

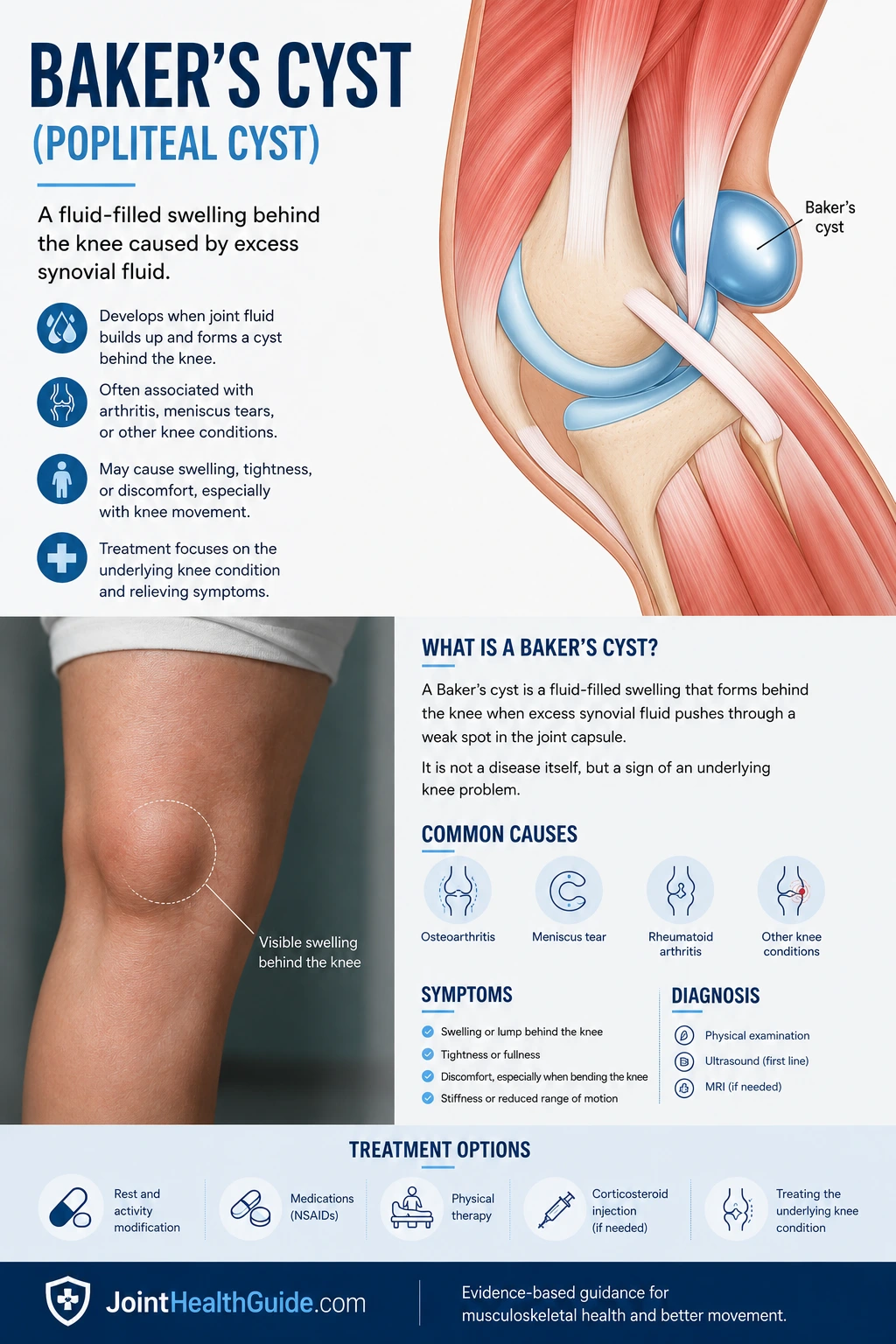
Baker’s cyst, also known as a popliteal cyst, is a fluid‑filled swelling that develops behind the knee when excess synovial fluid escapes into the popliteal space. This “cyst behind the knee” is most often linked to underlying knee problems such as osteoarthritis, meniscal tears, or inflammatory joint disease. Although it is most common in adults over 40, it can occasionally appear in children as well.
