Shoulder pain is a common complaint that can arise from a wide range of conditions, varying from mild soft tissue irritation to more complex structural problems. While many patients try to identify the cause based on symptoms alone, shoulder pain is rarely straightforward. The same type of discomfort may originate from different anatomical structures, and similar conditions can present in very different ways.
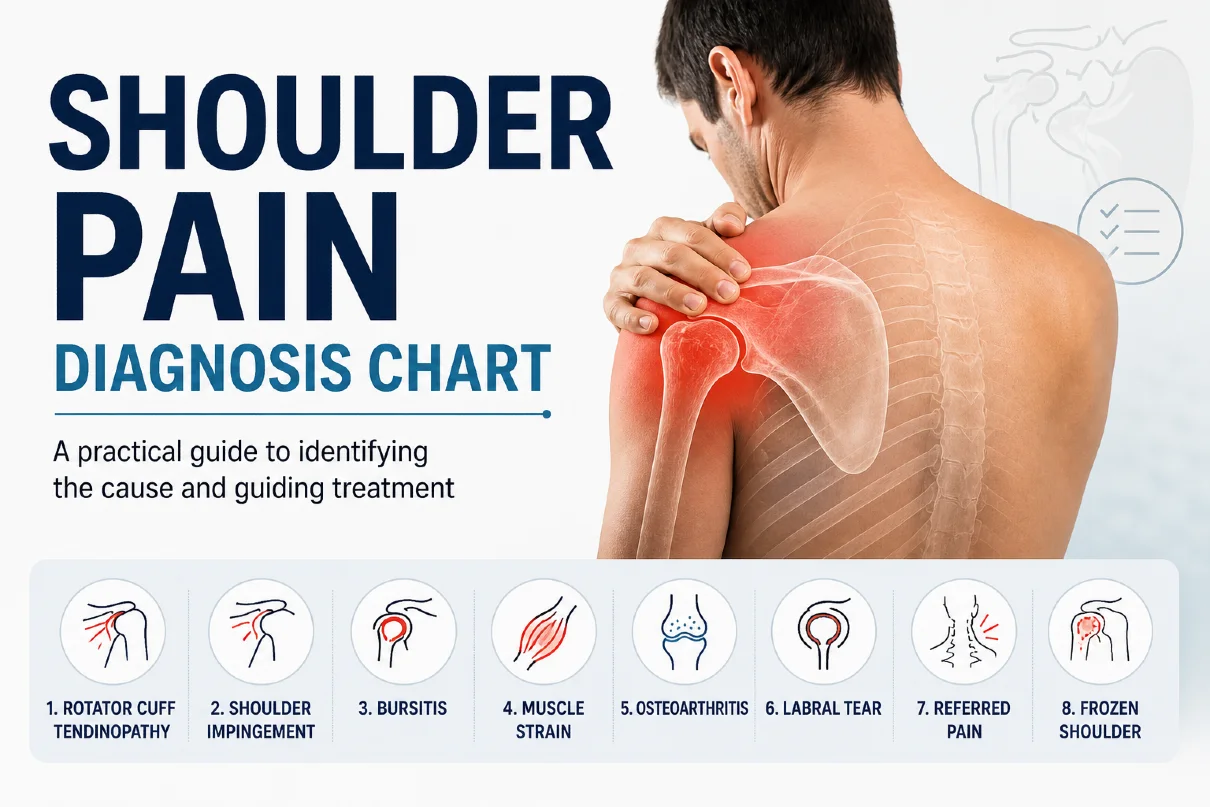
In clinical practice, an accurate diagnosis begins with a careful assessment of pain location, movement limitations, and associated symptoms. Understanding these patterns can provide valuable insight into the underlying cause, but it is important to approach this process with nuance rather than assumption. A shoulder pain diagnosis chart can be a useful clinical framework for organizing these patterns and improving diagnostic clarity.
This article outlines a practical, clinician-informed approach to shoulder pain diagnosis, helping you better understand what your symptoms may indicate—and when it is time to seek professional care.
