

Heel pain is one of the most common foot problems, affecting everyone from athletes and outdoor workers to people who spend most of their day sitting. With every step, the heel absorbs up to several times your body weight, making it especially vulnerable to strain, inflammation, and overuse injuries.
Although plantar fasciitis is the condition most people associate with heel pain, the truth is that more than ten different disorders can irritate the heel — including tendon problems, nerve entrapments, bursitis, stress fractures, and even systemic inflammatory diseases.
Understanding the exact cause of heel pain is essential, because each condition requires a different treatment approach. Early recognition and proper management can prevent chronic symptoms and help restore normal, pain‑free movement.
Key Clinical Points – Heel Pain Overview
- Heel pain is one of the most common musculoskeletal complaints, affecting both active individuals and sedentary adults.
- The pain may originate from plantar fascia, tendons, nerves, fat pad, or growth plate depending on location and activity level.
- Morning heel pain is typically caused by plantar fasciitis, while posterior heel pain often indicates Achilles tendinopathy.
- Medial heel pain may suggest tarsal tunnel syndrome or posterior tibial tendon dysfunction (PTTD), whereas lateral heel pain is linked to peroneal tendonitis or sinus tarsi syndrome.
- In children aged 8–14, Sever’s disease is the most frequent cause, related to growth plate irritation during rapid development.
- Diagnosis relies on clinical examination, pain localization, and imaging when necessary to rule out fractures or nerve compression.
- Treatment focuses on load reduction, supportive footwear, stretching, and physiotherapy; most cases improve with conservative management.
- Early recognition and targeted rehabilitation help prevent chronic pain and maintain optimal foot biomechanics.
Quick Heel Anatomy
The heel is built to handle high mechanical loads, absorbing shock with every step and providing stability during standing, walking, and running. At its center sits the calcaneus, the largest bone in the foot, which forms the foundation of the rearfoot and anchors several key structures.
On the underside of the heel attaches the plantar fascia, a thick band of connective tissue that supports the arch and helps transfer force during movement. Irritation of this structure is one of the most common sources of heel pain.
At the back of the heel inserts the Achilles tendon, the strongest tendon in the body. It connects the calf muscles to the calcaneus and enables push‑off during walking and running. Just in front of it lies the retrocalcaneal bursa, a small fluid‑filled sac that reduces friction but can become inflamed with overuse.
Beneath the heel sits the fat pad, a specialized shock‑absorbing cushion that protects the calcaneus from impact. When it thins or degenerates, deep, bruise‑like pain can develop.
Along the inner and outer sides of the heel run several tendons that stabilize the foot, while the tibial nerve and its branches — including the Baxter nerve — pass close to the heel and can become compressed.
Together, these structures allow the heel to function as both a shock absorber and a rigid lever. When any component becomes irritated or overloaded, heel pain can quickly develop.
Who Gets Heel Pain Most Often?
Heel pain can affect people of all ages, but certain groups are more likely to develop it due to activity level, age‑related changes, or biomechanical factors.
Older adults often experience heel pain because the natural heel fat pad becomes thinner with age, reducing shock absorption. Up to one‑third of people over 65 report heel discomfort, which may contribute to reduced mobility and a higher risk of falls.
Physically active adults over 40 are prone to overuse injuries as tendons and soft tissues lose elasticity and recover more slowly. Even regular walking or exercise can trigger heel pain in this group.
Children and adolescents (ages 8–13) may develop heel pain from Sever’s disease, a temporary irritation of the growth plate in active kids. Pain typically appears at the back or sides of the heel, especially during sports.
Athletes of all ages—particularly runners, dancers, and soccer players—place repetitive stress on the heel, increasing the risk of plantar fasciitis, Achilles problems, and stress injuries.
People with unilateral heel pain may eventually develop symptoms in the opposite heel due to altered gait and overcompensation.
What Increases the Risk of Heel Pain?
Although heel pain can affect anyone, certain factors make the heel more vulnerable to overload, irritation, or injury. Prepoznavanje ovih rizika pomaže u prevenciji i ranom liječenju.