The condition typically presents as a swelling behind the knee, accompanied by tightness, discomfort, or a feeling of fullness—especially during walking, squatting, or prolonged standing. Some individuals notice only the lump without significant pain, while others experience pressure that worsens with activity. In rare cases, a Baker’s cyst may rupture, causing sudden calf pain and swelling that can closely mimic deep vein thrombosis (DVT).
In this article, readers will learn how to recognize the key symptoms of a Baker’s cyst, how doctors diagnose it, which treatment options are most effective, and—crucially—how to distinguish a Baker’s cyst from deep vein thrombosis, a condition with similar symptoms but far more serious implications.
Quick Summary – Baker’s Cyst
- Baker’s cyst is a fluid-filled swelling behind the knee caused by increased synovial fluid, most often due to arthritis or meniscal injury.
- The most common symptoms include tightness, swelling, and pain behind the knee, especially during walking, squatting, or full flexion.
- Diagnosis is based on clinical examination and confirmed with ultrasound; MRI is used when additional knee pathology is suspected.
- Conservative treatment is first-line: rest, NSAIDs, physical therapy, and activity modification. Aspiration and corticosteroid injection are used when symptoms persist.
- Surgery is rarely needed and reserved for persistent cases or when the cyst compresses nerves or blood vessels.
- Complications include rupture of the cyst and compression of neurovascular structures. Rupture causes sudden calf pain and swelling, while DVT develops more gradually.
What Is a Baker’s Cyst?
A Baker’s cyst, also called a popliteal cyst, is a fluid‑filled swelling or lump that forms behind the knee. The condition is named after British surgeon Dr. William Morrant Baker (1838–1896), who first described it. In medical terms, a cyst refers to a fluid‑filled sac within soft tissues, and in this case, the sac develops in the popliteal fossa — the hollow area at the back of the knee.
A Baker’s cyst typically appears in the center or slightly inner side of the popliteal region and is filled with thick, clear, yellowish synovial fluid that resembles gel. This fluid originates from the knee joint itself and accumulates when the joint produces more synovial fluid than it can handle — often due to arthritis, meniscal injury, or inflammation.
Although commonly associated with adults over 40, a Baker’s cyst can occasionally be seen in children as well. Regardless of age, it is one of the most frequent causes of a noticeable swelling behind the knee.
Why Does a Baker’s Cyst Develop?
To understand why a Baker’s cyst (popliteal cyst) forms, it helps to first review the basic anatomy of the knee and the structures involved in producing and regulating synovial fluid.
Knee Anatomy
The knee is a complex joint formed by the femur, tibia, and patella. It is enclosed by a strong connective‑tissue envelope called the joint capsule. The inner surface of this capsule is lined with the synovial membrane, which produces synovial fluid — a thick, lubricating fluid that reduces friction between joint surfaces and nourishes the cartilage.
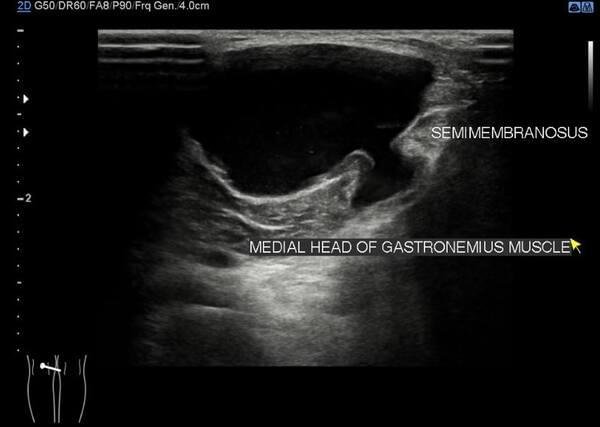
The knee also contains several bursae, which are small fluid‑filled sacs that reduce friction where tendons, muscles, or skin glide over bone. One of these is the popliteal bursa, located behind the knee between the semimembranosus tendon and the medial head of the gastrocnemius muscle. This bursa plays a key role in the formation of a Baker’s cyst.
