

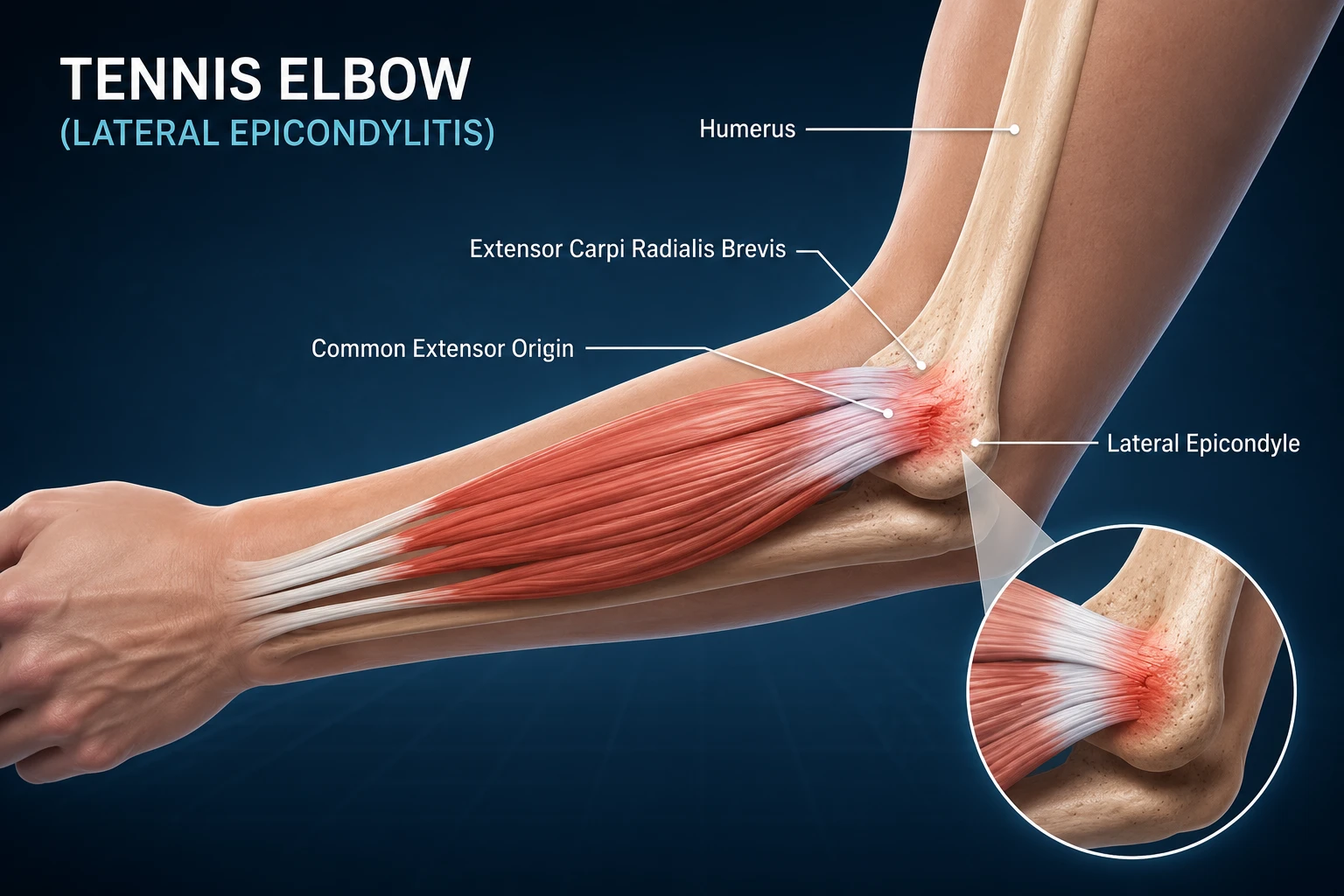
Tennis elbow or lateral epicondylitis, is the most common cause of pain on the outer side of the elbow. It develops when the wrist‑extensor tendons become overloaded from repetitive gripping and lifting. Although linked to racquet sports, it appears even more often in people whose work requires continuous manual tasks. The key symptom is lateral elbow pain that increases during activity.
