

Spinal stenosis is a condition defined by the narrowing of spaces within the spine—most commonly the spinal canal or neural foramina—leading to compression of the spinal cord or nerve roots. It is most often caused by age-related degenerative changes, including spondylosis, disc degeneration, and thickening of spinal ligaments.
As part of the natural aging process, spinal stenosis becomes increasingly common, particularly in the cervical (neck) and lumbar (lower back) regions. However, not all individuals with radiological narrowing develop symptoms.
When symptomatic, spinal stenosis may present with neck or back pain, radiating limb pain, numbness, tingling, muscle weakness, or reduced mobility. In more advanced cases, it can significantly impact daily activities and quality of life.
In this article, we will explain the key causes and mechanisms of spinal stenosis, outline the most common symptoms, and focus separately on cervical and lumbar stenosis, including their specific clinical features and treatment approaches.
Key Facts – Spinal Stenosis
- Spinal canal stenosis refers to the narrowing of space within the spine, leading to compression of the spinal cord or nerve roots.
- The most common cause is degenerative changes (spondylosis), including disc degeneration, osteophytes, and ligament thickening.
- It most commonly affects the cervical (neck) and lumbar (lower back) spine, particularly in older adults.
- Symptoms range from no symptoms to pain, tingling, numbness, and muscle weakness, depending on the degree of compression.
- Lumbar spinal stenosis often causes neurogenic claudication—pain and heaviness in the legs during walking, relieved by sitting or bending forward.
- Cervical spinal stenosis may lead to myelopathy, with gait disturbance, hand clumsiness, and progressive neurological deficits.
- Magnetic resonance imaging (MRI) is the gold standard for diagnosis, as it provides detailed visualization of neural compression.
- Treatment is most often conservative (exercise, physical therapy, symptom control), while surgery is considered in more severe or progressive cases.
Spinal Stenosis Definition
Spinal stenosis refers to the narrowing of the spine, most commonly within the spinal canal or neural foramina, leading to potential compression of the spinal cord or nerve roots.
The clinical significance of spinal stenosis lies in this compression of neural structures, which may result in symptoms such as pain, numbness, tingling, or weakness.
In most cases, spinal stenosis develops gradually due to age-related degenerative changes in the spine.
A key subtype is central canal stenosis, which involves narrowing of the main spinal canal and may affect multiple neural structures simultaneously.
Not all cases of spinal stenosis are symptomatic, but when the narrowing of the spine becomes significant, it can lead to clinically relevant symptoms.
Who Gets Spinal Stenosis?
Spinal stenosis (spinal canal stenosis) most commonly occurs in older adults, typically over the age of 65 years, as a result of gradual, age-related degenerative changes in the spine.
These changes develop slowly over time and are part of the natural wear-and-tear process affecting spinal structures such as intervertebral discs, facet joints, and ligaments. As degeneration progresses, it can contribute to the narrowing of the spine (spinal canal stenosis) and eventual compression of neural structures.
Although it is primarily a condition of aging, the severity and onset of symptoms can vary significantly between individuals depending on the degree of degeneration and anatomical changes.
What Causes Spinal Stenosis?
Spinal stenosis (spinal canal stenosis) is most commonly the result of degenerative changes of the spine, also known as spondylosis. This is a gradual process that develops over time and is highly prevalent in the aging population.
