

Lateral epicondylitis, commonly known as tennis elbow, is one of the most frequent causes of pain on the outer side of the elbow. Despite its name, the condition is not limited to tennis players and often affects people who perform repetitive gripping, lifting, or wrist extension activities at work, during sports, or in daily life.
A proper lateral epicondylitis test is an important part of diagnosing tennis elbow and identifying whether the symptoms are truly coming from the common extensor tendon origin at the lateral epicondyle. Doctors typically use a combination of specific physical examination tests, symptom evaluation, and functional assessment rather than relying on a single diagnostic maneuver.
There is no single test that can confirm tennis elbow with 100% accuracy. Because lateral epicondylitis is primarily a clinical diagnosis, the most reliable approach combines the patient’s history, location of pain, physical findings, and provocation tests that reproduce symptoms by stressing the affected tendon.
Commonly used clinical tests include Cozen’s test, Mill’s test, Maudsley’s test, resisted wrist extension testing, and grip strength assessment. These tests help clinicians evaluate the common extensor tendon complex and distinguish tennis elbow from other conditions that may cause similar symptoms, such as radial tunnel syndrome, cervical nerve irritation, or elbow joint disorders.
In this article, we will explain the most commonly used tennis elbow tests, how each test is performed, what a positive result means, and when ultrasound or MRI imaging may be necessary.
Key Takeaways – Lateral Epicondylitis Tests
- Lateral epicondylitis (tennis elbow) is usually diagnosed clinically through a combination of patient history, physical examination, and symptom reproduction during specific provocation tests.
- No single lateral epicondylitis test can confirm the diagnosis alone. The most reliable assessment combines multiple findings, including localized tenderness and positive provocation tests.
- Cozen’s test, Mill’s test, and Maudsley’s test are among the most commonly used clinical tests for reproducing pain related to the common extensor tendon.
- Grip strength testing provides useful functional information, as many patients experience reduced pain-free grip strength due to lateral elbow pain.
- Ultrasound and MRI are not routinely required for diagnosis but may help evaluate tendon changes or exclude other causes of lateral elbow pain in selected cases.
- Accurate diagnosis depends on recognizing a consistent clinical pattern and distinguishing tennis elbow from conditions such as radial tunnel syndrome, nerve disorders, and elbow joint pathology.
How Is Lateral Epicondylitis Diagnosed?
The diagnosis of lateral epicondylitis is usually made through a combination of medical history and physical examination. Unlike some musculoskeletal conditions, there is no single blood test, scan, or examination maneuver that can definitively confirm tennis elbow. Imaging, including ultrasound or MRI, is not usually necessary to diagnose tennis elbow, but it can provide additional information when the diagnosis is unclear or when other causes of elbow pain need to be excluded.
During the evaluation, the clinician focuses on the pattern of symptoms, the location of pain, activities that aggravate symptoms, and specific tests that place stress on the common extensor tendon.
Medical History
The first step in diagnosing tennis elbow is understanding how the symptoms developed. Doctors typically ask about:
- Location and character of pain – patients usually describe pain over the outer part of the elbow, directly around the lateral epicondyle. The pain may sometimes extend into the forearm.
- Activities that worsen symptoms – gripping, lifting objects, shaking hands, using tools, typing, or repetitive wrist movements commonly increase discomfort.
- Occupational activities – jobs involving repetitive hand and wrist movements, forceful gripping, or vibration exposure may increase the risk of developing lateral epicondylitis.
- Sports participation – although tennis elbow is not limited to tennis players, racquet sports, weight training, and other repetitive arm activities may contribute to tendon overload.
- Duration of symptoms – the timeline helps distinguish acute overload from chronic tendon degeneration.
Physical Examination
After taking the history, the clinician performs a physical examination to reproduce symptoms and assess the function of the elbow and forearm.
Typical examination findings include:
Tenderness Over the Lateral Epicondyle
The most characteristic finding is localized tenderness at the outer elbow, where the common extensor tendon attaches to the humerus.
Pressure over this area often reproduces the patient’s typical pain.