How and Why a Baker’s Cyst Forms
A Baker’s cyst develops when there is an increased amount of synovial fluid inside the knee joint — a condition commonly referred to as knee effusion. Excess fluid is typically produced due to joint damage (meniscal tears, cartilage injury, ligament injury) or inflammation (arthritis, gout, pseudogout).
In many individuals with a Baker’s cyst, there is a communication channel — a small tunnel — between the knee joint and the popliteal bursa. When pressure inside the knee rises, synovial fluid is pushed through this channel into the bursa. The surrounding muscles act like a one‑way valve, allowing fluid to move from the knee into the bursa, but not back into the joint. Over time, the bursa fills with fluid, enlarges, and becomes a popliteal cyst.
In about half of all patients, this communication is present. In others, the cyst forms due to direct bulging of the joint capsule backward into the popliteal space when intra‑articular pressure becomes too high.
Common Conditions Associated With Baker’s Cyst Formation
- Osteoarthritis of the knee
- Meniscal tears, cartilage injuries, cruciate ligament injuries
- Inflammatory arthritis (rheumatoid, psoriatic, reactive arthritis)
- Gout or pseudogout
- Knee trauma, especially in younger individuals
- Synovial disorders (synovial chondromatosis, pigmented villonodular synovitis)
All these conditions increase synovial fluid production, raise pressure inside the joint, and promote the formation of a swelling behind the knee characteristic of a Baker’s cyst.
Symptoms of a Baker’s Cyst
Some Baker’s cysts do not cause any symptoms and are discovered incidentally during a physical examination or when an ultrasound or MRI of the knee is performed for unrelated reasons. When symptoms do occur, they may include:
- A feeling of fullness or a lump behind the knee
- Pain behind the knee, sometimes radiating into the calf
- Stiffness or tightness in the back of the knee
- Swelling in the knee, swelling behind the knee, or swelling extending into the upper calf
In many cases, it can be difficult to determine whether symptoms are caused by the cyst itself or by the underlying knee condition such as arthritis or structural injury. The swelling behind the knee is usually most noticeable when standing with the knee fully extended, and it often decreases when the knee is slightly flexed to about 45 degrees.
Pain behind the knee typically worsens during walking or squatting because these movements increase pressure on the cyst. In some cases, a Baker’s cyst can limit full knee flexion or extension.
Anyone experiencing pain and swelling behind the knee should seek medical evaluation. A lump in the popliteal region can sometimes indicate a more serious condition, such as a popliteal artery aneurysm or a tumor, and should not be ignored.
Baker’s Cyst Diagnosis?
Diagnosis of a Baker’s cyst (popliteal cyst) is usually based on a combination of clinical examination, patient history, and imaging tests such as ultrasound or MRI. Because a cyst behind the knee can mimic other, more serious conditions, a careful evaluation is essential.
Clinical History and Physical Examination
Your doctor will begin by taking a detailed medical history and asking you to describe your symptoms. Important information includes previous knee injuries (such as ACL tears or meniscal injuries) and the presence of arthritis or chronic knee swelling.
During the physical examination, the doctor will compare the affected knee with the healthy one and look for:
- Swelling
- Joint instability
- Clicking or popping sounds during knee movement
- Reduced range of motion or stiffness
- A visible or palpable lump behind the knee when the leg is fully extended
A Baker’s cyst often becomes more noticeable when the knee is straight and may disappear when the knee is flexed. However, even with a thorough exam, the cyst cannot be detected by touch in up to half of all patients, especially if it is small or deep.
Imaging Tests
After the clinical exam, imaging is used to confirm the diagnosis and rule out other causes of swelling behind the knee.
- X‑ray cannot show the cyst itself, but it can reveal knee osteoarthritis, which is commonly associated with Baker’s cyst formation.