- Foot structure and mechanics — flat feet, high arches, or excessive pronation increase strain on the heel.
- Tight calves and poor flexibility — limited ankle mobility adds tension to the plantar fascia and Achilles tendon.
- Leg length difference — even small asymmetries can overload one heel.
- Excess body weight — higher impact forces with every step increase tissue stress.
- Repetitive or physically demanding work — long standing, lifting, jumping, or hard surfaces raise injury risk.
- Improper footwear — poor cushioning or lack of arch support leads to uneven pressure.
- Pregnancy — increased weight and fluid retention can temporarily irritate heel structures.
Identifying these factors early helps reduce strain, improve foot support, and lower the chances of developing chronic heel pain.
Conditions That Cause Pain in the Bottom of the Heel
Pain in the bottom of the heel — often described as a stabbing or bruised sensation — is one of the most common heel complaints. This area absorbs constant impact during walking, running, and standing, making it especially vulnerable to overuse and strain‑related injuries.
Here are the most frequent conditions that can cause pain beneath the heel:
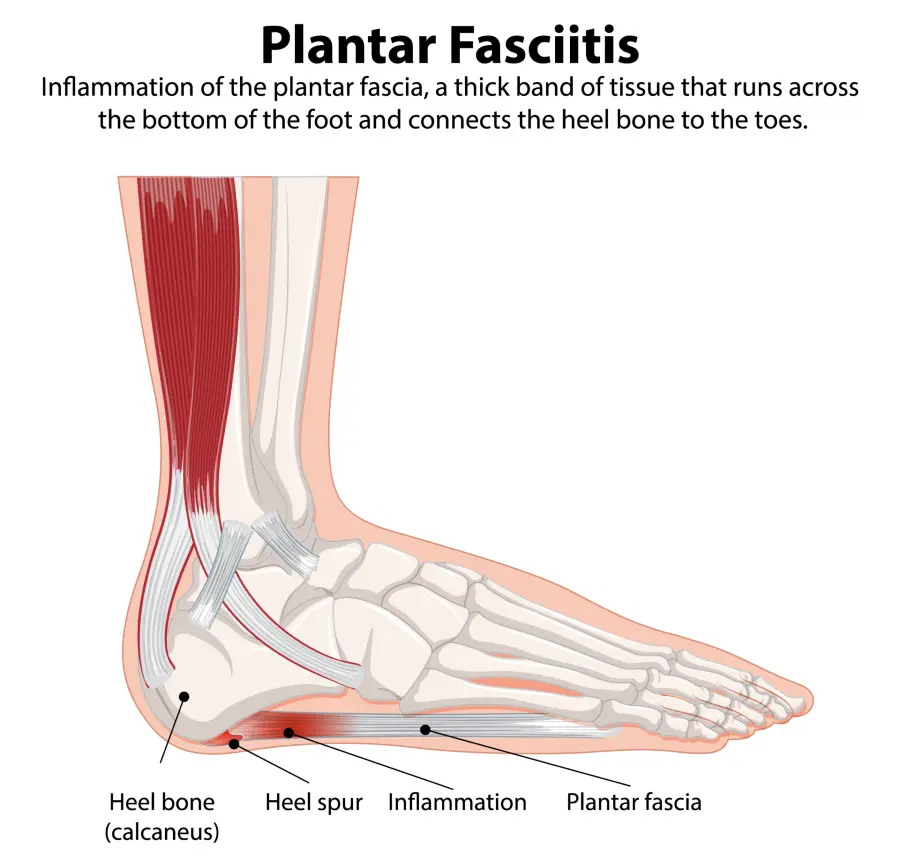
1. Plantar Fasciitis
Plantar fasciitis is the most common cause of heel pain, particularly in people who are active, overweight, or spend long hours standing. It involves degeneration and irritation of the plantar fascia — a thick band of tissue that runs along the bottom of the foot and supports the arch. Although the name ends in “‑itis,” research shows the condition is primarily degenerative, not inflammatory.
