JL. Magnetic Resonance Imaging of the Knee: An Overview and Update of Conventional and State of the Art Imaging. Journal of Magnetic Resonance Imaging. MRI review: Modern imaging techniques for knee disorders
Bunt CW, Jonas CE, Chang JG. Knee Pain in Adults and Adolescents: The Initial Evaluation. American Family Physician. Clinical guide: Initial assessment and differential diagnosis of knee pain
Kim IJ, Kim HA, Seo YI, et al. Prevalence of Knee Pain and Its Influence on Quality of Life and Physical Function in the Korean Elderly Population. Journal of Korean Medical Science. Epidemiology study: Impact of knee pain on quality of life and physical function
Calmbach WL, Hutchens M. Evaluation of Patients Presenting with Knee Pain: Part I. American Family Physician. Clinical review: History, physical examination, and diagnostic testing for knee pain
Koplas M, Schils J, Sundaram M. The Painful Knee: Choosing the Right Imaging Test. Cleveland Clinic Journal of Medicine. Imaging guide: Selecting appropriate imaging studies for knee disorders
Jacobson JA, Ruangchaijatuporn T, Khoury V, Magerkurth O. Ultrasound of the Knee: Common Pathology Excluding Extensor Mechanism. Seminars in Musculoskeletal Radiology. Ultrasound guide: Common knee pathologies and sonographic findings
Evans J, Mabrouk A, Nielson JL. Anterior Cruciate Ligament Knee Injury. StatPearls Publishing. StatPearls review: ACL injury diagnosis, treatment, and rehabilitation
Naqvi U, Sherman AL. Medial Collateral Ligament Knee Injury. StatPearls Publishing. StatPearls review: MCL injury evaluation and management
Raj MA, Mabrouk A, Varacallo MA. Posterior Cruciate Ligament Knee Injuries. StatPearls Publishing. StatPearls review: PCL injury diagnosis and treatment options
Bump JM, Lewis L. Patellofemoral Syndrome. StatPearls Publishing. StatPearls review: Patellofemoral pain syndrome diagnosis and management
Mabrouk A, Lee CYM, Sherman AL. Patellar Tendinopathy (Jumper’s Knee). StatPearls Publishing. StatPearls review: Patellar tendinopathy causes, diagnosis, and treatment
Mohseni M, Mabrouk A, Li D. Pes Anserine Bursitis. StatPearls Publishing. StatPearls review: Pes anserine bursitis evaluation and management
Chauhan K, Jandu JS, Brent LH, et al. Rheumatoid Arthritis. StatPearls Publishing. StatPearls review: Rheumatoid arthritis clinical presentation and treatment
Menon SG, Rednam M, Gujarathi R, et al. Gout. StatPearls Publishing. StatPearls review: Gout diagnosis, acute management, and prevention
Shekelle PG, FitzGerald J, Newberry SJ, et al. Management of Gout. Agency for Healthcare Research and Quality (AHRQ). Evidence review: Comparative effectiveness of gout treatments
Lavine R. Iliotibial Band Friction Syndrome. Current Reviews in Musculoskeletal Medicine. Review article: Iliotibial band syndrome pathophysiology and treatment
D’Ambrosi R, Meena A, Raj A, Ursino N, Hewett TE. Anterior Knee Pain: State of the Art. Sports Medicine – Open. Comprehensive review: Modern concepts in anterior knee pain diagnosis and treatment

















