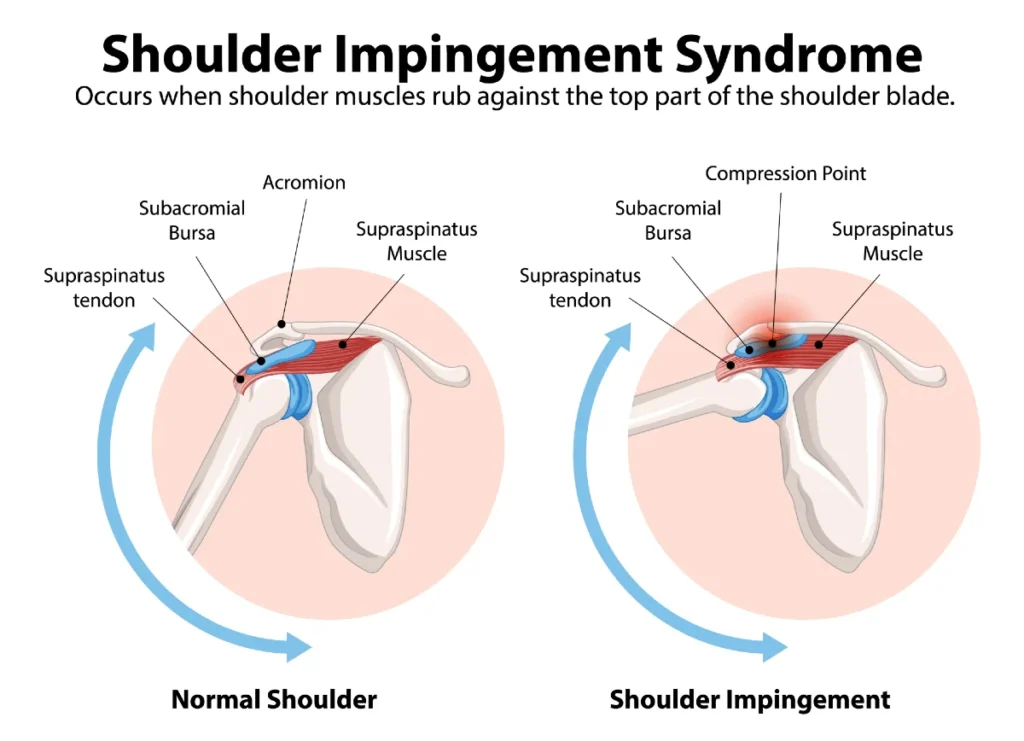
Shoulder impingement syndrome, also known as subacromial impingement, is one of the most common causes of shoulder pain, reduced strength, and limited range of motion in the shoulder joint.
This condition develops when soft tissues such as the rotator cuff tendons or the subacromial bursa become compressed between the structures of the shoulder during arm movement. This repeated mechanical irritation can lead to inflammation, pain, and progressive tendon degeneration within the subacromial space.
In this article, we explain what is shoulder impingement syndrome, how it develops, how to recognize its symptoms, and which treatment options are available. We also discuss practical strategies for pain relief, rehabilitation, and long-term prevention, helping you maintain shoulder health and safely return to your daily activities.
Key Clinical Points – Shoulder Impingement Syndrome
- Shoulder impingement syndrome (also known as subacromial impingement) is a common cause of shoulder pain due to mechanical irritation of rotator cuff tendons within the subacromial space.
- The condition is frequently associated with overhead activities, age-related tendon degeneration, and impaired scapular or rotator cuff muscle control.
- Patients typically present with pain during arm elevation, especially between 60° and 120° of abduction, often accompanied by a painful arc and night pain.
- Diagnosis is primarily clinical, based on history and examination, with tests such as Hawkins-Kennedy and Neer test supporting the diagnosis but lacking full specificity.
- Physiotherapy and exercise-based rehabilitation targeting the rotator cuff and scapular stabilizers represent the cornerstone of treatment.
- Most patients improve with conservative management, while surgery or injections are reserved for persistent or refractory cases.
Anatomy of the Shoulder – A Brief Overview
To better understand shoulder impingement syndrome, it is important to first review the basic anatomy of the shoulder.
The subacromial space is located between the acromion, a bony projection of the scapula that forms the “roof” of the shoulder, and the head of the humerus below. This narrow space contains several key structures that play an essential role in shoulder movement and stability.
One of the most important structures in this region is the rotator cuff, a functional group made up of four muscles and their tendons: supraspinatus, infraspinatus, teres minor, and subscapularis. These muscles are responsible for shoulder movement and, more importantly, for stabilizing the humeral head during arm motion.