The pain is typically located on the underside of the heel, slightly toward the inner side, and is often sharp or stabbing. Symptoms are usually worst with the first steps in the morning or after prolonged rest. Pain may ease with movement but often returns after long activity. Pressing on the affected area usually triggers pinpoint tenderness. A heel spur may be visible on X‑ray, although it does not always cause symptoms.
Treatment: Conservative management is usually effective. Helpful strategies include reducing aggravating activities, stretching the calves and plantar fascia, ice massage, and using cushioned or supportive insoles. Physical therapy can improve mobility and tissue load tolerance. Night splints and shockwave therapy may help in persistent cases. Corticosteroid or PRP injections are sometimes considered when symptoms do not improve. Surgery is rarely required and reserved for chronic, treatment‑resistant cases.
Want to dive deeper into symptoms, causes, and advanced treatment options? Learn more in our full guide to Plantar Fasciitis → jointhealthguide.com/plantar-fasciitis
2. Heel Spur (Calcaneal Spur)
A heel spur is a bony outgrowth that forms at the point where the plantar fascia attaches to the heel bone. It is commonly associated with prolonged stress on the foot, especially in runners, joggers, and individuals with excess body weight. Although once believed to be caused by the plantar fascia pulling on the heel bone, newer research suggests that heel spurs develop as an adaptive response — helping distribute load across a wider surface of the heel.
Heel spurs are frequently found incidentally on X‑rays, particularly in adults over 60, and they often coexist with plantar fasciitis. Many people with heel spurs never experience symptoms, while others may develop pain in heel when walking due to irritation of surrounding soft tissues, nerve compression, or even a small stress reaction at the spur site. Genetics also play a role, making some individuals more prone to forming bony growths even under normal pressure.

Treatment: Treatment does not target the spur itself, because the spur is rarely the true source of pain. Instead, therapy focuses on the underlying condition, most commonly plantar fasciitis or heel fat pad syndrome. Supportive footwear, custom orthotics, stretching programs, and anti‑inflammatory strategies can reduce pressure and irritation in the heel area. Shock‑absorbing insoles and physical therapy may also help. Surgical removal of the spur is rarely necessary and reserved only for severe, persistent cases.
3. Fat Pad Syndrome (Heel Fat Pad Atrophy)
Heel pain caused by fat pad syndrome is typically described as a deep, aching, bruise‑like pain in the very center of the heel. Although it can resemble symptoms of plantar fasciitis, the underlying cause is different. Instead of irritation of the plantar fascia, the pain comes from inflammation, damage, or thinning (atrophy) of the heel’s natural shock‑absorbing fat pad.
Symptoms usually worsen when walking barefoot on hard surfaces, during prolonged standing, or after high‑impact activities. Because the pain is often centralized and feels “deep,” it can sometimes be difficult to distinguish fat pad syndrome from plantar fasciitis without a clinical exam.
Fat pad atrophy may develop due to aging, repetitive impact on hard surfaces, previous heel injuries, or excess body weight. Athletes who frequently jump or run on firm ground are also at higher risk.
Treatment: Management focuses on reducing pressure on the heel and protecting the weakened fat pad. Soft heel cups, silicone pads, cushioned footwear, and avoiding barefoot walking on hard floors are key strategies. Short periods of rest, ice, and general anti‑inflammatory measures can help reduce discomfort. Physical therapy may improve load distribution, while advanced options such as autologous fat grafting are considered only in chronic, severe cases.
4. Calcaneal Stress Fracture (Heel Bone Stress Fracture)
A calcaneal stress fracture is a small crack in the heel bone (calcaneus) caused by repetitive overuse, not a single traumatic event. It develops when healthy bone is exposed to repeated loading without enough time to recover, leading to micro‑damage and eventual breakdown. Common triggers include a sudden increase in training volume, starting a new exercise routine, weight gain, or wearing unsupportive footwear — especially on hard surfaces.