Tennis elbow can limit daily function and lead to time away from work, especially in manual labor occupations. Early management focuses on reducing activities that provoke pain. Most patients respond well to conservative treatment, including analgesics, physiotherapy, and targeted injections. Surgery is rarely needed and reserved for long‑lasting, resistant cases.
Symptoms may persist for months, but proper treatment significantly shortens recovery. This article explains what tennis elbow is, why it develops, how to recognize symptoms, and which treatment options offer the best outcomes for this common condition.
Key Clinical Points – Tennis Elbow (Lateral Epicondylitis)
- Tennis elbow (lateral epicondylitis) is the most common cause of pain on the outer side of the elbow and affects the common extensor tendon at the lateral epicondyle.
- The condition develops due to repetitive tendon overload from gripping, lifting, and wrist-extension activities, with most cases occurring in manual workers rather than tennis players.
- The main symptoms include lateral elbow pain, reduced grip strength, and pain during activities such as lifting objects, shaking hands, or using tools.
- Diagnosis is usually clinical, based on history and physical examination. Imaging is not routinely required but ultrasound can confirm tendon changes when needed.
- Conservative treatment is effective for most patients and includes activity modification, pain management, exercises, and progressive tendon rehabilitation.
- Recovery is often gradual, with symptoms commonly improving over 6–12 months. Surgery is rarely required and is reserved for persistent cases that do not respond to appropriate non-surgical treatment.
What Is Tennis Elbow (Lateral Epicondylitis)?
Tennis elbow is an overuse injury affecting the common extensor tendon on the outer side of the elbow. This tendon originates at the lateral epicondyle, a bony prominence that serves as the attachment point for muscles responsible for wrist extension and grip.
When these muscles are repeatedly overloaded, the tendon fibers become irritated and weakened, leading to pain and reduced function. In medical terminology, this condition is known as lateral epicondylitis, but the term tennis elbow remains more widely used in everyday practice.
The core problem in tennis elbow is a combination of tendon overload and gradual degenerative changes. Repetitive gripping, lifting, or wrist‑extension movements increase strain on the common extensor tendon, especially the ECRB portion, which is most vulnerable to micro‑tearing. Over time, this leads to localized pain on the lateral epicondyle, reduced grip strength, and difficulty performing everyday tasks.
Although athletes can develop symptoms, most cases occur in people whose work or hobbies involve frequent manual activity.
In the next section, we explain how tendon overload develops over time and why both “tendinitis” and chronic tendon degeneration play a key role in the progression of tennis elbow.
Tendon Overload: Acute vs. Chronic Changes
Short‑term overload of the common extensor tendon can trigger a rapid, reactive response in the tissue. This often appears after a full day of painting, moving heavy furniture, hammering, or an intense tennis match. The tendon becomes thicker and sensitive, a process commonly described as “tendon inflammation – tendinitis,” although true inflammatory cells are usually absent. This phase is known as reactive tendinopathy, and it typically resolves within days or weeks if the tendon is allowed to rest. Importantly, it does not leave lasting structural damage.
When overload continues for weeks or months, the tendon loses its ability to recover between bouts of mechanical stress. This leads to degenerative tendinopathy, the hallmark of chronic lateral epicondylitis.
Microscopic tendon fibers begin to break down, collagen becomes disorganized, and areas of cell death appear. Instead of healthy tendon tissue, the body forms patches of degraded matrix and small blood vessels. These changes reduce the tendon’s healing capacity and create a mixture of healthy and damaged tissue. In this stage, pain may persist even with rest.
However, chronic tendon degeneration does not always produce pain — structural changes in the tendon can exist even in completely asymptomatic individuals.
Causes & Risk Factors: What Causes Tennis Elbow?