The tendons of the rotator cuff attach to the humeral head and pass through the subacromial space. In addition to enabling arm movement, they play a critical role in maintaining joint stability during everyday activities and sports.
Another important structure in the subacromial space is the subacromial bursa, a small fluid-filled sac that acts as a cushion between the rotator cuff tendons and the acromion. Its main function is to reduce friction and allow smooth, pain-free shoulder movement.
The third key structure in this region is the long head of the biceps tendon. It assists in elbow flexion and forearm rotation, while also contributing as a secondary stabilizer of the shoulder joint.
Shoulder Impingement Syndrome – How Common Is It and Who Is Affected?
Subacromial impingement is one of the most common causes of shoulder pain and accounts for a large proportion of shoulder-related complaints seen in clinical practice. It is estimated to be responsible for nearly half of all cases of shoulder pain.
The prevalence increases with age, with the condition most frequently affecting individuals in their 50s and 60s. This age-related rise is largely associated with gradual degenerative changes in the rotator cuff tendons and reduced shoulder mechanics over time.
Shoulder impingement syndrome is particularly common in people who regularly perform repetitive overhead movements. This includes athletes involved in sports such as handball, volleyball, swimming, and other disciplines that require frequent arm elevation above shoulder level.
Certain occupational groups are also at higher risk, especially those whose work involves repeated lifting or sustained overhead arm positions. These include carpenters, electricians, painters, and other manual labor professions where the shoulder is frequently exposed to mechanical overload.
How Does Subacromial Impingement Develop?
The space between the acromion and the head of the humerus, known as the subacromial space, is normally narrow and typically measures around 10 to 15 millimeters. Within this confined anatomical region lie several important structures essential for normal shoulder function.
These include the subacromial bursa, the rotator cuff tendons, and the long head of the biceps tendon. All of these structures need to glide smoothly during shoulder movement, particularly during arm elevation.
Subacromial impingement develops when these soft tissues become irritated or mechanically compressed during movement of the shoulder. This repeated friction can lead to pain, inflammation, and progressive impairment of shoulder function and mobility.
Depending on the underlying mechanism, subacromial impingement is generally divided into two main types.
Primary Subacromial Impingement – Structural Impingement
Primary subacromial impingement develops due to structural changes that reduce the available space within the subacromial region. A common cause is the presence of bony outgrowths (osteophytes) on the undersurface of the acromion, which can narrow the subacromial space and increase mechanical pressure on the soft tissues.
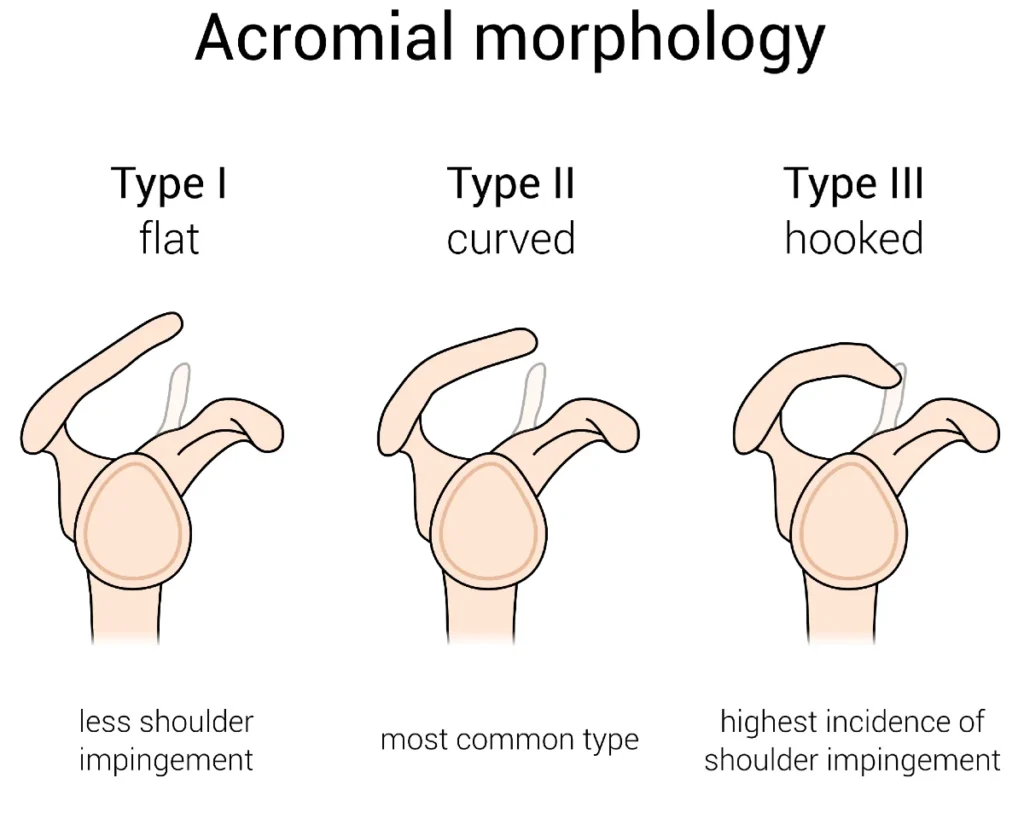
In some individuals, the shape of the acromion itself contributes to this narrowing. A naturally curved or hooked acromion, known as a type III acromion, can further reduce the subacromial space and increase the likelihood of tendon compression during shoulder movement.