This injury is frequently seen in runners, military recruits, and athletes involved in high‑impact sports. Pain typically worsens with activity and improves with rest. Symptoms can mimic plantar fasciitis, but the pain is often more diffuse, sometimes accompanied by mild swelling or tenderness directly over the heel bone. Bruising is uncommon. X‑rays may appear normal in early stages, so MRI is often required for confirmation.
Treatment: Management focuses on resting the bone to allow healing. Most patients require 6–8 weeks of reduced or non‑weight‑bearing activity, depending on severity. Supportive footwear or a walking boot may be recommended to limit stress on the heel. Once pain subsides, a structured rehabilitation program helps restore strength, mobility, and gradual return to activity. Addressing contributing factors — such as training errors, footwear, or biomechanics — reduces the risk of recurrence.
Heel Pain in the Back: Conditions That Affect the Rear Part of the Heel
Pain at the back of the heel — often referred to as back of heel pain — is most commonly linked to problems involving the Achilles tendon and surrounding soft tissues. This type of pain frequently affects active individuals, runners, and people who wear stiff or poorly fitting shoes that irritate the heel. Because the Achilles tendon absorbs large forces during walking and running, even small changes in load, footwear, or training volume can trigger irritation and inflammation in this area.
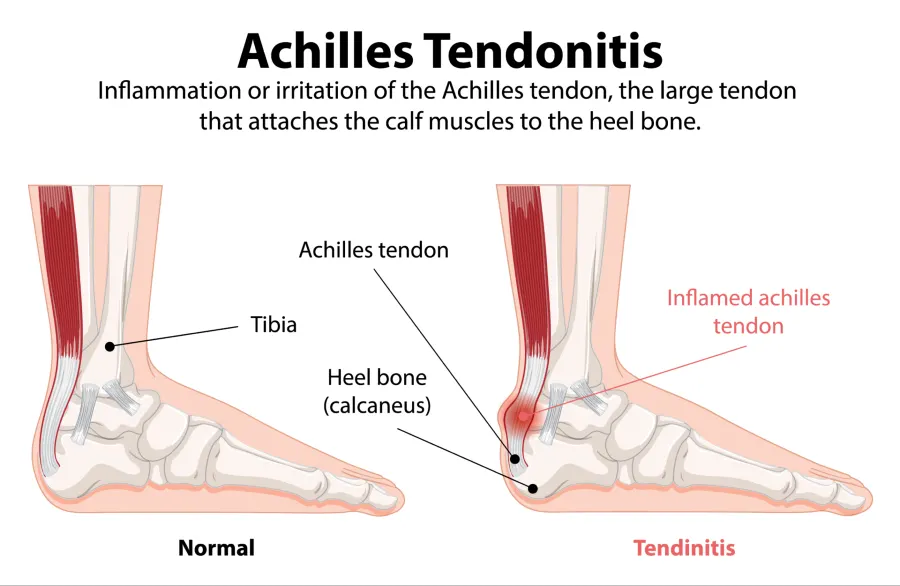
5. Achilles Tendonitis (Achilles Tendinopathy)
The Achilles tendon is the strongest tendon in the human body, connecting the calf muscles to the heel bone and playing a crucial role in walking, running, and jumping. Achilles tendinopathy — often referred to as Achilles tendonitis — occurs when the tendon becomes painful, thickened, or weakened due to overuse or gradual degeneration. Although the term “tendonitis” implies inflammation, chronic cases usually involve degenerative changes rather than active inflammation.
Achilles tendinopathy is a common cause of back of heel pain, especially in runners and individuals who perform repetitive or high‑impact activities. Additional risk factors include aging, poor or unsupportive footwear, inadequate warm‑up routines, excess body weight, and training on hard surfaces.
There are two main forms of the condition:
- Insertional Achilles tendinopathy — at the point where the tendon attaches to the heel bone
- Non‑insertional (mid‑portion) tendinopathy — affecting the middle section of the tendon
Symptoms often include dull or sharp pain at the back of the heel, morning stiffness, swelling, and tenderness along the tendon, especially during activity or when pressure is applied.