- Ultrasound is the first‑line imaging method. It is safe, accessible, and highly accurate for identifying the location, size, and shape of a Baker’s cyst. It can also distinguish the cyst from other masses such as tumors or a popliteal artery aneurysm.
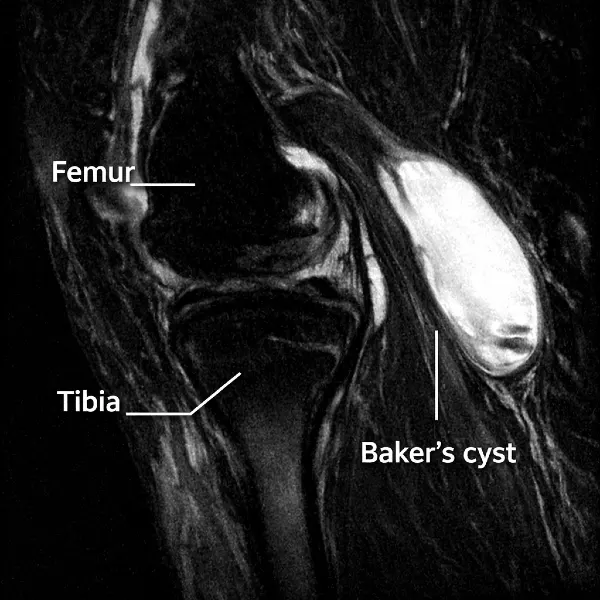
- MRI provides the most detailed view of soft tissues. Although not always necessary, it is useful when evaluating meniscal tears, ligament injuries, or other structural problems that may be causing the cyst.
Treatment of a Baker’s Cyst
Treatment for a Baker’s cyst (popliteal cyst) is not necessary if you have no symptoms. When symptoms are present, the key to successful management is addressing the underlying knee condition that caused the excess synovial fluid and the formation of the cyst. Many conservative measures can be performed at home to reduce discomfort and swelling.
Conservative (Non‑Surgical) Treatment
Conservative therapy is always the first‑line approach for managing a Baker’s cyst. Common non‑surgical strategies include:
- Rest and activity modification — reducing activities that worsen swelling, using compression bandages, and applying cold packs to decrease discomfort.
- Medications — pain relief is typically achieved with paracetamol or non‑steroidal anti‑inflammatory drugs (NSAIDs). Paracetamol has fewer side effects but is less effective for inflammation, while NSAIDs (such as ibuprofen, naproxen, diclofenac, indomethacin) reduce both pain and inflammation. These medications should be used at the lowest effective dose and for the shortest duration due to potential side effects.
- Exercise and physical therapy — stretching and strengthening exercises for the muscles around the knee can reduce symptoms. Physical therapy improves joint mobility and helps decrease swelling.
- Aspiration and corticosteroid injection — used when conservative measures fail to provide relief.
Clinical Insight
In practice, treatment usually begins with rest, cold therapy, and NSAIDs. If symptoms persist, a 2–3‑week course of physical therapy is commonly recommended. When these measures are insufficient, aspiration and corticosteroid injection are considered.
Aspiration and Corticosteroid Injection
Corticosteroids have strong anti‑inflammatory effects and are widely used in treating musculoskeletal conditions. They reduce inflammation inside the knee joint (in osteoarthritis or inflammatory arthritis), which in turn decreases the production of excess synovial fluid and reduces swelling.
A corticosteroid injection may be administered into the knee joint or directly into the cyst, ideally under ultrasound guidance.
Aspiration of a Baker’s cyst is performed by inserting a needle into the cyst under ultrasound visualization and withdrawing the fluid with a syringe. Ultrasound guidance is essential to avoid accidental injury to nearby blood vessels and nerves. After aspiration, a corticosteroid injection is often given through the same needle.
Most patients experience significant pain relief and reduction of symptoms after aspiration and corticosteroid injection. The effect typically lasts 6–9 months. However, the cyst may recur in about one‑third of patients, especially when the underlying knee damage is more severe or when the cyst has been present for a long time.