In the past, primary (structural) impingement was considered the main and almost exclusive cause of subacromial impingement. However, current evidence suggests that purely structural factors account for only a small proportion of cases.
Secondary Subacromial Impingement – Functional Impingement Syndrome
Secondary or functional subacromial impingement occurs when the shoulder appears anatomically normal at rest, but dynamic movement leads to compression of the soft tissues within the subacromial space.
This mechanism is primarily related to weakness or poor neuromuscular control of the rotator cuff muscles, which play a central role in stabilizing the humeral head during arm movement. When these stabilizing muscles are not functioning optimally, the humeral head may migrate superiorly toward the acromion, reducing the subacromial space and creating impingement during motion.
Weakness or poor coordination of the scapular stabilizing muscles, particularly the lower trapezius and serratus anterior, can further contribute to this condition. Inadequate scapular control may position the shoulder in a mechanically disadvantageous alignment during arm elevation, further narrowing the subacromial space.
According to current research, the functional (secondary) form of subacromial impingement is the most common presentation. This has important implications for diagnosis, rehabilitation, and overall treatment strategy.
Symptoms of Shoulder Impingement Syndrome
Patients with shoulder impingement syndrome commonly report pain when lifting the arm or when lying on the affected shoulder.
Night pain is particularly characteristic and often more pronounced, especially when sleeping on the painful side or with the arm positioned overhead. Over time, persistent pain and reduced use of the joint may lead to muscle weakness and stiffness in the shoulder.
Typical symptoms include:
- Pain when lifting the arm above shoulder level
- Pain during overhead activities such as reaching, dressing, or lifting
- Night pain, especially when lying on the affected side
- Weakness in the shoulder muscles
- Gradual loss of range of motion and increasing stiffness
The onset of symptoms is usually gradual, developing over weeks or months. In many cases, patients cannot identify a specific injury or triggering event. However, symptoms may also be triggered or worsened after minor overuse or a sudden movement, such as an awkward reach or a quick jerk of the arm.
Pain is most commonly felt at the front and outer aspect of the shoulder. In some cases, it may radiate into the upper arm and occasionally extend toward the elbow.
Symptoms may temporarily improve with rest, pain medication, or cold application. However, once normal activities are resumed, the pain often returns.
Over time, persistent symptoms can significantly affect daily functioning, including dressing, personal hygiene, work activities, and other routine movements.
How Is Shoulder Impingement Syndrome Diagnosed?
A thorough clinical history and a careful physical examination are the most important steps in diagnosing shoulder impingement syndrome.
The first step involves a detailed conversation between the physician and the patient regarding shoulder pain, known as the medical history (anamnesis). During this discussion, it is important to gather information about when the pain started, how it feels, what aggravates or relieves it, and how it affects daily activities. Previous treatments and their outcomes, as well as any history of shoulder injuries, should also be taken into account.
This is followed by a physical examination, during which the physician assesses shoulder range of motion, joint stability, and areas of tenderness. In shoulder impingement syndrome, several characteristic findings may be present:
- Strength may be reduced, usually due to pain inhibition rather than true muscle weakness
- Range of motion is typically preserved, without major restriction
- Mild limitation may be present in terminal external rotation and abduction
- A painful arc is often observed during abduction, typically between 60° and 120°, commonly associated with supraspinatus tendon irritation
Specific clinical tests are used to support the diagnosis, including the Neer test and the Hawkins-Kennedy test. These maneuvers aim to reproduce subacromial impingement and elicit pain. However, these tests are not specific and may also be positive in other shoulder conditions, such as calcific tendinopathy or subacromial bursitis.