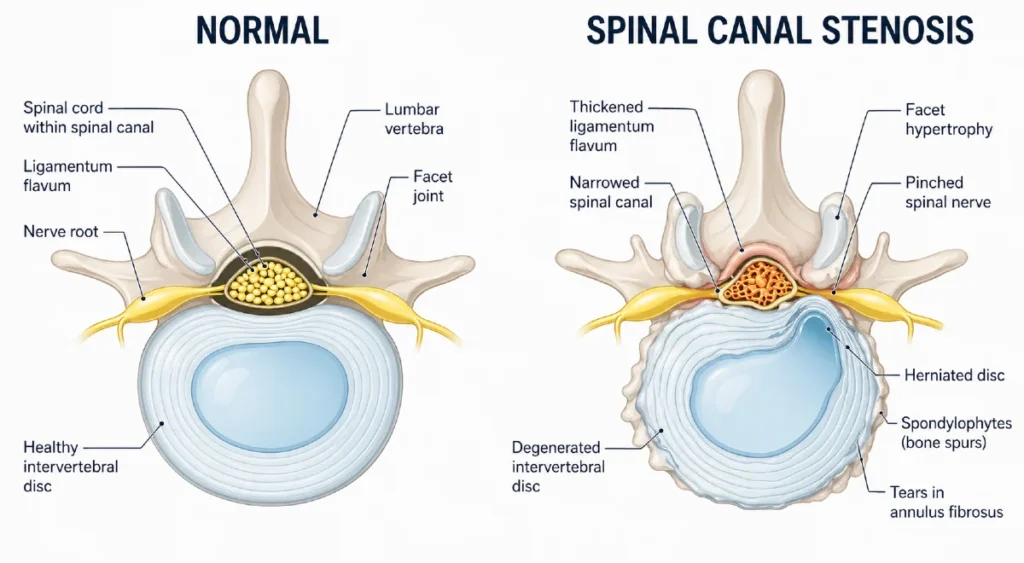
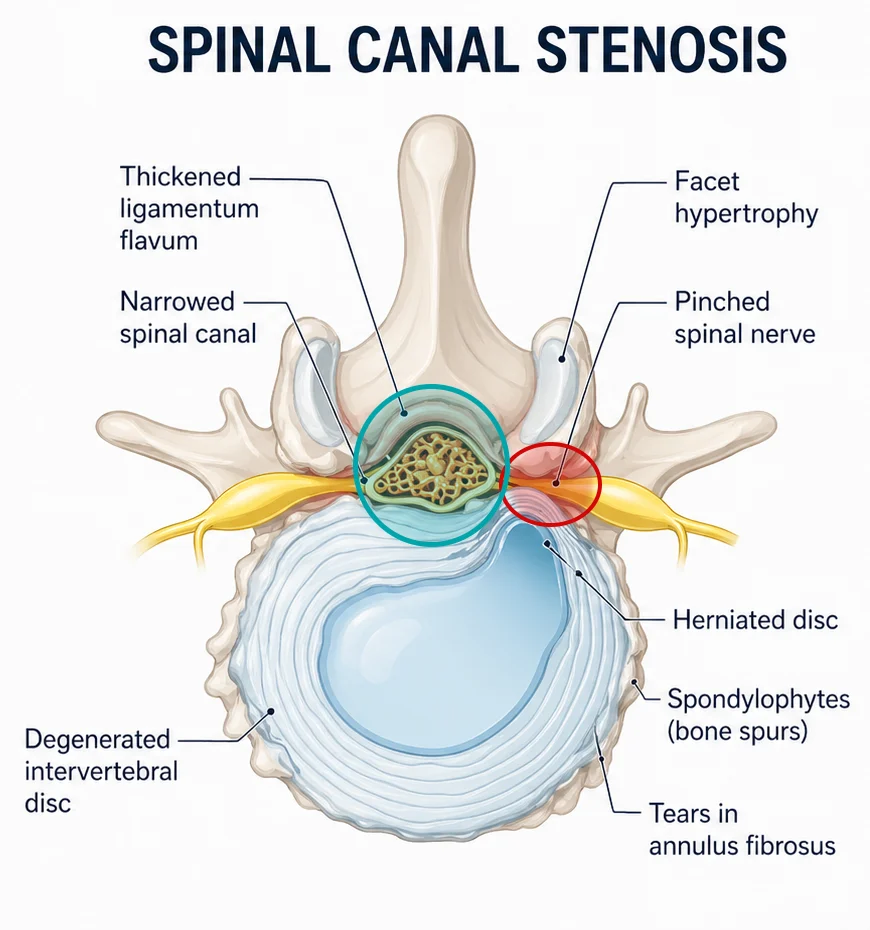
Degenerative changes include intervertebral disc degeneration, facet joint osteoarthritis, osteophyte (bone spur) formation, and thickening of the ligamentum flavum. Together, these structural changes contribute to the narrowing of the spine (spinal canal stenosis and neural foramina stenosis), leading to potential compression of neural elements.
In some cases, degenerative changes in the facet joints may also lead to spondylolisthesis, a forward or backward displacement of one vertebra relative to another, which can further reduce spinal canal space and worsen symptoms.