Why Shoulder Pain Is Not Always Easy to Diagnose
Shoulder pain is a common issue, but identifying its exact cause is not always straightforward. The shoulder is a highly complex joint made up of multiple muscles, tendons, and supporting structures that work together to allow a wide range of motion. Because of this, different conditions can produce very similar symptoms, making it difficult to rely on pain alone as a clear indicator.
In clinical practice, an accurate diagnosis depends on recognizing patterns rather than focusing on a single symptom. Factors such as pain location, movement limitations, and associated signs all play a role in understanding the underlying cause. This is why a structured approach is essential when evaluating shoulder pain.
A Structured Approach to Shoulder Pain Diagnosis
Accurately diagnosing shoulder pain requires more than identifying where it hurts. In clinical practice, evaluation is based on recognizing patterns that emerge from a combination of symptoms rather than relying on a single complaint.
A structured approach provides a clear diagnostic framework that helps differentiate between common conditions that may initially present with similar symptoms. Instead of focusing on isolated findings, clinicians interpret multiple factors together to better understand the underlying cause.
This framework typically includes several key elements:
- location of pain
- response to movement
- range of motion and functional limitation
- associated symptoms such as weakness or stiffness
In clinical practice, these elements are often organized using a shoulder pain diagnosis chart, which helps systematically interpret symptom patterns and supports more consistent clinical reasoning.
When assessed together, these factors provide a more reliable and clinically meaningful diagnosis than evaluating any single symptom in isolation.
The Importance of Pain Location
The location of shoulder pain is often the first clue in the diagnostic process. While it is not definitive on its own, it can help narrow down the structures most likely involved. For example, pain in the front of the shoulder is frequently associated with the biceps tendon or labral structures, whereas pain felt on the lateral aspect of the shoulder is more commonly linked to the rotator cuff.
However, it is important to recognize that patients do not always localize pain precisely. Discomfort may be described as diffuse or may radiate into the upper arm, which can make interpretation less straightforward. For this reason, pain location should always be considered alongside other clinical findings.
How Movement Influences Shoulder Pain
The way shoulder pain responds to movement provides valuable diagnostic insight. Pain that occurs primarily during specific activities, such as lifting the arm or reaching overhead, often suggests involvement of the tendons or muscles responsible for those actions. In contrast, pain that persists at rest or during the night may indicate a more advanced or inflammatory condition.
In clinical settings, particular attention is given to movements that consistently reproduce symptoms. Identifying these patterns helps differentiate between mechanical causes of pain and those that may require further investigation.
Range of Motion and Functional Limitation
Assessing range of motion is a key component of shoulder evaluation. A distinction is made between active movement, performed by the patient, and passive movement, assessed by the examiner. When both active and passive movements are restricted, this may point toward joint-related conditions such as adhesive capsulitis.
On the other hand, if passive range of motion is preserved but active movement is painful or limited, this often suggests involvement of the muscles or tendons, particularly within the rotator cuff. Functional limitations, such as difficulty reaching overhead or behind the back, also provide important context in understanding the severity and nature of the condition.
Associated Symptoms That Provide Clues
In addition to pain itself, associated symptoms can offer important diagnostic clues. A sense of weakness may indicate tendon involvement or muscle dysfunction, while progressive stiffness is commonly seen in conditions such as frozen shoulder. Night pain, particularly when it disrupts sleep, is another feature that may suggest a more significant underlying issue.
These accompanying signs help complete the clinical picture and should always be considered as part of a broader assessment. When evaluated together with pain location and movement patterns, they contribute to a more accurate and reliable understanding of shoulder pain.
Shoulder Pain by Location: What Your Symptoms May Indicate
The location of shoulder pain often provides one of the most useful starting points in understanding its underlying cause. Although it should never be used in isolation, pain distribution can help identify which anatomical structures are most likely involved.