Treatment: Management is typically conservative and focuses on reducing strain on the tendon while promoting gradual healing. Effective strategies include activity modification, structured physical therapy, eccentric strengthening exercises, proper footwear or orthotic inserts, and short‑term anti‑inflammatory measures. In persistent or severe cases, advanced options such as shockwave therapy, injections, or surgery may be considered.
6. Haglund’s Deformity (Haglund’s Heel / Haglund’s Disease)
Haglund’s disease — also known as Haglund’s deformity — is a painful condition caused by a bony enlargement at the upper back part of the heel bone (calcaneus), near the insertion of the Achilles tendon. This bony prominence, often referred to as a “pump bump,” can irritate surrounding soft tissues, especially when compressed by stiff or tight shoes. Although the exact cause is not fully understood, repetitive pressure, friction, and mechanical irritation on the back of the heel play a major role in its development.
The condition is most common in middle‑aged women, particularly those who frequently wear rigid‑backed footwear. It typically presents as a firm, sometimes red or swollen lump on the back of the heel that becomes painful with direct pressure. Haglund’s deformity often coexists with Achilles tendinopathy or retrocalcaneal bursitis, making symptoms more pronounced.
Pain usually worsens when walking in shoes with hard heel counters, during uphill running, or after increased activity. In some cases, the bony prominence is clearly visible; in others, imaging may be needed to confirm the diagnosis.
Treatment: Management focuses on reducing pressure and inflammation around the affected area. Helpful strategies include wearing shoes with a soft or open heel, using heel lifts or custom orthotic insoles to reduce friction, and modifying activities that aggravate symptoms. Physical therapy can improve calf flexibility and reduce tension on the Achilles tendon. Anti‑inflammatory measures or pain‑relieving medication may help during flare‑ups. In more persistent cases, ultrasound‑guided corticosteroid injections may be considered (with caution near the Achilles tendon). Surgery to remove the bony prominence is reserved for severe or chronic cases
7. Sever’s Disease (Calcaneal Apophysitis in Children)
Sever’s disease, also known as calcaneal apophysitis, is one of the most common causes of heel pain in active children aged 8–14. It occurs when the growth plate (apophysis) at the back of the heel becomes irritated due to repetitive stress. Because this growth plate is still developing, it is more vulnerable to overload during periods of rapid growth — especially in children who participate in running and jumping sports.
The condition is frequently seen in young athletes involved in football, basketball, gymnastics, athletics, and dance. Tight calf muscles, poor footwear, and sudden increases in training intensity can further increase stress on the heel.
Typical symptoms include pain at the back of the heel, tenderness when squeezing the heel from both sides, limping after activity, and discomfort that worsens with running or jumping. Pain usually improves with rest and often affects both heels at the same time.
Treatment: Management focuses on load reduction and relieving stress on the irritated growth plate. Short‑term rest from high‑impact activities, ice after sports, and cushioned or supportive footwear are key early steps. Calf stretching exercises help reduce tension on the Achilles tendon and decrease pulling on the growth plate. Heel cups or soft orthotic inserts can improve comfort during activity. Most children recover fully within weeks to months, and the condition resolves once the growth plate closes in adolescence.
Conditions That Cause Inner and Outer Side Heel Pain
Pain on the inner (medial) or outer (lateral) side of the heel is less common than pain beneath or behind the heel, but it can still indicate several specific conditions. Because inner and outer heel pain often results from tendon irritation or nerve compression, identifying the exact location of discomfort is essential for narrowing down the cause.
Outer side (lateral) heel pain is most often linked to:
- Peroneal tendonitis
- Sinus tarsi syndrome
Inner side (medial) heel pain is commonly caused by:
- Tarsal tunnel syndrome
- Posterior tibial tendon dysfunction (PTTD)
Understanding whether the pain is located on the inside or outside of the heel helps guide the differential diagnosis and ensures each condition is explained clearly in the sections that follow.