Tennis elbow, or lateral epicondylitis, develops when the common extensor tendon at the lateral epicondyle is exposed to forces it cannot adequately tolerate. These forces may come from repetitive movements, sudden increases in load, poor conditioning, or occupational demands. Although the condition is strongly associated with racquet sports, most cases arise from everyday manual tasks rather than athletic activity.
Overuse of the Wrist Extensors in Sport
The most common cause of tennis elbow is repetitive use of the wrist‑extensor muscles. Movements such as gripping, lifting, twisting, and wrist extension place continuous stress on the common extensor tendon, especially the ECRB portion. Sports like tennis, badminton, and squash increase this load, particularly during the backhand stroke, where the elbow extends and the wrist lifts sharply. These repeated motions gradually exceed the tendon’s capacity, leading to irritation, micro‑tearing, and pain.
Occupational Load and Manual Work
Tennis elbow is frequently seen in people who perform demanding manual tasks. Construction workers, carpenters, painters, plumbers, masons, factory workers, warehouse staff, and meat processors often rely heavily on repetitive gripping and wrist‑extension movements. These activities create sustained mechanical stress on the lateral epicondyle attachment, making work‑related overload one of the strongest risk factors. In many cases, occupational exposure explains what causes tennis elbow more accurately than sports participation.
Low Conditioning and Insufficient Tendon Capacity
Tennis elbow also occurs in people who are not physically active. In these cases, the tendon lacks the conditioning needed to tolerate even normal daily loads. Individuals who spend most of the day at a computer may develop pain at the lateral epicondyle despite minimal physical activity. The underlying issue is insufficient tendon capacity, not excessive force. This explains why tennis elbow is common among office workers, administrators, and healthcare professionals, including nurses.
Who Is Most at Risk?
Lateral epicondylitis appears equally in men and women, more often on the dominant arm, and is especially common among workers who perform repetitive wrist and forearm movements.
- Middle‑aged adults (30–50 years)
- People performing repetitive hand tasks
- Recreational racquet‑sport players
- Individuals with low physical conditioning
- Workers using tools requiring strong grip
Clinical Insight
Only about 5% of all patients with tennis elbow actually play tennis, while the condition affects 1–3% of the general population.
Tennis Elbow Symptoms
The hallmark tennis elbow symptoms include pain on the outer (lateral) side of the elbow that may radiate down the forearm or, less commonly, up toward the upper arm. The pain is typically triggered by activity and improves with rest, although some people experience persistent pain even when not using the arm. In more severe cases, the discomfort may also occur at night.
Most people with tennis elbow do not recall a specific injury. Instead, symptoms usually develop gradually following repetitive use of the forearm muscles and tendons. Elbow pain often appears 1–3 days after activities involving repeated gripping, wrist extension, or forearm rotation.In athletes, symptoms may begin after increasing training intensity, changing equipment (such as a new tennis racquet), or practicing for longer than usual.
Tennis elbow can also develop after a single episode of excessive strain, such as lifting a heavy object or hitting a powerful backhand shot.
Pain severity varies widely. Some individuals experience only mild discomfort during strenuous activities, while others find even simple daily tasks difficult. Actions such as lifting a coffee mug, shaking hands, opening a jar, turning a doorknob, or carrying a shopping bag may become painful. Many patients also report a noticeable reduction in grip strength on the affected side.
Common activities that worsen tennis elbow symptoms include:
- Gripping objects firmly.
- Lifting items with the palm facing downward.
- Turning a screwdriver or using hand tools.
- Wringing out a wet towel or cloth.
- Carrying grocery bags or suitcases.
- Playing tennis, particularly the backhand stroke.
- Repetitive computer mouse use or prolonged keyboard work.
- Manual work involving repetitive wrist and forearm movements.
Symptoms often progress gradually over weeks or months if the affected tendon is repeatedly overloaded without adequate recovery.
How Is Lateral Epicondylitis Diagnosed?
In most cases, diagnosing lateral epicondylitis (tennis elbow) does not require complex investigations. An experienced clinician can usually make the diagnosis based on a detailed medical history and a focused physical examination. Imaging tests are often unnecessary unless the diagnosis is uncertain or another condition is suspected.