While pain location is an important part of the diagnostic framework, it becomes most useful when interpreted in a clinical context. The patterns below illustrate how different pain distributions may point toward specific underlying conditions.
Pain in the Front of the Shoulder
Pain located in the front of the shoulder (anterior shoulder pain) is commonly associated with structures such as the biceps tendon or the labrum. Patients often describe discomfort during activities that involve lifting, carrying, or reaching forward. This type of pain may also be aggravated by repetitive overhead movements or resistance-based exercises.
In some cases, anterior shoulder pain can develop gradually due to overuse, particularly in physically active individuals. However, it may also follow a specific strain or injury. Because several structures in this region are closely related, distinguishing between them requires careful assessment of movement and symptom patterns.
Pain on the Side of the Shoulder
Pain felt on the lateral aspect of the shoulder is one of the most frequently reported patterns in clinical practice. It is often linked to rotator cuff disorders or shoulder impingement, particularly in individuals over the age of 40 or those engaged in repetitive overhead activity.
This type of pain is typically worsened by lifting the arm away from the body or reaching above shoulder level. Patients may also report difficulty sleeping on the affected side.
This pattern most often reflects overlap between rotator cuff tendinopathy and subacromial impingement syndrome. Differentiation between these conditions is usually based on clinical examination, particularly strength testing and movement-provocation tests.
Pain at the Top of the Shoulder
Pain localized at the top of the shoulder is often related to the acromioclavicular (AC) joint. This type of discomfort is usually more focal and can be reproduced with specific movements, such as bringing the arm across the body or lifting objects overhead.
AC joint-related pain may develop following direct trauma, such as a fall onto the shoulder, or as a result of chronic stress and degeneration over time. In some cases, swelling or tenderness over the joint may also be present, providing an additional clinical clue.
Pain in the Back of the Shoulder
Pain in the back of the shoulder is less commonly associated with primary shoulder joint pathology and may instead be related to posture, muscle imbalance, or referred pain from the cervical spine. Patients often describe a deep, diffuse discomfort that may extend toward the upper back or neck.
This pattern is frequently seen in individuals with prolonged sitting habits or poor ergonomic positioning. In such cases, the pain may not be directly linked to shoulder movement itself but rather to sustained muscle tension or altered biomechanics. A broader assessment is therefore important to identify contributing factors beyond the shoulder joint alone.
Onset of Symptoms: Acute vs Gradual Shoulder Pain
The onset of shoulder pain refers to how symptoms begin, either suddenly or gradually over time. This distinction is an important part of clinical evaluation, as it helps differentiate between acute injuries and chronic degenerative conditions.
In practice, the onset of symptoms is always interpreted together with pain location and movement patterns, since no single factor is sufficient to establish a diagnosis.
Acute onset (sudden shoulder pain)
Acute shoulder pain begins suddenly and is often associated with a specific event, such as trauma, lifting, or a sudden movement. Patients can usually identify the exact moment when symptoms started.