Although degeneration is by far the most common cause, other etiologies of spinal stenosis include:
- Space-occupying lesions, such as synovial or neural cysts, tumors, or lipomas, which can directly compress the spinal canal
- Post-traumatic or postoperative changes, where scar tissue (fibrosis) may contribute to narrowing of the spine and neural compression
- Systemic skeletal diseases, including ankylosing spondylitis, rheumatoid arthritis, and Paget’s disease, which can alter spinal anatomy and stability
- Congenital or developmental conditions, such as achondroplasia, Morquio syndrome, and neural tube defects (e.g., spina bifida and myelomeningocele), which may predispose to spinal canal stenosis
Overall, while multiple causes exist, degenerative spinal canal stenosis remains the dominant clinical form encountered in practice.
Types of Spinal Canal Stenosis: Central and Foraminal Stenosis
Spinal stenosis (spinal canal stenosis) can be classified based on the location of narrowing within the spine. This distinction is clinically important, as different types of narrowing of the spine produce different symptom patterns.
Central canal stenosis refers to the narrowing of the main spinal canal, where the spinal cord is located in the cervical region and the cauda equina in the lumbar region. Because this type of stenosis affects central neural structures, it is more likely to produce a broader range of neurological symptoms. In the cervical spine, it may lead to signs of myelopathy, including gait disturbance, balance problems, and progressive motor impairment.
Foraminal stenosis occurs when there is narrowing of the neural foramina — the openings through which individual nerve roots exit the spine. This leads to compression of a specific nerve root and most commonly presents as radiculopathy, with radiating pain, numbness, tingling, or weakness in the upper or lower extremities.
In clinical practice, mixed forms of spinal canal stenosis are common, especially in advanced degenerative disease, which can result in overlapping symptoms and variable clinical presentation.
Symptoms: How to Recognize Spinal Stenosis
Significant proportion of individuals over the age of 60 who show radiological signs of spinal canal narrowing, remain completely asymptomatic. The clinical presentation of spinal stenosis depends primarily on the level of stenosis and the degree of neural structure compression. Symptoms can range from mild, intermittent discomfort to pronounced neurological deficits that significantly affect daily functioning. In clinical practice, a clear distinction is made between cervical and lumbar spinal stenosis due to their different symptom profiles.
Cervical spinal stenosis
In cervical stenosis, symptoms arise either from compression of the nerve roots (radiculopathy) or from direct compression of the spinal cord itself (myelopathy).
Neck pain is common but is often attributed to underlying degenerative changes (cervical spondylosis) rather than stenosis per se. When nerve roots are affected, patients typically experience radiating pain into the upper extremities, accompanied by paresthesia, numbness, and weakness in the arms or hands.
More clinically significant is cervical myelopathy, which results from spinal cord compression. This condition may present with impaired fine motor skills (e.g., clumsiness of the hands), gait instability, balance disturbances, and progressive limb weakness. Cervical myelopathy is potentially progressive and, if not recognized and treated in time, may lead to irreversible neurological impairment.
In cases of significant or worsening neurological deficits, surgical decompression is often indicated in order to prevent further deterioration and preserve neurological function.
Lumbar spinal stenosis
In lumbar stenosis, symptoms predominantly affect the lower extremities. They result from compression of nerve roots within the central spinal canal (central stenosis) or at the foraminal exit zones (foraminal stenosis).
Lumbar radiculopathy
Lumbar radiculopathy occurs due to compression of a nerve root within the intervertebral foramen (foraminal stenosis). It typically presents with radiating leg pain, often accompanied by paresthesia, numbness, and possible muscle weakness.
Symptoms may be unilateral or bilateral, although bilateral involvement is common in spinal stenosis. Unlike classic disc herniation, symptoms in stenosis often involve a broader distribution along the lower limb rather than a sharply defined dermatomal pattern.
In addition to pain, patients frequently report a sensation of heaviness or weakness in the legs, particularly during walking or prolonged standing, which can significantly limit daily activities.
Spinal stenosis of lumbar region with neurogenic claudication
Neurogenic claudication is a hallmark symptom of lumbar spinal stenosis and an important clinical indicator of functional canal narrowing. It manifests as pain, heaviness, weakness, or discomfort in the legs that is triggered by walking, standing, or maintaining an upright posture.