There are no visible external signs of tennis elbow. Swelling and bruising are uncommon, and the elbow usually appears normal. Instead, the diagnosis relies on identifying characteristic pain patterns and reproducing symptoms during specific clinical examination maneuvers.
Physical Examination and Tennis Elbow Tests
The hallmark finding on physical examination is localized tenderness over the lateral epicondyle, where the common extensor tendon originates from the humerus. Several tennis elbow tests can reliably reproduce the patient’s symptoms by loading the extensor tendons and help confirm the diagnosis of lateral epicondylitis.
- Cozen’s Test – The patient makes a fist, pronates the forearm, extends the wrist, and slightly radially deviates the wrist against resistance. Reproduction of sharp pain over the lateral epicondyle is considered a positive test and strongly suggests lateral epicondylitis.
- Maudsley’s Test (Middle Finger Extension Test) – The patient extends the middle finger against resistance while the elbow is extended. This maneuver preferentially loads the extensor digitorum communis and the extensor carpi radialis brevis (ECRB). Pain over the lateral epicondyle is considered a positive finding.
- Mill’s Test – With the elbow extended, the examiner passively pronates the forearm, flexes the wrist, and flexes the fingers, stretching the common extensor tendon. Reproduction of lateral elbow pain indicates a positive test.
- Resisted Wrist Extension Test – Active wrist extension against resistance with the elbow extended typically reproduces pain at the lateral epicondyle and is one of the most commonly performed clinical tests.
- Resisted Forearm Supination Test – The patient attempts to supinate the forearm against resistance. This maneuver increases load across the extensor–supinator muscle complex and may reproduce the characteristic pain of tennis elbow.
Imaging
Imaging is not routinely required for diagnosing lateral epicondylitis (tennis elbow), as the diagnosis is usually based on the patient’s symptoms and physical examination. However, imaging may be useful when symptoms persist, when the diagnosis is uncertain, or when other causes of elbow pain need to be excluded.
Ultrasound
Musculoskeletal ultrasound is the preferred imaging method for evaluating tennis elbow. It can show typical tendon changes associated with chronic tendinopathy, including:
- thickening of the common extensor tendon
- irregular or heterogeneous tendon structure
- hypoechoic areas related to tendon degeneration and microtears
- small calcifications
- changes at the tendon attachment site
- increased blood flow (neovascularization) on Doppler examination
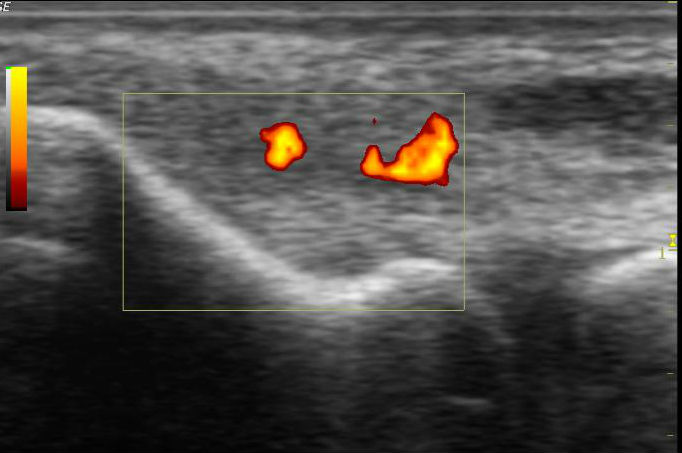
Ultrasound is also useful because it allows dynamic assessment of the tendon and can guide injections or other minimally invasive treatments when needed.
MRI
MRI provides a detailed view of tendon degeneration and possible partial tears but is rarely needed in typical cases. It is usually reserved for persistent symptoms, unclear diagnoses, suspected significant tendon damage, or when surgical treatment is being considered.
X-ray
X-rays cannot visualize tendons or tendon degeneration, so they do not confirm tennis elbow. However, they may help rule out other causes of lateral elbow pain, such as fractures, arthritis, or bone abnormalities.