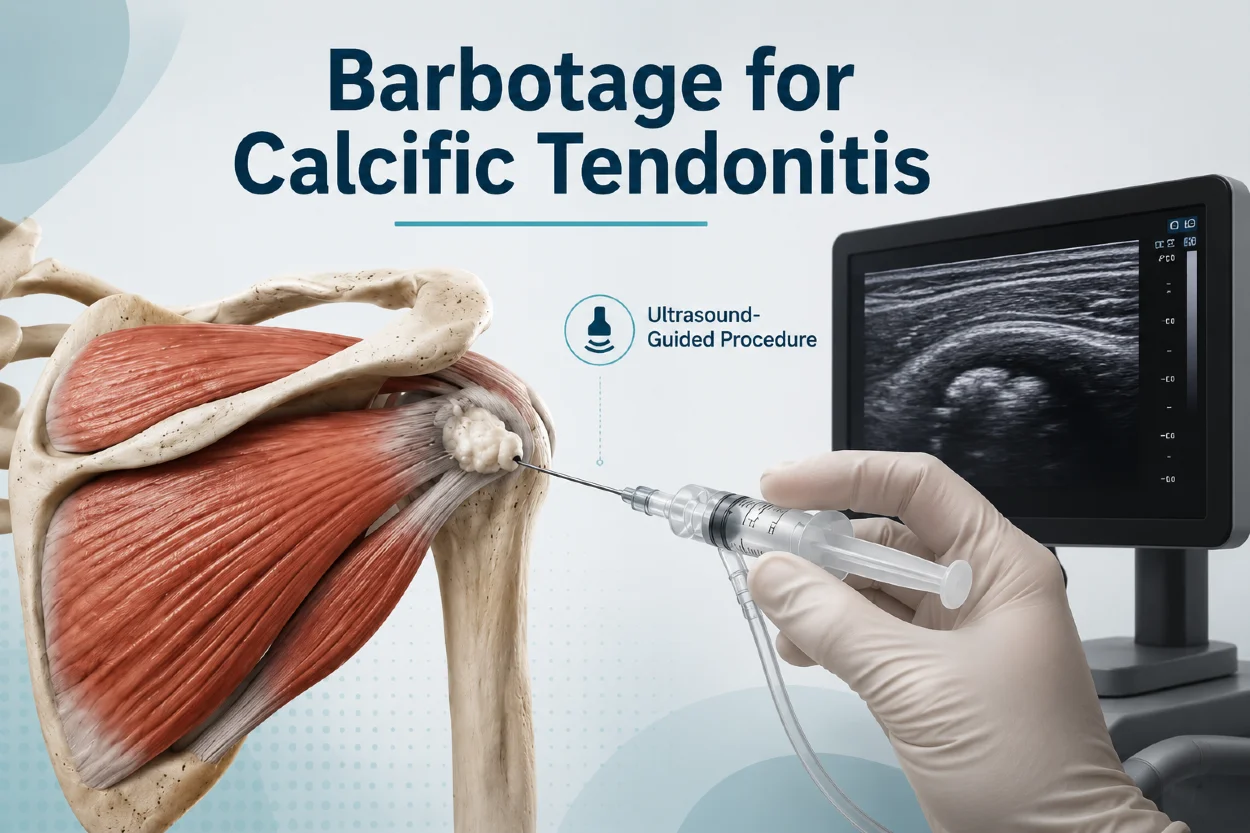
This pattern is most commonly seen in conditions such as rotator cuff tears following trauma, shoulder dislocation, or acute calcific tendinitis. Unlike traumatic injuries, acute calcific tendinitis often develops spontaneously, although symptoms may sometimes be triggered or aggravated by physical activity.
Pain is often more intense and may be accompanied by weakness, reduced range of motion, or a sudden loss of function.
Clinical Insight
Because acute onset may indicate structural injury or an active inflammatory process, early clinical assessment is often necessary.
Gradual (insidious) onset
In contrast, gradual shoulder pain develops slowly over time and is usually related to overuse, repetitive strain, or degenerative changes. Symptoms may initially be mild and intermittent, but tend to progress and become more persistent.
This pattern is typically associated with conditions such as shoulder impingement syndrome, chronic rotator cuff tendinopathy, or degenerative tendon changes. In the early stages, pain is often activity-related, but it may later occur at rest or during the night.
Why onset matters in diagnosis
Distinguishing between sudden and gradual onset provides important clinical context. Acute onset is more suggestive of injury or sudden pathological change, while gradual onset is more commonly linked to chronic mechanical or degenerative processes.
When combined with pain location, movement response, and functional limitation, onset becomes a key component of a structured approach to shoulder pain diagnosis.
How Movement Influences Shoulder Pain
The way shoulder pain responds to movement provides important diagnostic information and often helps differentiate between common shoulder conditions. Certain movement patterns are strongly associated with specific anatomical structures, making dynamic assessment a key part of clinical evaluation.