A key feature is its strong dependence on body position. Lumbar spine extension typically exacerbates symptoms by further narrowing the spinal canal, while flexion (bending forward) relieves them by increasing available space for neural structures. As a result, patients often adopt a slightly flexed posture when walking or standing.
Clinically, this leads to a reduced walking distance (walking intolerance), with patients needing frequent stops due to symptom onset. Symptoms typically improve rapidly with sitting, forward flexion, or lying down—an important diagnostic clue distinguishing neurogenic claudication from vascular causes of leg pain.
Clinical Insight
Neck or lower back pain alone is most commonly related to degenerative spinal changes (spondylosis) rather than spinal stenosis itself. When central canal narrowing is present, it may lead to cervical myelopathy in the cervical spine or neurogenic claudication in the lumbar region.
In contrast, narrowing of the foramina (foraminal stenosis), with subsequent nerve root compression, leads to radiculopathy. Understanding this anatomical-clinical correlation is essential for accurate diagnosis and appropriate management of spinal stenosis.
Diagnosis of spinal stenosis
The diagnosis of spinal stenosis is based on a combination of clinical presentation and imaging studies. It is important to emphasize that in some patients the neurological examination may remain normal despite the presence of significant symptoms.
Clinical examination
The neurological status may be normal or may show signs of multilevel radiculopathy.
Possible findings include:
- muscle weakness
- reduced or absent tendon reflexes
- sensory disturbances
Muscle atrophy in the foot (e.g. extensor digitorum brevis) may indicate chronic nerve compression.
Imaging studies (key for confirming diagnosis)
Imaging plays a central role in confirming spinal canal stenosis, as it provides a direct visualization of anatomical narrowing and the degree of neural structure compression.
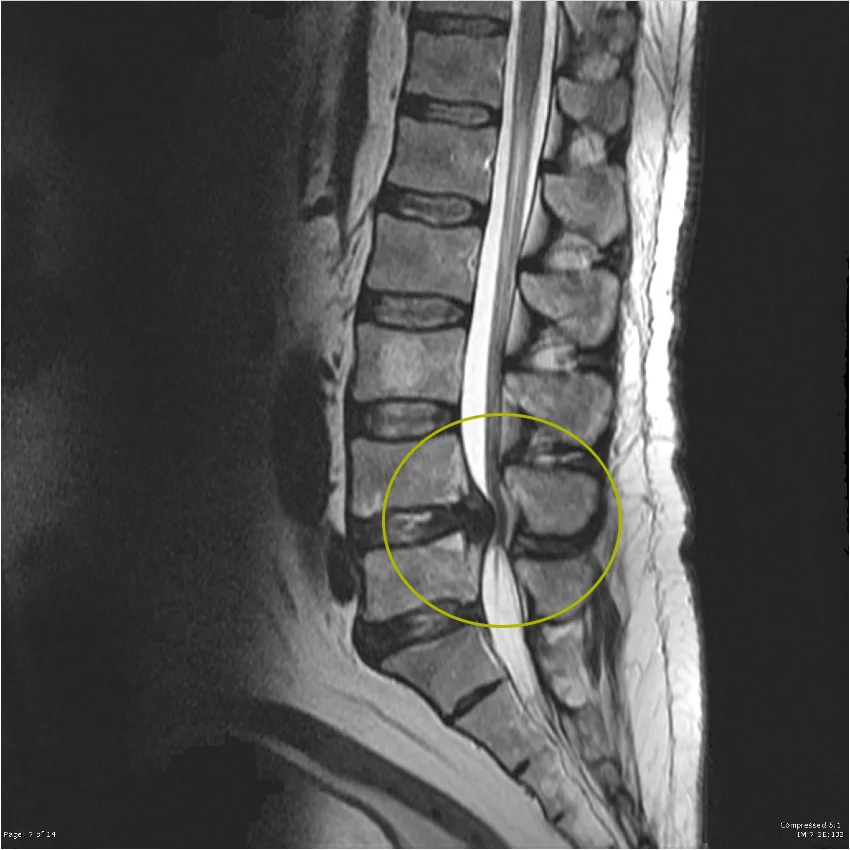
MRI (Magnetic Resonance Imaging) – gold standard
- provides detailed visualization of soft tissues, including intervertebral discs, ligaments, and neural structures
- clearly demonstrates central canal stenosis, spinal cord compression, or nerve root compression
- allows differentiation between central canal stenosis and foraminal stenosis
- non-invasive and does not involve ionizing radiation
CT (Computed Tomography)
- useful for detailed assessment of bony structures, such as osteophytes and degenerative facet joint changes
- often used as a complement to MRI or when MRI is not available or contraindicated
Clinical Insight
In everyday clinical practice, MRI is the most important diagnostic tool for evaluating spinal stenosis, as it provides the most comprehensive assessment of both the cause and extent of narrowing of the spine. It is also essential for treatment planning, particularly when surgical intervention is being considered.