8. Peroneal Tendonitis (Peroneal Tendinopathy)
Peroneal tendonitis — or peroneal tendinopathy — refers to irritation, overuse, or degeneration of the peroneal tendons located on the outer (lateral) side of the ankle and heel. These tendons, the peroneus longus and peroneus brevis, play a key role in stabilizing the foot and ankle during walking, running, and side‑to‑side movements. When overloaded or strained, the tendons can develop micro‑tears and become painful, leading to a common form of lateral heel pain.
Symptoms typically include aching or sharp pain behind or below the outer ankle bone, especially during walking, running, or jumping. Pain often improves with rest but returns with activity. Some people experience discomfort radiating up the outer calf or down toward the side of the foot. Swelling or a feeling of instability may also be present, particularly after repeated ankle sprains.
Peroneal tendonitis is more common in runners, individuals with high arches, and people with chronic ankle instability. Sudden increases in training volume, uneven terrain, or improper footwear can also contribute to tendon overload.
Treatment: Management focuses on reducing load on the irritated tendon during the acute phase. This includes activity modification, ice, short‑term anti‑inflammatory measures, and supportive footwear. Once pain begins to settle, a structured rehabilitation program with progressive strengthening and balance training is essential to restore tendon capacity and prevent recurrence. Physical therapy, orthotics, and taping techniques can improve foot mechanics. In persistent cases, ultrasound‑guided injections (such as PRP or hyaluronic acid) may be considered. Recovery time varies but often takes several weeks to a few months
9. Posterior Tibial Tendon Dysfunction (PTTD / Posterior Tibial Tendonitis)
Posterior tibial tendon dysfunction (PTTD) — sometimes referred to as posterior tibial tendonitis — is a condition affecting the posterior tibial tendon on the inner (medial) side of the ankle and heel. This tendon plays a crucial role in supporting the arch and stabilizing the foot during walking and running. When the tendon becomes overstressed, inflamed, or degenerates over time, it can lose its ability to maintain proper foot alignment, leading to pain and progressive flattening of the arch.
PTTD may develop due to overuse, trauma, or natural age‑related degeneration. It is more common in middle‑aged adults and individuals with flat feet, obesity, or chronic ankle instability. The condition often begins as posterior tibial tendonitis, characterized by irritation and inflammation, and can progress to partial or complete tendon dysfunction if untreated.
Symptoms typically include pain and tenderness along the inner side of the ankle or heel, which worsen with walking, running, or prolonged standing. Swelling, flattening of the foot arch, and difficulty standing on tiptoe are common in more advanced stages. In severe cases, the deformity may become visible, with the foot rolling inward and the ankle appearing unstable.
Treatment: Management depends on the stage of the condition. In early or mild cases, treatment focuses on rest, activity modification, and supportive footwear or orthotics to reduce strain on the tendon. Physical therapy and strengthening exercises for the posterior tibial muscle help restore stability and arch support. Anti‑inflammatory medications or ice can relieve pain during flare‑ups. In persistent or moderate cases, custom orthotics or ankle braces may be prescribed. For chronic or advanced stages, ultrasound‑guided injections (such as PRP) or surgical reconstruction may be considered to restore tendon function and correct foot alignment.
10. Tarsal Tunnel Syndrome
Tarsal tunnel syndrome is a condition caused by compression or irritation of the tibial nerve as it passes through the tarsal tunnel, a narrow space on the inner (medial) side of the ankle. This tunnel is formed by bone and covered by a strong connective tissue band called the flexor retinaculum. Several important structures pass through it, including the tibial nerve, tibial artery and vein, and the tendons of the tibialis posterior, flexor digitorum longus, and flexor hallucis longus muscles.
Because the tibial nerve supplies sensation to the sole and inner heel, compression within the tunnel can lead to medial heel pain and neurological symptoms. Patients often describe sharp, burning pain, tingling, or numbness that begins just above the inner ankle and radiates toward the arch, sole, or even up the calf. The discomfort typically follows the path of the tibial nerve and may worsen with foot dorsiflexion and eversion. Since symptoms can mimic plantar fasciitis or ankle joint disorders, careful clinical evaluation and sometimes nerve conduction studies are essential for accurate diagnosis.