Pain With Resisted Wrist Extension
One of the most important findings is pain when the patient extends the wrist against resistance. This movement activates the wrist extensor muscles, particularly the extensor carpi radialis brevis (ECRB), which is frequently involved in tennis elbow.
Pain With Gripping Activities
Many patients report pain when squeezing objects, carrying bags, opening jars, or using tools. Grip testing can demonstrate both pain reproduction and reduced pain-free grip strength.
Provocation Tests
Several specific clinical tests have been developed to stress the affected tendon and reproduce symptoms, including:
- Cozen’s test
- Mill’s test
- Maudsley’s test
- Resisted wrist extension test
- Grip strength testing
Clinical Insight
No individual test should be interpreted in isolation. The diagnosis becomes more reliable when multiple findings are consistent with the patient’s symptoms and clinical presentation.
1. Cozen’s Test
Cozen’s test is one of the most commonly used lateral epicondylitis tests for evaluating tennis elbow. It is designed to reproduce pain by placing stress on the common extensor tendon origin, particularly the extensor carpi radialis brevis (ECRB) tendon, which is frequently involved in lateral epicondylitis.
The test evaluates whether resisted wrist extension triggers the patient’s typical pain over the lateral epicondyle.
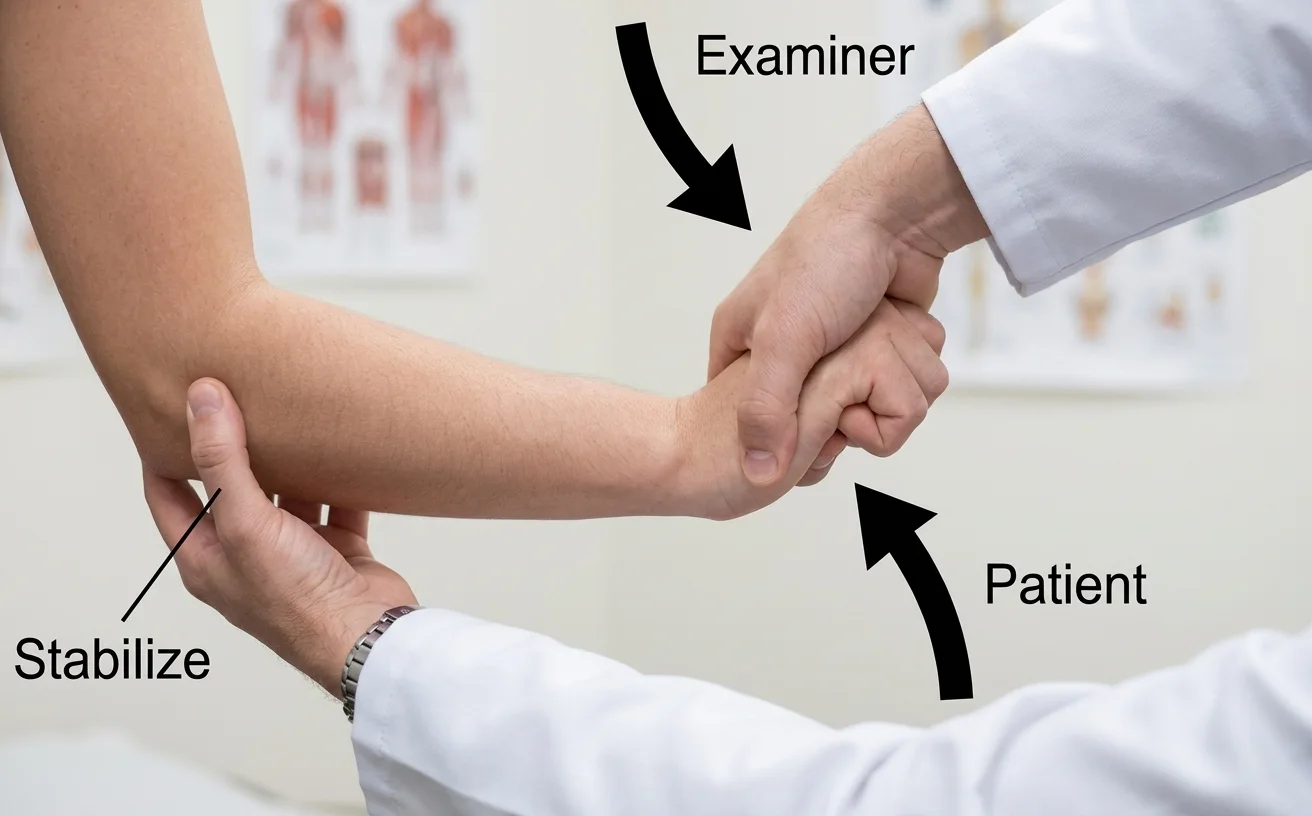
How to Perform Cozen’s Test
During Cozen’s test, the patient is usually seated with the elbow flexed at approximately 90 degrees and the forearm pronated.