Conservative (non-operative) treatment
When choosing a therapeutic approach for spinal stenosis, it is essential to assess how significantly symptoms affect daily life—particularly walking capacity, pain level, and the patient’s psychosocial well-being. Treatment is always individually tailored, as there is no single universally most effective form of conservative management.
Since this is a degenerative condition, the goal of treatment is not “cure” in the classical sense, but rather symptom reduction, preservation of function, and improvement of quality of life. The course of spinal stenosis is most often gradual. In some patients with mild to moderate symptoms, the condition may remain stable for a long period or even show spontaneous symptom improvement over time.
Physical activity and physiotherapy
The foundation of conservative management consists of exercise and physical therapy. Recommended programs typically include stretching, strengthening of the paravertebral muscles, and improving spinal stability and mobility. In selected patients, manual therapy techniques such as spinal mobilization and manipulation may also be used.
Clinical experience shows that physiotherapy-guided exercise programs and manual therapy can significantly reduce pain and improve functional capacity, particularly walking ability and performance of daily activities.
At the beginning of treatment, some patients may experience a temporary increase in pain or discomfort, which is often related to adaptation to increased activity and improved mobility.
However, in most patients, after several weeks of consistent and supervised exercise, symptoms gradually improve. Pain decreases, walking becomes more stable and longer in duration, and daily activities become easier to perform. This gradual improvement also has an important psychological effect, as patients regain confidence in their ability to move and function.
Pain medications
The effectiveness of pharmacological treatment in spinal canal stenosis is not fully established. Analgesics are used cautiously, mainly for short-term symptom relief or as supportive therapy while waiting for other treatment options, including surgery. It is important to discuss potential side effects and the limited long-term benefit of these medications.
Epidural injections
Epidural steroid injections (ESI) are a minimally invasive treatment option in which a medication (local anesthetic, with or without corticosteroids) is injected into the epidural space of the spine to reduce inflammation and pain around neural structures.
Clinical studies show that approximately 30–40% of patients experience significant short-term improvement in symptoms, mainly reduced pain and improved function, typically within the first few weeks after injection. However, no clear evidence exists that corticosteroid-containing injections are more effective than local anesthetic alone.
Therefore, in selected patients, epidural injection with a local anesthetic may be considered, with appropriate counseling that the effect is usually temporary, the procedure may need to be repeated, and possible side effects include injection-site pain, headache, dizziness, or transient neurological symptoms.
Surgical treatment
Surgical treatment for spinal stenosis is considered in a smaller proportion of patients, mainly when symptoms significantly impair quality of life or when there is no improvement despite adequate conservative management. Surgery is most often recommended in cases of severe pain, progressive neurological deficit, or worsening symptoms after 3–6 months of structured non-operative treatment.
Lumbar spinal stenosis
The primary goal of surgery is to increase the space available for neural structures and reduce compression. The most common procedure is a decompression laminectomy, in which part of the vertebral bone is removed to relieve pressure within the spinal canal.
In selected cases where spinal instability is present, spinal fusion may be added to stabilize the affected segments.
Although surgery can lead to significant pain reduction and functional improvement in many patients, outcomes are not uniform. In patients with milder symptoms, surgical intervention often does not provide a clear advantage over conservative treatment, and in a proportion of cases, some symptoms may persist even after the procedure.
Cervical spinal stenosis
In cervical stenosis, surgical treatment is most commonly considered in the presence of cervical myelopathy or progressive neurological deterioration. The goal of surgery is decompression of the spinal cord in order to prevent further neurological damage and improve function.
Depending on the pathology and anatomical findings, either an anterior or posterior surgical approach may be used. However, the fundamental principle remains the same—relief of pressure on neural structures.