Tennis Elbow Treatment
Treatment of tennis elbow (lateral epicondylitis) is usually based on conservative, non-surgical methods. The majority of patients improve with appropriate activity modification, pain management, and a structured rehabilitation program.
Surgery is rarely required and is generally considered only in patients with persistent symptoms despite several months of well-conducted conservative treatment.
The main goals of treatment are to:
- reduce pain
- restore normal elbow function
- improve tendon capacity and strength
- prevent recurrence
Conservative Treatment for Tennis Elbow
The first step in treating tennis elbow is reducing or modifying activities that aggravate symptoms. Complete immobilization is usually not necessary; instead, patients should avoid painful movements while gradually returning to normal activities.
For symptoms caused by short-term overload, a period of relative rest lasting 1–3 weeks may be sufficient.
People who play tennis should also evaluate factors that may contribute to tendon overload, including:
- incorrect backhand technique
- unsuitable racket grip size
- excessive string tension
- inappropriate equipment
Improving sports technique and adjusting equipment may help reduce stress on the extensor tendons.
Pain Relief Medication
Pain-relieving medications may be used during the early stages of tennis elbow treatment. Common options include:
- non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, naproxen, or diclofenac
- paracetamol for pain control
These medications should generally be used for the shortest possible period and are not recommended as a long-term solution, as they do not address the underlying tendon problem.
Tennis Elbow Brace and Tennis Elbow Strap
A tennis elbow brace or tennis elbow strap can help reduce pain by decreasing the load transmitted through the affected extensor tendons.
The strap is usually placed around the forearm, approximately 5–7 cm below the elbow joint, rather than directly over the painful tendon attachment.
Braces may be particularly useful during activities that provoke symptoms, such as:
- lifting objects
- repetitive wrist movements
- sports activities
However, braces should be considered a supportive measure and are usually combined with exercises and rehabilitation rather than used as the only treatment.
Lateral Epicondylitis Exercises and Physical Therapy
Exercise-based rehabilitation is one of the most important components of long-term recovery from tennis elbow.
A structured program usually includes:
- stretching exercises for the wrist extensor muscles
- strengthening exercises for the forearm muscles
- progressive loading of the tendon
- eccentric exercises designed to improve tendon capacity
Physical therapy may also include additional treatments such as manual therapy, extracorporeal shockwave therapy, or other modalities depending on the individual patient.
The focus of modern rehabilitation is not only reducing pain but also gradually restoring the tendon’s ability to tolerate load.
Injection Treatments
When symptoms persist despite appropriate conservative treatment, injection therapies may be considered.
Corticosteroid Injections
Corticosteroid injections can provide short-term pain relief in some patients. However, their effect may not be long-lasting, and repeated injections should be avoided because they may negatively affect tendon quality and increase the risk of tendon weakening.
Platelet-Rich Plasma (PRP)
PRP therapy involves injecting a concentrated preparation of the patient’s own platelets into the area of tendon degeneration.
PRP contains growth factors that may support tissue healing and tendon remodeling. Current evidence suggests that PRP may provide benefits in some patients with chronic tennis elbow, although research is still ongoing.
Surgical Treatment
Most patients with tennis elbow recover without surgery. Operative treatment is reserved for a small group of patients with:
- persistent pain despite prolonged conservative treatment
- significant functional limitations
- confirmed structural tendon damage
Surgery aims to remove degenerated tendon tissue and stimulate healing of the tendon attachment.
How to Treat Tennis Elbow at Home
Most cases of tennis elbow can be successfully managed at home with a combination of activity modification, pain control, and gradual strengthening exercises. The goal is not complete rest, but reducing irritation of the tendon while gradually improving its ability to tolerate load.
1. Modify Activities That Trigger Pain
The first step in home treatment is avoiding or reducing activities that repeatedly overload the wrist extensor tendons.