In most cases, the combination of medical history and clinical examination is sufficient to establish a working diagnosis.
In certain situations, an X-ray of the shoulder may be recommended to rule out structural abnormalities, calcific tendinopathy, or shoulder osteoarthritis. Advanced imaging such as ultrasound or magnetic resonance imaging (MRI) is not routinely required but may be helpful if symptoms persist despite appropriate treatment.
MRI provides a detailed evaluation of both bone and soft tissue structures of the shoulder. Ultrasound is particularly useful for identifying soft tissue conditions such as bursitis, tendinopathies, or rotator cuff tears.
Shoulder Impingement Treatment
Treatment of shoulder impingement syndrome is individualized for each patient. The underlying cause, severity of symptoms, and duration of complaints all play an important role in guiding management decisions.
In most cases, treatment is conservative and does not require surgery. The first step usually involves activity modification, particularly avoiding movements that provoke pain, such as repetitive overhead activities.
Pain-relieving medications such as paracetamol (acetaminophen) or nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly used to reduce symptoms. While these medications can help control pain, they do not address the underlying cause and should not be considered a long-term treatment solution.
1. Physical Therapy and Shoulder Impingement Exercises
Physical therapy and structured exercise programs are the most important components in the treatment of shoulder impingement syndrome. The main goal is not only pain reduction, but also restoration of normal shoulder mechanics and prevention of recurrence.
Exercises focuses on improving strength, coordination, and control of the shoulder complex. Particular attention is given to the rotator cuff muscles and the scapular stabilizers, as their proper function is essential for maintaining optimal positioning of the humeral head within the joint.
A typical rehabilitation program includes:
- Strengthening exercises for the rotator cuff muscles
- Scapular stabilization training, especially the lower trapezius and serratus anterior
- Mobility exercises to improve shoulder range of motion
- Postural correction and movement re-education
- Gradual return to overhead activities in a controlled manner
Early stages of rehabilitation often focus on pain-free isometric exercises, progressing gradually to dynamic strengthening and functional movements as symptoms improve. Proper load management is essential to avoid aggravation of symptoms and to support tissue recovery.
When performed consistently and correctly, physical therapy has been shown to significantly improve pain, function, and long-term outcomes in patients with shoulder impingement syndrome.
2. Injection Therapy
If symptoms do not improve with physiotherapy and pain medication, injection therapy may be considered as part of the treatment plan for shoulder impingement syndrome.
Corticosteroid injections are commonly used to reduce inflammation and provide short-term pain relief, particularly in patients with significant pain that limits participation in rehabilitation. These injections can help improve comfort and allow more effective engagement in physical therapy.
In addition to corticosteroids, hyaluronic acid injections may also be used in selected cases. Hyaluronic acid is thought to improve joint lubrication and reduce friction within the shoulder, potentially supporting smoother movement and symptom relief. While evidence is more variable compared to other joints, it may be considered as an adjunct option in chronic or degenerative presentations.
Whenever possible, injections should be performed under ultrasound guidance to ensure accurate placement within the subacromial space. In patients with severe pain, injection therapy may be used early to facilitate participation in rehabilitation exercises.
3. Surgical Treatment
Surgery may be considered when conservative treatment fails to provide sufficient improvement. The most commonly performed procedure is subacromial decompression, which is typically carried out arthroscopically.
Current evidence suggests that subacromial decompression does not provide better long-term outcomes than well-structured physiotherapy. Therefore, surgery should be reserved for carefully selected patients. In cases of rotator cuff tendon rupture, particularly after trauma or in patients under 60 years of age, arthroscopic rotator cuff repair may be recommended.
Prognosis
With an accurate diagnosis and an appropriate treatment approach, most patients with shoulder impingement syndrome experience a significant improvement in symptoms. In the majority of cases, this allows a gradual return to normal daily activities without major limitations.
Prevention and Long-Term Shoulder Health
Key strategies to help prevent subacromial impingement and maintain long-term shoulder health include:
- Maintaining proper posture at work, during sports, and in daily life
- Avoiding repetitive movements that overload the shoulder, especially overhead activities
- Performing adequate warm-up before physical activity
- Maintaining strength and mobility of the rotator cuff and scapular stabilizing muscles
- Preserving a balanced strength relationship between the anterior and posterior shoulder muscles
It is also important to listen to the body and allow sufficient rest and recovery when shoulder pain or discomfort occurs, especially during periods of increased load.