Treatment: Management depends on the severity and underlying cause of nerve compression. Conservative approaches include rest, ice, NSAIDs, and medications for neuropathic pain such as gabapentin or pregabalin. Physical therapy, nerve‑gliding exercises, and custom orthotics can help relieve symptoms and reduce mechanical stress on the tibial nerve. In cases resistant to conservative treatment, surgical release of the flexor retinaculum may be necessary to decompress the nerve and restore normal function. Early diagnosis and intervention are key to preventing chronic nerve damage and persistent pain.
11. Sinus Tarsi Syndrome
Sinus tarsi syndrome refers to pain and discomfort on the outer (lateral) side of the heel, specifically in the small anatomical space between the ankle joint and the heel bone known as the sinus tarsi. This space contains ligaments, joint capsule tissue, fat, and nerve endings that help stabilize the subtalar joint. When these structures become irritated or inflamed, patients develop localized pain and instability in the outer ankle and heel.
The condition is more common in dancers, volleyball and basketball players, individuals with flat feet, excessive foot pronation, and those with excess body weight. Repetitive side‑to‑side movements, uneven surfaces, or previous ankle sprains can also contribute to irritation of the sinus tarsi.
The hallmark symptom is localized pain in the sinus tarsi area, especially when pressing over the outer ankle or during walking and weight‑bearing activities. Many patients describe a sensation of ankle instability, particularly on uneven ground or during quick directional changes. This instability is often due to subtle dysfunction of the subtalar joint and surrounding ligaments.
Treatment: Most cases respond well to conservative management. Anti‑inflammatory medications, cold therapy, and stable, supportive footwear help reduce irritation. A short period of immobilization may be recommended during acute flare‑ups. Supportive devices such as ankle braces or orthoses can improve joint stability and reduce excessive pronation. A structured rehabilitation program focusing on balance, proprioception, and strengthening exercises is essential for full recovery and preventing recurrence. In rare, persistent cases, advanced interventions such as corticosteroid injections or surgical debridement may be considered.
Heel Pain Symptoms Checker
Heel pain can originate from several different structures — the plantar fascia, fat pad, Achilles tendon, nerves, growth plates, or tendons on the inner or outer side of the foot. Because these conditions often share overlapping symptoms, identifying the exact location, type of pain, and activities that worsen symptoms can significantly narrow down the likely cause.
The table below provides a clear overview to help readers quickly identify the most likely cause of their heel pain.
| Symptom Pattern | Likely Condition | Key Clues |
|---|---|---|
| Pain under the heel (central) | Fat Pad Syndrome | Deep, bruise‑like pain; worse when barefoot on hard surfaces |
| Sharp pain under the heel, first steps in the morning | Plantar Fasciitis | Morning stiffness; improves with movement; tender medial heel |
| Pain at the back of the heel | Achilles Tendonitis | Worse with running/jumping; swelling or tendon thickening |
| Heel pain in active children (8–14) | Sever’s Disease | Pain with sports; tender heel squeeze; growth spurt age |
| Outer side heel pain | Peroneal Tendonitis | Pain behind/below outer ankle; worse with walking/running |
| Instability + outer heel pain | Sinus Tarsi Syndrome | Pain on uneven surfaces; ankle “giving way” |
| Inner heel/ankle pain | PTTD | Flattening arch; difficulty standing on tiptoe |
| Burning/tingling inner heel pain | Tarsal Tunnel Syndrome | Numbness; radiating pain to arch/sole; nerve‑like symptoms |
| Pain beneath heel + spur on X‑ray | Heel Spur | Often incidental; pain usually from plantar fasciitis |

Frequently Asked Questions (FAQ)
1. Heel Pain in the Morning: What’s Causing It?
Waking up with sharp heel pain during your first steps is a classic sign of plantar fasciitis. During sleep, the plantar fascia tightens. When you stand up, it suddenly stretches again, causing a sharp, stabbing pain at the bottom of the heel. The pain usually improves with movement but may return after long periods of sitting.