Surgical Treatment of a Baker’s Cyst
Surgery for a Baker’s cyst is reserved only for persistent, long‑lasting cases that do not respond to conservative treatment. Because a Baker’s cyst is almost always a consequence of an underlying knee problem, surgery is typically aimed at treating the primary joint pathology, not just removing the cyst itself. Two surgical approaches may be used: arthroscopy and, less commonly, open surgery.
Arthroscopy
During knee arthroscopy, the surgeon makes several small incisions and inserts a tiny camera (arthroscope) into the joint. The camera displays the inside of the knee on a monitor, allowing the surgeon to treat structural problems using miniature instruments. Arthroscopy is most often used to address meniscal tears, cartilage damage, or ligament injuries—conditions that frequently lead to excess synovial fluid and the formation of a Baker’s cyst.
By treating the underlying cause, arthroscopy helps reduce fluid production inside the joint, which in turn decreases the size of the cyst or allows it to resolve naturally.
Open Surgery
In rare cases—typically when the cyst is very large, causes compression of nerves or blood vessels, or does not improve despite all other treatments—an open surgical procedure may be required. This approach allows the surgeon to remove the entire cyst directly. Open surgery is less common today because most Baker’s cysts improve once the underlying knee disorder is treated.
Why Treating the Underlying Knee Problem Matters?
For all patients with symptomatic Baker’s cysts, it is essential to identify and treat the primary joint disorder. Whether the issue is osteoarthritis, a meniscal tear, or inflammatory arthritis, addressing the root cause reduces synovial fluid production and prevents the cyst from enlarging again.
Complications of a Popliteal Cyst
Complications of a popliteal cyst are fortunately uncommon, but when they do occur, they can cause significant symptoms and require prompt medical attention. The two most frequent complications are compression of nearby nerves and blood vessels and rupture of the cyst.
Compression of Blood Vessels and Nerves
A large popliteal cyst can press on surrounding neurovascular structures due to its size and location. This may lead to:
- Superficial thrombophlebitis — inflammation and clotting in the superficial veins of the calf
- Compression of the tibial nerve — causing calf and foot weakness, numbness, or sharp, electric‑like pain radiating down the leg
- Swelling of the lower leg due to compression of the deep veins, which can resemble deep vein thrombosis (DVT)
- In rare cases, compression of the popliteal artery
If compression of nerves or blood vessels is confirmed, surgical removal of the cyst is usually required to prevent permanent damage.
Ruptured Baker’s Cyst
Rupture of a Baker’s cyst is far more common than neurovascular compression. It occurs when pressure inside the cyst becomes too high or changes suddenly. When the cyst ruptures, its fluid (often mixed with a small amount of blood) leaks into the soft tissues of the calf, triggering inflammation.
Typical symptoms of ruptured popliteal cyst include:
- Sudden, sharp pain in the knee or calf
- Swelling or redness of the calf
- A sensation of fluid “running down” the leg
- Symptoms that closely mimic DVT or an acute calf muscle tear
Because deep vein thrombosis is a medical emergency, any suspicion of DVT requires immediate evaluation, including blood tests and ultrasound of the leg veins.
Treatment of a Ruptured Baker’s Cyst
Management is conservative and focuses on reducing inflammation:
- Rest and reduced physical activity
- Cold compresses applied to the calf
- Anti‑inflammatory medications and analgesics
- Compression bandage if calf swelling is significant
Symptoms typically improve gradually over 2–3 weeks.
Summary
Baker’s cyst is a fluid‑filled swelling behind the knee most often caused by arthritis, meniscal injury, or other conditions that increase synovial fluid production. Symptoms range from mild tightness to significant pain and swelling behind the knee, especially during walking or squatting. Diagnosis relies on clinical examination supported by ultrasound or MRI, which help confirm the cyst and rule out other causes of a popliteal mass.