The examiner stabilizes the patient’s elbow while asking the patient to:
- make a fist,
- extend the wrist upward,
- radially deviate the wrist (move it toward the thumb side),
- resist downward pressure applied by the examiner.
This movement activates the wrist extensor muscles and places tension on the common extensor tendon attachment at the lateral epicondyle.
Positive Cozen’s Test
A Cozen’s test is considered positive when the maneuver reproduces the patient’s familiar pain over the lateral epicondyle or the outer aspect of the elbow.
Pain may also extend slightly into the proximal forearm along the extensor muscle group.
A positive test does not confirm tennis elbow by itself, but it supports the diagnosis when combined with:
- localized tenderness over the lateral epicondyle,
- a typical history of overuse-related pain,
- symptoms aggravated by gripping or wrist movements.
2. Mill’s Test
Mill’s test is a commonly used tennis elbow test that evaluates pain caused by stretching the common extensor tendon at its attachment on the lateral epicondyle.
Unlike Cozen’s test, which stresses the tendon through active muscle contraction, Mill’s test places the extensor tendon under passive stretch. This helps identify tendon-related pain that is characteristic of lateral epicondylitis.
How to Perform Mill’s Test
During Mill’s test, the patient is seated or standing while the examiner performs the maneuver:
- the patient’s elbow is fully extended,
- the forearm is pronated (palm facing downward),
- the wrist is flexed,
- the forearm is slightly rotated inward.
The examiner gradually increases the stretch by combining elbow extension, forearm pronation, and wrist flexion.
This position lengthens the wrist extensor muscles and places tension on the common extensor tendon origin at the lateral epicondyle.

Positive Mill’s Test
The test is considered positive when it reproduces the patient’s typical pain over the lateral epicondyle or the outer aspect of the elbow.
Patients may describe:
- sharp pain at the tendon attachment,
- pulling discomfort along the extensor muscles of the forearm,
- pain similar to symptoms experienced during daily activities.
3. Maudsley’s Test (Middle Finger Extension Test)
Maudsley’s test is a commonly used tennis elbow test that evaluates pain produced by resisted extension of the middle finger. The test places stress on the wrist and finger extensor muscles, particularly the extensor digitorum and structures associated with the common extensor tendon origin.
Because the extensor muscles attach near the lateral epicondyle, resisted middle finger extension may reproduce pain in patients with lateral epicondylitis. However, this test can also be positive in some patients with radial tunnel syndrome, so the findings should always be interpreted together with the overall clinical picture.
How to Perform Maudsley’s Test
During Maudsley’s test, the patient is seated with the elbow extended or slightly flexed and the forearm pronated.
The examiner asks the patient to:
- extend the middle finger against resistance,
- maintain the extension while the examiner applies downward pressure to the finger.
This movement activates the finger extensor muscles and increases tension through the extensor tendon complex at the lateral elbow.

Positive Maudsley’s Test
The test is considered positive when resisted middle finger extension reproduces the patient’s typical pain over the lateral epicondyle or the outer aspect of the elbow.
Patients may experience:
- sharp pain at the lateral epicondyle,
- discomfort extending into the proximal forearm,
- pain similar to symptoms triggered by gripping or lifting activities.
4. Resisted Wrist Extension Test
The resisted wrist extension test is a simple and commonly performed examination maneuver used to assess pain related to the common extensor tendon in patients with suspected lateral epicondylitis.
Unlike more specific provocation tests such as Cozen’s test, this test focuses on the patient’s ability to extend the wrist against resistance and whether this contraction reproduces pain at the lateral elbow.