Frequently Asked Questions (FAQ)
1. What other conditions can cause symptoms similar to shoulder impingement syndrome?
Several shoulder conditions can present with very similar symptoms, including rotator cuff tendinopathy, subacromial bursitis, adhesive capsulitis (frozen shoulder), and early glenohumeral osteoarthritis. Clinical examination alone may sometimes overlap, which is why imaging can be helpful in persistent cases.
Still unsure what is causing your shoulder pain? Explore the most common underlying conditions, symptoms, and diagnostic patterns in our comprehensive guide on shoulder pain. Learn more about possible causes of shoulder pain here.
2. How can shoulder impingement syndrome be distinguished from a rotator cuff tear?
Both conditions can cause shoulder pain and weakness, but a rotator cuff tear more often presents with a more pronounced loss of strength, especially during specific movements such as abduction or external rotation. In contrast, shoulder impingement syndrome typically shows pain-related weakness rather than true structural loss of strength. Imaging such as ultrasound or MRI is often required for definitive differentiation.
3. How can shoulder impingement syndrome be differentiated from chronic calcific tendinopathy?
Calcific tendinopathy can closely mimic subacromial impingement, as both conditions cause lateral shoulder pain and painful arm elevation. However, calcific deposits within the rotator cuff tendons can sometimes lead to more acute pain flare-ups. In many cases, ultrasound or X-ray is necessary to confirm calcifications, as clinical examination alone is often not sufficient for differentiation.
4. Can shoulder impingement syndrome heal without surgery?
Yes, most cases improve significantly with conservative treatment, especially physiotherapy and activity modification. Surgery is only considered in selected cases that do not respond to non-operative management.
5. Is exercise safe for shoulder impingement syndrome?
Yes, but it must be appropriately prescribed. Correctly guided physiotherapy exercises are essential for recovery, while uncontrolled or painful overhead loading can worsen symptoms.
6. How long does shoulder impingement syndrome take to recover?
Recovery time varies depending on severity and adherence to rehabilitation, but many patients experience improvement within several weeks to a few months of consistent treatment.
7. When should I see a doctor for shoulder pain?
Medical evaluation is recommended if shoulder pain persists for more than a few weeks, worsens over time, or significantly limits daily activities or sleep.
Creech JA, Busse A, Li D, et al. Shoulder Impingement Syndrome. [Updated 2026 Jan 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. StatPearls: Shoulder Impingement Syndrome overview
Diercks R, Bron C, Dorrestijn O, Meskers C, Naber R, de Ruiter T, Willems J, Winters J, van der Woude HJ; Dutch Orthopaedic Association. Guideline for diagnosis and treatment of subacromial pain syndrome: a multidisciplinary review. Acta Orthop. 2014 Jun;85(3):314-22. doi: 10.3109/17453674.2014.920991. Clinical guideline: Subacromial pain syndrome diagnosis and treatment
Witten A, Mikkelsen K, Wagenblast Mayntzhusen T, Clausen MB, Thorborg K, Hölmich P, Barfod KW. Terminology and diagnostic criteria used in studies investigating subacromial pain syndrome (1972–2019): a scoping review. Br J Sports Med. 2023;57(13):864-871. Scoping review: Diagnostic criteria for subacromial pain syndrome
Lewis J. Rotator cuff related shoulder pain: Assessment, management and uncertainties. Man Ther. 2016 Jun;23:57-68. Review: Rotator cuff-related shoulder pain assessment and management
Varacallo MA, El Bitar Y, Sina RE, et al. Rotator Cuff Syndrome. [Updated 2024 Mar 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. StatPearls: Rotator cuff syndrome clinical overview
Dubé MO, Desmeules F, Lewis J, Roy JS. Rotator cuff-related shoulder pain: does the type of exercise influence outcomes? BMJ Open. 2020;10(11):e039976. doi: 10.1136/bmjopen-2020-039976. BMJ Open: Exercise-based rehabilitation in rotator cuff-related shoulder pain
Lo CN, Leung BPL, Sanders G, et al. The major pain source of rotator cuff-related shoulder pain: a narrative review. Musculoskeletal Care. 2023;21(2):285-293. Narrative review: Pain mechanisms in rotator cuff-related shoulder pain
Powell JK, Lewis JS. Rotator Cuff-Related Shoulder Pain: Is It Time to Reframe the Advice “You Need to Strengthen Your Shoulder”? J Orthop Sports Phys Ther. 2021;51(4):156-158. Clinical perspective: Exercise and rehabilitation recommendations