Most patients improve with conservative treatment, including rest, NSAIDs, physical therapy, and—when necessary—aspiration and corticosteroid injection. Surgery is reserved for persistent cases or when the cyst compresses nearby nerves or blood vessels. Complications such as rupture of the cyst can closely resemble deep vein thrombosis (DVT), making accurate assessment essential.
In the FAQ section, readers will learn how to distinguish a ruptured Baker’s cyst from DVT, how to tell the difference between a ruptured Baker’s cyst and a calf muscle tear
Frequently Asked Questions (FAQ)
1. How dangerous is a Baker’s cyst?
A Baker’s cyst is usually not dangerous, but it can cause discomfort such as pain, swelling, and tightness behind the knee. If the cyst ruptures, fluid can leak into the calf and cause sudden pain and swelling that may resemble thrombophlebitis or even deep vein thrombosis (DVT). In rare cases, a large cyst may compress nearby nerves or blood vessels, which requires prompt medical evaluation. Treating the underlying knee condition (arthritis, meniscal tear, inflammation) is essential to prevent the cyst from enlarging or recurring.
2. Baker’s cyst vs. deep vein thrombosis (DVT) — what’s the difference?
A Baker’s cyst and DVT can share very similar symptoms, making differentiation challenging.
Similarities:
- calf pain
- swelling of the lower leg
- tightness or heaviness
- redness and warmth (especially after cyst rupture)
Differences:
- A Baker’s cyst is a collection of synovial fluid, while DVT is a blood clot in a deep vein.
- A ruptured Baker’s cyst typically causes a sudden onset of sharp calf pain, followed by swelling and discomfort in the lower leg.
- DVT can also cause calf pain and swelling, but symptoms usually develop more gradually and not as abruptly as in an acute cyst rupture.
Diagnosis: A venous ultrasound is the fastest and most reliable way to distinguish between the two. If DVT is suspected, urgent medical assessment is required.
3. What else can cause pain behind the knee besides a Baker’s cyst?
Pain behind the knee can be caused by several conditions, including:
- gastrocnemius tendinitis
- meniscal tear
- posterior cruciate ligament (PCL) injury
- osteoarthritis or rheumatoid arthritis
- hamstring strain or tightness
- meniscal cyst
- deep vein thrombosis (DVT)
- bursitis
Each condition requires a different treatment approach, so accurate diagnosis is important.
4. What is the difference between a ruptured Baker’s cyst and a calf muscle tear?
A ruptured Baker’s cyst and a calf muscle tear (most commonly the medial head of the gastrocnemius) can look almost identical, especially because both occur suddenly during activity and cause sharp, acute calf pain.
Similarities:
- sudden onset of severe pain
- swelling and tenderness
- difficulty walking
- a “popping” or “snapping” sensation at the moment of injury
Differences:
- A ruptured Baker’s cyst often causes diffuse swelling and a sensation of fluid spreading down the calf.
- A calf muscle tear usually has a localized point of maximal tenderness, and sometimes a palpable defect in the muscle.
In real‑world practice, it is often impossible to reliably distinguish the two without ultrasound imaging, which is the quickest and most accurate diagnostic method.
Handy JR. Popliteal cysts in adults: a review. Seminars in Arthritis and Rheumatism. Review: Pathophysiology and clinical relevance of Baker’s (popliteal) cysts
Leib AD et al. Baker’s Cyst. StatPearls Publishing. Evidence-based overview: Diagnosis, imaging, and management of Baker’s cyst
Stroiescu AE et al. Ultrasound and fluoroscopic-guided aspiration and injection treatment of symptomatic Baker’s cysts. Ulster Medical Journal. Clinical study: Image-guided treatment outcomes for Baker’s cyst
Sansone V et al. Popliteal cysts and associated disorders of the knee: MRI review. International Orthopaedics. MRI-based review: Associated intra-articular knee pathology in Baker’s cyst
Frush TJ, Noyes FR. Baker’s Cyst: Diagnostic and Surgical Considerations. Sports Health. Clinical review: Diagnosis, differential diagnosis, and treatment strategies

