Wrist extension activates the forearm extensor muscles, including the extensor carpi radialis brevis (ECRB), which is frequently involved in tennis elbow.
How to Perform the Resisted Wrist Extension Test
During the test, the patient is seated with the forearm supported and the palm facing downward.
The examiner asks the patient to:
- extend the wrist upward,
- maintain the position while the examiner applies downward resistance.
The patient attempts to lift the hand against resistance while the examiner evaluates for pain and strength.
This maneuver increases tension through the wrist extensor muscles and loads their attachment at the lateral epicondyle.
Positive Resisted Wrist Extension Test
The test is considered positive when resisted wrist extension reproduces the patient’s familiar pain over the lateral epicondyle or the outer aspect of the elbow.
Patients may report:
- localized pain at the tendon attachment,
- discomfort spreading into the extensor muscles of the forearm,
- pain during activities involving lifting, gripping, or repetitive wrist movements.
Difference between Cozen’s test and resisted wrist extension test
Although both the resisted wrist extension test and Cozen’s test evaluate pain during wrist extension, they are not exactly the same maneuver.
The resisted wrist extension test is a more general assessment of wrist extensor function, focusing mainly on whether contraction of the extensor muscles reproduces lateral elbow pain.
In contrast, Cozen’s test uses a more specific position that combines wrist extension, radial deviation, and resisted movement with the forearm pronated. This places additional stress on the common extensor tendon origin and is designed specifically as a provocation test for lateral epicondylitis.
5. Resisted Forearm Supination Test
The resisted forearm supination test is a clinical maneuver that evaluates pain produced during resisted supination of the forearm. Although it is not one of the primary diagnostic tests for lateral epicondylitis, it can provide additional information when assessing patients with lateral elbow pain.
Forearm supination activates the supinator muscle and the biceps brachii, while also increasing tension within the lateral elbow structures. Because several muscles and tendons contribute to lateral elbow function, pain during this movement may occur in different conditions affecting the area.
How to Perform the Resisted Forearm Supination Test
During the test, the patient is seated with the elbow flexed and the forearm in a neutral position.
The examiner asks the patient to:
- rotate the forearm outward into a palm-up position (supination),
- resist the examiner’s attempt to push the forearm back toward pronation.
The examiner evaluates whether this resisted movement reproduces pain around the lateral elbow.
Positive Resisted Forearm Supination Test
The test is considered positive when resisted supination reproduces the patient’s familiar pain over the lateral aspect of the elbow.
Patients may report:
- pain near the lateral epicondyle,
- discomfort deeper in the proximal forearm,
- symptoms that increase with gripping or rotational movements.
Pain during resisted supination is not specific for lateral epicondylitis and should be interpreted alongside other examination findings. It may also be present in conditions affecting the radial tunnel, supinator muscle, or other structures around the lateral elbow.
6. Grip Strength Test
The grip strength test is a functional assessment commonly used during the evaluation of patients with suspected lateral epicondylitis. Although it does not directly stress the common extensor tendon in the same way as provocation tests, it provides important information about how elbow pain affects hand function.
Grip strength is often reduced in patients with tennis elbow, not necessarily because of true muscle weakness, but because pain during gripping limits the amount of force the patient can comfortably generate.
How to Perform the Grip Strength Test
Grip strength is usually measured using a hand dynamometer, which allows objective assessment of squeezing force.
During the test:
- the patient holds the dynamometer in the hand,
- the elbow is positioned according to the testing protocol,
- the patient squeezes as firmly as possible,
- the examiner records the generated grip force.
The test is often repeated on both sides to compare the affected and unaffected arms.
Positive Grip Strength Test
The test is considered clinically relevant when gripping reproduces the patient’s typical pain over the lateral epicondyle or when there is a noticeable reduction in pain-free grip strength compared with the opposite side.
Patients may experience:
- pain while squeezing the device,
- reduced ability to generate force because of discomfort,
- difficulty with everyday activities such as opening jars, carrying objects, or using tools.
A reduction in pain-free grip strength can be a useful functional indicator in patients with lateral epicondylitis and may help monitor symptom severity over time.