Pain during cross-body adduction is most commonly associated with acromioclavicular (AC) joint pathology. Patients typically experience localized pain at the top of the shoulder when the arm is moved across the midline of the body, particularly in terminal range of motion. This pattern is characteristic of AC joint irritation or degenerative changes.
A painful arc during shoulder abduction is another important clinical sign, most often seen in rotator cuff-related conditions such as supraspinatus tendinopathy, shoulder impingement syndrome, partial rotator cuff tears, and chronic calcific tendinitis. Pain typically occurs between approximately 60 and 120 degrees of abduction, corresponding to increased mechanical compression of the rotator cuff tendons beneath the acromion.
In acute conditions such as rotator cuff rupture, acute bursitis, or acute calcific tendinitis, movement is often significantly limited due to pain, and patients may avoid active shoulder motion altogether. In contrast, chronic conditions such as tendinopathy or degenerative tears usually allow preserved movement, but pain increases with specific ranges, load, or repetitive activity. Recognizing these movement-based patterns is essential for narrowing the differential diagnosis and improving clinical accuracy.
Common Shoulder Conditions Explained in a Clinical Context
While shoulder pain can present in many different ways, several conditions are consistently encountered in clinical practice. Understanding how these disorders typically develop and present helps place symptoms into a clearer context. Rather than viewing them as isolated diagnoses, it is often more useful to consider how each condition fits within a broader pattern of movement, pain distribution, and functional limitation.
Rotator cuff disorders are among the most common causes of shoulder pain, particularly in middle-aged and older individuals. They often present with lateral shoulder pain that worsens during overhead activities or when lifting the arm away from the body. Depending on the severity, this may range from mild tendon irritation to partial or full-thickness tears. Patients frequently report weakness or difficulty performing everyday movements, such as reaching or carrying objects.
Frozen shoulder, or adhesive capsulitis, is characterized by a progressive loss of both active and passive range of motion. It typically develops gradually, often without a clear initial injury, and may be accompanied by deep, aching pain that worsens over time. In clinical settings, the defining feature is stiffness rather than isolated pain, with patients experiencing increasing difficulty in performing routine tasks such as dressing or reaching behind the back.
Shoulder impingement refers to a condition in which the tendons of the rotator cuff become compressed during certain movements, particularly when the arm is elevated. This often results in pain during mid-range motion, especially when lifting the arm overhead. It is commonly associated with repetitive use, poor movement mechanics, or structural factors that reduce the available space within the shoulder.
Biceps tendinopathy is typically associated with pain in the front of the shoulder, often described as a localized discomfort that may worsen with lifting, pulling, or repetitive arm use. It can develop as a result of overuse or in combination with other shoulder conditions, particularly those affecting the rotator cuff. In some cases, patients may also report a sense of tenderness along the course of the tendon.
A more detailed overview of shoulder pain patterns, underlying causes, and clinical considerations is available in a dedicated article on shoulder pain , which may be helpful for further understanding the topic.
A Practical Shoulder Pain Diagnosis Chart
A structured shoulder pain “diagnosis chart” can help organize shoulder symptoms into more clinically meaningful patterns. While it is not a substitute for a full medical assessment, it provides a useful framework for understanding which conditions are more likely based on pain location, triggers, and functional limitations.
In general, anterior shoulder pain is often associated with biceps tendon pathology or labral involvement, particularly when symptoms are aggravated by lifting or pulling movements. Lateral shoulder pain most commonly suggests rotator cuff disorders, including impingement syndrome and degenerative tendon changes, especially when pain is provoked by overhead activity or side-lying positions.
When pain is localized at the top of the shoulder, the acromioclavicular (AC) joint should be considered. Degeneration or injury of the AC joint is frequently seen in both acute trauma and long-term wear-and-tear, and symptoms are often reproduced when the arm is moved across the body or during direct pressure on the joint.
A more diffuse or deep shoulder pain pattern may indicate degenerative or inflammatory joint disease. Osteoarthritis of the shoulder can present with gradual stiffness and aching pain, while inflammatory arthritides may involve broader joint symptoms and morning stiffness. In these cases, pain is often less activity-specific and more persistent throughout the day.