Clinical Insight
The decision to proceed with surgery is always made in consultation with a neurosurgeon or spinal surgeon, with a clear explanation of expected benefits, potential risks, and realistic outcomes.
Prognosis and living with spinal stenosis
Spinal stenosis can significantly affect quality of life, particularly due to pain, reduced mobility, and limitations in walking. In some patients, symptoms remain stable over long periods, while in others there is a gradual progression over time.
As the condition evolves, it may lead to chronic pain, muscle weakness, and reduced physical endurance. In more pronounced central canal stenosis, patients may develop gait disturbances and balance problems, further limiting daily activities.
In rare but serious cases, cauda equina syndrome may occur, requiring urgent medical evaluation and treatment.
Lifestyle measures play an important role in long-term management. Regular physical activity adapted to individual capacity, smoking cessation, and maintaining a healthy body weight can all positively influence the course of spinal canal stenosis and overall functional status.
When to seek medical attention
Medical evaluation is recommended when symptoms become more pronounced or begin to significantly interfere with daily functioning.
“Red flags” (urgent symptoms):
- loss of bladder or bowel control
- sudden or severe weakness in the legs or arms
- significant numbness in the saddle area (perineal region)
Signs of progression:
- gradual worsening of pain, weakness, or walking difficulties
- decreasing walking distance without the need to stop
- worsening balance or functional ability
Conclusion: key messages for patients
Spinal stenosis is a relatively common degenerative condition of the spine, most often affecting older adults. It can cause pain, walking difficulties, and a range of neurological symptoms.
Most patients are treated conservatively, with physical therapy, activity modification, and symptom control. Surgery is reserved for selected cases with significant deterioration or neurological deficits. Because narrowing of the spine develops gradually and varies between individuals, treatment should always be tailored to the specific patient.
Frequently asked questions (FAQ)
What is spinal stenosis?
Spinal stenosis refers to a narrowing of the spine, specifically the spinal canal, which can lead to compression of the spinal cord or nerve roots. It is most commonly caused by degenerative changes and may result in pain, tingling, weakness, and walking difficulties.
Can spinal stenosis be treated without surgery?
Yes. In most cases, symptoms can be effectively managed with conservative treatment, including physical therapy, targeted exercises, and activity modification. Surgery is considered only in more severe cases or when non-operative measures fail to provide relief.
Which exercises help with spinal stenosis?
Exercises that improve flexibility, core strength, and spinal stability are most commonly recommended, ideally under the guidance of a physiotherapist. Gentle stretching and strengthening of the back and abdominal muscles can help reduce mechanical stress associated with spinal stenosis.
Is walking good or bad for spinal stenosis?
Walking is generally beneficial, but it may provoke symptoms, especially over longer distances or in an upright posture. In patients with spinal canal stenosis, symptoms often improve with rest or forward bending. Therefore, walking should be adapted to individual tolerance, with attention to pacing and posture.
Raja A, Patel P, Mesfin FB. Spinal Stenosis. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. NCBI Bookshelf: Spinal stenosis overview
Munakomi S, Foris LA, Varacallo MA. Spinal Stenosis and Neurogenic Claudication. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. NCBI Bookshelf: Neurogenic claudication and spinal stenosis
BMJ. Lumbar spinal stenosis. BMJ 2021;373:n1581. BMJ clinical review: Lumbar spinal stenosis
Margetis K, Donnally III CJ. Cervical Myelopathy. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. NCBI Bookshelf: Cervical myelopathy
Saunders LM, Sandhu HS, McBride L, et al. Degenerative Cervical Myelopathy: An Overview. Cureus. 2023;15(12):e50387. Cureus article: Degenerative cervical myelopathy
Dydyk AM, Khan MZ, Singh P. Radicular Back Pain. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. NCBI Bookshelf: Radicular back pain
Margetis K, Magnus W, Mesfin FB. Cervical Radiculopathy. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. NCBI Bookshelf: Cervical radiculopathy
BMJ Best Practice. Cervical radiculopathy. BMJ clinical decision guide
Hasvik E, Haugen AJ, Grøvle L. Symptom descriptors and patterns in lumbar radicular pain caused by disc herniation. BMJ Open. BMJ Open cohort study

