Try to temporarily limit:
- repetitive gripping and lifting
- heavy household tasks
- activities that require forceful wrist extension
- movements that consistently reproduce pain
Complete immobilization is usually not recommended, as gradual movement and progressive loading are important for tendon recovery.
2. Apply Ice for Short-Term Pain Relief
Ice may help reduce pain, especially after activities that aggravate symptoms.
Apply an ice pack wrapped in a towel to the painful area for 10–15 minutes, particularly after activities that increase discomfort.
3. Use a Tennis Elbow Strap
A tennis elbow strap may reduce stress on the painful tendon attachment during daily activities.
The strap should be positioned approximately 5–7 cm below the outside of the elbow, around the forearm muscles, rather than directly over the painful area.
A brace can be useful during activities that provoke symptoms, but it should not replace rehabilitation exercises.
4. Perform Lateral Epicondylitis Exercises
Specific lateral epicondylitis exercises are an important part of recovery. They help improve tendon strength, flexibility, and tolerance to load.
Common exercises include:
- gentle stretching of the wrist extensor muscles
- progressive strengthening exercises
- eccentric exercises for the forearm muscles
Exercises should be performed gradually and should not significantly increase pain during or after activity.
5. Pain Relief Medication When Needed
Short-term use of pain medication may help during periods of increased discomfort. Options may include paracetamol or non-steroidal anti-inflammatory drugs (NSAIDs), if appropriate for the individual patient.
Medication can reduce symptoms but does not correct the underlying tendon problem, so it should be combined with activity modification and rehabilitation.
When to Seek Medical Advice
Although tennis elbow often improves with home treatment, medical evaluation is recommended when:
- pain persists despite several weeks of appropriate self-care
- symptoms significantly limit daily activities
- there is weakness, numbness, or loss of elbow movement
- the diagnosis is uncertain
A structured rehabilitation program guided by a healthcare professional may be recommended for persistent symptoms.
Prognosis and What to Expect
Tennis elbow usually develops gradually over time. Tendon changes may be present for months or even years before a person notices pain or functional problems.
The course of recovery depends on several factors, including the duration of symptoms, the severity of tendon changes, daily activities, and adherence to rehabilitation. In many cases, symptoms improve with appropriate activity modification and a structured exercise program, but recovery is often slow and requires patience.
If pain develops after a short period of overuse, symptoms may improve within several weeks with relative rest, avoiding aggravating activities, and short-term pain management. However, in many patients, tennis elbow becomes a longer-lasting condition, with symptoms persisting for several months.
Most patients experience gradual improvement within 6–12 months, and conservative treatment is successful in the majority of cases. However, some people may continue to have symptoms for longer periods, especially when tendon overload continues or when rehabilitation is insufficient.
Even after symptoms improve, recurrence is possible, particularly if the tendon is exposed to the same repetitive stresses that contributed to the original problem. Gradual return to activities, strengthening exercises, and attention to technique and workload are important to reduce the risk of recurrence.
Although tennis elbow can be frustrating because of its slow recovery, the overall prognosis is generally good, and only a small proportion of patients require surgical treatment.
Frequently Asked Questions About Tennis Elbow
What is the difference between tennis elbow and golfer’s elbow?
Tennis elbow (lateral epicondylitis) affects the tendons on the outside of the elbow, where the wrist extensor muscles attach to the lateral epicondyle. Golfer’s elbow (medial epicondylitis) affects the tendons on the inside of the elbow, where the wrist flexor muscles attach to the medial epicondyle. Both conditions are caused by tendon overload, but they involve different tendon groups and cause pain in different areas of the elbow.
What happens if tennis elbow remains untreated?
If tennis elbow is left untreated, symptoms may persist and become more difficult to manage. Continued overload of the tendon can maintain pain, reduce grip strength, and interfere with daily activities. However, tennis elbow does not usually lead to permanent damage, and most people improve with appropriate activity modification and rehabilitation.
How long does tennis elbow take to heal?
Tennis elbow recovery can take several months because tendon healing and remodeling are slow processes. Many patients experience significant improvement within 6–12 months with appropriate treatment, although some people may have symptoms for a longer period.