2. Why Does My Heel Hurt After Running?
Post‑running heel pain is most commonly linked to Achilles tendonitis or plantar fasciitis. Sudden increases in training volume, poor footwear, or tight calf muscles often contribute.
3. Why Does My Child Have Heel Pain?
Heel pain in active children aged 8–14 is often caused by Sever’s disease — irritation of the heel growth plate during growth spurts.
4. What Causes Burning or Tingling Heel Pain?
Neurological symptoms such as burning, tingling, or numbness suggest tarsal tunnel syndrome, caused by tibial nerve compression.
5. Why Does My Heel Hurt When Walking?
Pain during walking may indicate:
- Plantar fasciitis
- Fat pad syndrome
- Peroneal tendonitis
- PTTD
Location of pain is key for differentiation.
6. Why Do I Have Heel Pain on the Inner Side?
Inner (medial) heel pain is commonly caused by PTTD or tarsal tunnel syndrome.
7. Why Do I Have Heel Pain on the Outer Side?
Outer (lateral) heel pain is often due to peroneal tendonitis or sinus tarsi syndrome.
8. Can Heel Spurs Cause Pain?
Heel spurs are often not the true cause of pain. Most symptoms come from plantar fasciitis, even when a spur is visible on X‑ray.
9. When Should I See a Doctor for Heel Pain?
Seek medical evaluation if heel pain:
- persists longer than 2–3 weeks
- is severe or worsening
- includes numbness or tingling
- affects walking or daily activities
- occurs after trauma
A healthcare professional can help determine the underlying cause and appropriate management.
10. What Is the Fastest Way to Relieve Heel Pain?
General strategies include:
- reducing load
- supportive footwear
- calf stretching
- ice after activity
- avoiding barefoot walking on hard floors
But because heel pain has many causes, a proper diagnosis is important before choosing treatment.
Black JR, Hale WE. Prevalence of foot complaints in the elderly. Journal of the American Podiatric Medical Association. PubMed: Foot complaints prevalence in elderly population
Buchanan BK, Kushner D. Plantar Fasciitis. StatPearls Publishing. StatPearls: Clinical overview of plantar fasciitis
Kirkpatrick J, Yassaie O, Mirjalili SA. The plantar calcaneal spur: a review of anatomy, histology, etiology and key associations. Journal of Anatomy. PubMed: Heel spur anatomy and clinical associations
Italiano J, Bitterman AD. Diagnosis and Management of Calcaneal Stress Fractures. Radiologic Technology. PubMed: Calcaneal stress fractures diagnosis and management
Weber JM, Vidt LG, Gehl RS, Montgomery T. Calcaneal stress fractures. Clinics in Podiatric Medicine and Surgery. Clinical review: Calcaneal stress fracture pathology and treatment
Medina Pabón MA, Naqvi U. Achilles Tendinopathy. StatPearls Publishing. StatPearls: Achilles tendinopathy clinical review
Vaishya R, Agarwal AK, Azizi AT, Vijay V. Haglund’s Syndrome: A Commonly Seen Mysterious Condition. Cureus. PubMed: Haglund’s deformity and posterior heel pain
Kiel J, Kaiser K. Tarsal Tunnel Syndrome. StatPearls Publishing. StatPearls: Tarsal tunnel syndrome clinical overview
Radiopaedia. Sinus tarsi syndrome. Radiology reference: Sinus tarsi syndrome imaging and description
Silva GL et al. Antioxidant, analgesic and anti-inflammatory effects of lavender essential oil. Anais da Academia Brasileira de Ciências. PubMed: Lavender oil anti-inflammatory effects study
Fizijatar.hr. Bol u peti: 9 glavnih uzroka i kako ih liječiti. Clinical overview: Causes and treatment of heel pain


















{kind=link}