Which Test Is the Most Accurate?
There is no single lateral epicondylitis test that can confirm tennis elbow with complete accuracy. The diagnosis is based on the combination of the patient’s symptoms, physical examination findings, and reproduction of pain during specific provocation tests.
The most useful clinical findings include:
- Tenderness over the lateral epicondyle – one of the most consistent examination findings in patients with tennis elbow.
- Positive Cozen’s test – pain reproduction during resisted wrist extension supports involvement of the common extensor tendon.
- Positive Mill’s test – pain during passive stretching of the extensor tendon complex supports tendon-related lateral elbow pain.
- Positive Maudsley’s test – pain during resisted middle finger extension may support the diagnosis, although it should be interpreted together with other findings.
Additional information from pain-free grip strength testing and the patient’s symptom pattern during daily activities can help assess functional impact.
The most accurate approach is not identifying one “best” test, but recognizing a consistent clinical pattern combining history, tenderness, and multiple positive provocation tests.
Imaging is not routinely required for the diagnosis of lateral epicondylitis, but ultrasound and MRI may be useful in selected cases when the diagnosis is uncertain, to evaluate tendon changes, or to exclude other causes of lateral elbow pain.
Do You Need MRI or Ultrasound?
Imaging is not routinely required to diagnose lateral epicondylitis because the condition is usually identified through a combination of medical history and physical examination findings. However, ultrasound and MRI can provide additional information when the diagnosis is unclear, symptoms are persistent, or another condition needs to be excluded.
Imaging is particularly useful for evaluating the condition of the common extensor tendon, identifying structural changes, and assessing alternative causes of lateral elbow pain.
Ultrasound for Tennis Elbow
Musculoskeletal ultrasound is a valuable imaging method for evaluating the tendons involved in lateral epicondylitis. It allows dynamic assessment of the elbow and can identify changes associated with tendon degeneration.
Typical ultrasound findings include:
- Tendon thickening – enlargement of the common extensor tendon due to degenerative changes.
- Hypoechoic areas – regions of reduced echogenicity that may represent tendon disorganization and tissue degeneration.
- Loss of the normal fibrillar tendon pattern – disruption of the typical ultrasound appearance of healthy tendon fibers.
- Neovascularization on Doppler imaging – increased blood flow within the tendon, which is commonly seen in chronic tendinopathy.
- Calcifications – calcium deposits within or around the tendon that may contribute to symptoms.
One of the main advantages of ultrasound is that it allows dynamic examination, comparison with the opposite elbow, and can be used to guide procedures such as ultrasound-guided injections when indicated.
MRI for Tennis Elbow
MRI is not usually necessary for routine diagnosis but can be helpful in selected patients, especially when symptoms are severe, prolonged, or the diagnosis is uncertain.
MRI findings associated with lateral epicondylitis may include:
- increased signal intensity within the common extensor tendon,
- tendon thickening,
- partial tendon tears,
- degenerative changes at the tendon origin.
MRI can also help identify other causes of lateral elbow pain, such as:
- ligament injuries,
- osteochondral lesions,
- joint pathology,
- nerve-related conditions.
X-ray in Tennis Elbow
X-rays do not show tendon degeneration directly and are not used to diagnose lateral epicondylitis. However, they may be useful when the clinician needs to exclude other conditions, such as:
- elbow osteoarthritis,
- fractures,
- calcifications near the tendon attachment,
- other bone abnormalities.
Conditions That Mimic Tennis Elbow
Although lateral epicondylitis is the most common cause of pain on the outer side of the elbow, several other conditions can produce similar symptoms. This is why the results of tennis elbow tests should always be interpreted together with the patient’s history and complete clinical examination.
Common conditions that may mimic tennis elbow include:
Radial Tunnel Syndrome
Radial tunnel syndrome can cause pain in the lateral elbow and proximal forearm, but the tenderness is often located farther down the forearm rather than directly over the lateral epicondyle. Symptoms may worsen with forearm rotation and resisted supination.
Posterior Interosseous Nerve (PIN) Syndrome
PIN syndrome may resemble tennis elbow but is more commonly associated with weakness of finger and thumb extension due to nerve dysfunction.