Can tennis elbow heal on its own?
Yes. Tennis elbow can improve without surgery. Reducing activities that overload the tendon, combined with gradual strengthening exercises, allows the tendon to recover and adapt to increased loads. However, recovery is often slow, and structured rehabilitation can help improve outcomes.
What are the best exercises for tennis elbow?
The most effective lateral epicondylitis exercises include stretching of the wrist extensor muscles and progressive strengthening exercises, especially eccentric exercises. These exercises help improve tendon strength, increase load tolerance, and reduce the risk of recurrence.
Does a tennis elbow brace or strap help?
A tennis elbow brace or tennis elbow strap can temporarily reduce pain by decreasing stress on the affected tendon during activities. However, braces should be considered a supportive treatment and are most effective when combined with rehabilitation exercises rather than used as the only treatment.
Can tennis elbow come back after treatment?
Yes. Recurrence is possible, especially if the tendon is exposed again to repetitive overload without adequate strengthening or gradual return to activities. Maintaining tendon strength, improving technique, and modifying activities that trigger symptoms can help reduce the risk of recurrence.
When should I see a doctor for tennis elbow?
You should seek medical advice if pain persists despite several weeks of self-care, significantly limits daily activities, or is associated with weakness, numbness, swelling, or reduced elbow movement.
Is tennis elbow caused by inflammation?
Despite its name, tennis elbow is not usually a classic inflammatory condition. It is better understood as a tendinopathy, involving tendon degeneration, changes in collagen structure, and impaired tendon healing. This is why modern treatment focuses on progressive tendon loading and rehabilitation rather than only reducing inflammation.
Buchanan BK, Varacallo MA. Lateral Epicondylitis (Tennis Elbow). StatPearls Publishing. StatPearls: Evidence-based overview of tennis elbow diagnosis and management
Ma KL, Wang HQ. Management of Lateral Epicondylitis: A Narrative Literature Review. Pain Research and Management. Narrative review: Current concepts in lateral epicondylitis treatment
Lapner P, Alfonso A, Hebert-Davies J, et al. Nonoperative treatment of lateral epicondylitis: A systematic review and meta-analysis. JSES International. Systematic review: Effectiveness of conservative treatment for tennis elbow
Kim JH, Hoy JF, Smith SR, et al. Recalcitrant Lateral Epicondylitis: A Systematic Review on Current Nonoperative and Operative Treatment Modalities. JBJS Reviews. Systematic review: Current treatment options for refractory tennis elbow
Bateman M, Littlewood C, Rawson B, Tambe AA. Surgery for Tennis Elbow: A Systematic Review. Shoulder & Elbow. Systematic review: Surgical treatment outcomes for tennis elbow
Kim YJ, Wood SM, Yoon AP, et al. Efficacy of Nonoperative Treatments for Lateral Epicondylitis: A Systematic Review and Meta-analysis. Plastic and Reconstructive Surgery. Meta-analysis: Evidence for nonoperative tennis elbow treatments
Keijsers R, de Vos RJ, Kuijer PPF, et al. Tennis Elbow. Shoulder & Elbow. Clinical review: Tennis elbow diagnosis, imaging, and treatment
Karabinov V, Georgiev GP. Lateral Epicondylitis: New Trends and Challenges in Treatment. World Journal of Orthopedics. Review article: Emerging treatment strategies for lateral epicondylitis
Cutts S, Gangoo S, Modi N, Pasapula C. Tennis Elbow: A Clinical Review Article. Journal of Orthopaedics. Clinical review: Tennis elbow pathophysiology, diagnosis, and treatment
Binder AI, Hazleman BL. Lateral Humeral Epicondylitis: A Study of Natural History and the Effect of Conservative Therapy. British Journal of Rheumatology. Classic study: Natural history and prognosis of tennis elbow
InformedHealth.org (IQWiG). Overview: Tennis Elbow. NCBI Bookshelf. Patient guide: Tennis elbow symptoms, treatment, and recovery
