Calcific tendinopathy is another important condition to consider, particularly in cases of sudden, severe shoulder pain without clear injury. It is caused by calcium deposits within the rotator cuff tendons and can lead to acute inflammation, significantly limiting movement and function.
Finally, it is important to recognize that multiple conditions may coexist. Degenerative changes, tendon pathology, and joint involvement can overlap, making clinical correlation essential.
The chart below summarizes these common patterns in a simplified form:
| Pain Pattern | Onset & Movement Pattern | Most Likely Causes | Typical Clinical Features |
|---|---|---|---|
| Front of shoulder pain | Gradual onset; worsens with lifting, pulling, or overhead activity | Biceps tendinopathy, labral pathology | Activity-related anterior pain; often provoked by resistance or repetitive use |
| Side of shoulder pain | Painful arc (60–120° abduction); worse with overhead movement; gradual onset | Rotator cuff tendinopathy, subacromial impingement, partial tears, chronic calcific tendinitis | Pain during mid-range abduction; often worse at night or when lying on affected side |
| Top of shoulder pain | Pain with cross-body adduction or terminal range of motion; gradual or post-traumatic onset | AC joint degeneration or injury | Well-localized superior shoulder pain; reproduced by cross-body movement or direct pressure |
| Deep or diffuse shoulder pain | Gradual onset; stiffness dominant; global movement restriction | Shoulder osteoarthritis, inflammatory arthritis | Progressive stiffness, reduced ROM, morning stiffness, grinding sensation |
| Sudden severe shoulder pain | Acute onset; marked movement limitation due to pain | Acute calcific tendinitis, rotator cuff tear, shoulder dislocation, acute bursitis | Severe pain with sudden loss of function; may present with inflammatory flare |
When Shoulder Pain Requires Medical Evaluation
Not all shoulder pain requires immediate medical attention, but certain patterns should prompt a more careful clinical evaluation. Persistent pain that does not improve with rest or basic activity modification may indicate an underlying structural or inflammatory condition that requires further assessment.
It is also important to consider functional impact. When shoulder pain begins to interfere with everyday activities such as dressing, lifting objects, or sleeping, this often suggests that the condition is progressing beyond a mild self-limiting issue. In such cases, early evaluation can help prevent further deterioration and guide appropriate treatment.
Another important consideration is the duration and progression of symptoms. Pain that gradually worsens over time, or fails to show any improvement over several weeks, should not be ignored. A structured clinical examination is often needed to clarify the cause and determine the most appropriate management strategy.
Red Flags That Should Not Be Ignored
While most cases of shoulder pain are related to musculoskeletal conditions, certain symptoms may indicate a more serious underlying problem. Sudden onset of severe pain following trauma, particularly if accompanied by visible deformity or inability to move the arm, may suggest a fracture or dislocation and requires urgent assessment.
Night pain that consistently disrupts sleep, especially when unrelated to movement or position, can also be a warning sign. Although it is sometimes seen in common conditions such as rotator cuff disorders, it may also indicate more significant pathology when persistent or progressive.
Neurological symptoms such as numbness, tingling, or radiating pain into the arm should also be taken seriously, as they may suggest cervical spine involvement or nerve compression. Similarly, systemic symptoms such as fever, unexplained weight loss, or general malaise in combination with shoulder pain warrant further investigation.
Final Thoughts on Understanding Shoulder Pain Patterns
Shoulder pain is best understood as a pattern rather than a single isolated symptom. Because multiple structures can produce similar clinical presentations, accurate interpretation depends on combining several factors, including pain location, movement patterns, range of motion, and associated symptoms.
A structured approach, such as a diagnosis chart, can help organize these observations and provide a clearer clinical perspective. However, it should always be viewed as a guide rather than a definitive diagnostic tool. In many cases, careful clinical examination remains essential to confirm the underlying cause.