Cervical Radiculopathy
Nerve irritation from the neck can cause pain around the elbow and forearm. Associated symptoms such as neck pain, numbness, tingling, or changes in strength may suggest a cervical origin.
Elbow Joint Disorders
Conditions such as osteoarthritis, ligament injuries, or other joint problems may also cause lateral elbow pain, particularly when symptoms include stiffness, instability, or reduced range of motion.
A thorough clinical assessment helps distinguish lateral epicondylitis from these conditions and ensures that treatment is directed at the correct source of pain.
When Should You See a Doctor?
Most cases of tennis elbow improve with activity modification and appropriate rehabilitation. However, medical evaluation is recommended if:
- symptoms persist for several weeks despite rest and self-care,
- elbow pain is getting worse over time,
- there is significant weakness in the hand or grip,
- numbness or tingling develops,
- symptoms started after an injury or trauma,
- elbow movement becomes limited,
- the symptoms do not match typical tennis elbow or another condition is suspected.
A proper clinical assessment can help confirm the diagnosis and ensure that other causes of lateral elbow pain are not overlooked.
FAQ
What is the best test for lateral epicondylitis?
There is no single best test that confirms lateral epicondylitis. The diagnosis is based on a combination of findings, including tenderness over the lateral epicondyle, patient history, and positive provocation tests such as Cozen’s test, Mill’s test, and Maudsley’s test.
Is Cozen’s test accurate for tennis elbow?
Cozen’s test is one of the most commonly used clinical tests for tennis elbow because it reproduces pain by loading the common extensor tendon. However, it should not be interpreted alone, as the diagnosis depends on the overall clinical assessment.
Is Mill’s test painful?
Mill’s test may reproduce pain because it stretches the common extensor tendon attached to the lateral epicondyle. In patients with tennis elbow, this stretch often causes their typical outer elbow pain.
Can I test myself for tennis elbow?
Some simple maneuvers, such as resisted wrist extension or gripping activities, may reproduce symptoms associated with tennis elbow. However, self-testing cannot reliably confirm the diagnosis or exclude other causes of elbow pain.
What is the difference between Cozen’s and Mill’s test?
Cozen’s test evaluates pain during active wrist extension against resistance, placing load on the common extensor tendon. Mill’s test evaluates pain produced by passive stretching of the same tendon structures.
Does MRI confirm tennis elbow?
MRI can show tendon changes associated with lateral epicondylitis, such as tendon thickening or degeneration, but it is not required for routine diagnosis. Tennis elbow is primarily a clinical diagnosis based on symptoms and examination findings.
Is ultrasound better than MRI for tennis elbow?
Ultrasound and MRI both have a role in evaluating tennis elbow. Ultrasound offers dynamic assessment, allows comparison with the opposite side, and can detect tendon abnormalities, while MRI may provide more detailed evaluation of deeper structures and other possible causes of pain.
Can tennis elbow be diagnosed without imaging?
Yes. Most cases of tennis elbow can be diagnosed without ultrasound or MRI. Imaging is usually reserved for unclear cases, persistent symptoms, suspected tendon tears, or when another diagnosis needs to be excluded.
Which muscles are tested in lateral epicondylitis?
Lateral epicondylitis tests mainly evaluate the wrist and finger extensor muscles attached to the common extensor tendon, particularly the extensor carpi radialis brevis (ECRB).
How long does a tennis elbow examination take?
A typical clinical examination for tennis elbow usually takes only a few minutes. It includes a review of symptoms, physical examination, palpation of the elbow, movement testing, and specific provocation tests.
Bisset L et al. A systematic review of clinical tests for lateral epicondylalgia. British Journal of Sports Medicine. PubMed: Clinical diagnosis and examination of lateral epicondylalgia
Coombes BK et al. Efficacy and safety of corticosteroid injections and other treatments for lateral epicondylitis. The Lancet. PubMed: Evidence review of tennis elbow treatment strategies
Ma KL et al. Diagnostic accuracy of clinical tests for lateral epicondylitis: a systematic review. PubMed: Diagnostic evaluation of clinical provocative tests for tennis elbow
