Understanding these patterns allows for earlier recognition of common conditions and more appropriate decision-making regarding treatment or further evaluation.
Key Takeaway
Shoulder pain should be interpreted through patterns rather than isolated symptoms. A structured clinical approach—considering pain location, movement response, range of motion, and associated features—helps narrow down the most likely cause, but a definitive diagnosis always requires proper clinical evaluation.
FAQ About Shoulder Pain
What is a shoulder pain diagnosis chart?
A shoulder pain diagnosis chart is a clinical tool used to organize symptoms based on pain location, movement patterns, and associated features. It helps narrow down possible causes such as rotator cuff disorders, AC joint problems, or tendon-related conditions, but it does not replace a full medical examination. In clinical practice, a shoulder pain diagnosis chart is often used as a structured reference to guide initial assessment.
Can shoulder pain be diagnosed based on location alone?
Pain location provides useful clues, but it is not sufficient for a definitive diagnosis. Many different conditions can cause pain in the same area of the shoulder, which is why additional factors such as movement, strength, and range of motion must also be considered.
What is the most common cause of shoulder pain?
Rotator cuff disorders are among the most common causes of shoulder pain, especially in adults over 40. These conditions often present with lateral shoulder pain that worsens during overhead movements or repetitive arm use.
When should I worry about shoulder pain?
Shoulder pain should be evaluated if it persists for several weeks, worsens over time, or significantly affects daily activities. Red flags include severe trauma, inability to move the arm, night pain that disrupts sleep, or neurological symptoms such as numbness or tingling.
Is shoulder pain always related to injury?
No. Shoulder pain can develop gradually without a specific injury. Degenerative changes, overuse, inflammatory conditions, and posture-related strain are all common non-traumatic causes.
Lewis JS. Rotator cuff tendinopathy: a model for the continuum of pathology and related management. British Journal of Sports Medicine. Review article: Rotator cuff tendinopathy mechanisms and treatment
Seitz AL et al. Mechanisms of rotator cuff tendinopathy: intrinsic, extrinsic, or both? Clinical Biomechanics. Study on causes of rotator cuff disease and impingement
Yamamoto A et al. Prevalence and risk factors of a rotator cuff tear in the general population. Journal of Shoulder and Elbow Surgery. Epidemiological study on rotator cuff tears
Michener LA, McClure PW, Karduna AR. Anatomical and biomechanical mechanisms of subacromial impingement syndrome. Clinical Biomechanics. Study on biomechanical mechanisms of shoulder impingement
Uppal HS, Evans JP, Smith C. Frozen shoulder: A systematic review of therapeutic options. World Journal of Orthopedics. Systematic review of treatment options for adhesive capsulitis
Zuckerman JD, Rokito A. Frozen shoulder: a consensus definition. Journal of Shoulder and Elbow Surgery. Standardized definition and classification of frozen shoulder
Sansone V, Maiorano E. Calcific tendinopathy of the shoulder: clinical perspectives. Orthopedic Research and Reviews. Review of calcific tendinitis pathogenesis and management
Speed CA, Hazleman BL. Calcific tendinitis of the shoulder. New England Journal of Medicine. NEJM review of calcific tendon disease
van der Windt DA et al. Shoulder disorders in general practice: incidence and patient characteristics. Annals of the Rheumatic Diseases. Epidemiological data on shoulder pain in primary care
Luime JJ et al. Prevalence and incidence of shoulder pain in the general population. Scandinavian Journal of Rheumatology. Population-based study of shoulder pain prevalence
Hegedus EJ et al. Physical examination tests of the shoulder: a systematic review with meta-analysis. British Journal of Sports Medicine. Diagnostic accuracy of shoulder clinical tests
Mitchell C et al. Shoulder pain: diagnosis and management in primary care. BMJ. Clinical review of shoulder pain diagnosis and treatment
Diercks RL et al. Guideline for diagnosis and treatment of subacromial pain syndrome. Acta Orthopaedica. Evidence-based guideline for subacromial shoulder pain