

Calcific tendonitis is a condition in which calcium deposits accumulate within the rotator cuff tendons of the shoulder. Although calcium buildup can occur in other tendons throughout the body, it most commonly affects the shoulder. These deposits are a frequent cause of chronic shoulder pain and one of the leading reasons for episodes of sudden, severe shoulder pain.
Several theories attempt to explain why calcium forms inside the rotator cuff tendons, but the exact cause of calcific tendonitis remains unclear. The condition is most often seen in adults between the ages of 30 and 60. In the majority of cases, treatment is conservative and may include non‑steroidal anti‑inflammatory medications, corticosteroid injections, physical therapy, targeted exercise programs, and shockwave therapy.
In this article, we will explain how calcium deposits develop, outline the most common symptoms, describe how calcific tendonitis is diagnosed, review the natural course of the condition, and present the most effective treatment options — along with practical advice to support recovery.
Key Clinical Points – Calcific Tendonitis of the Shoulder
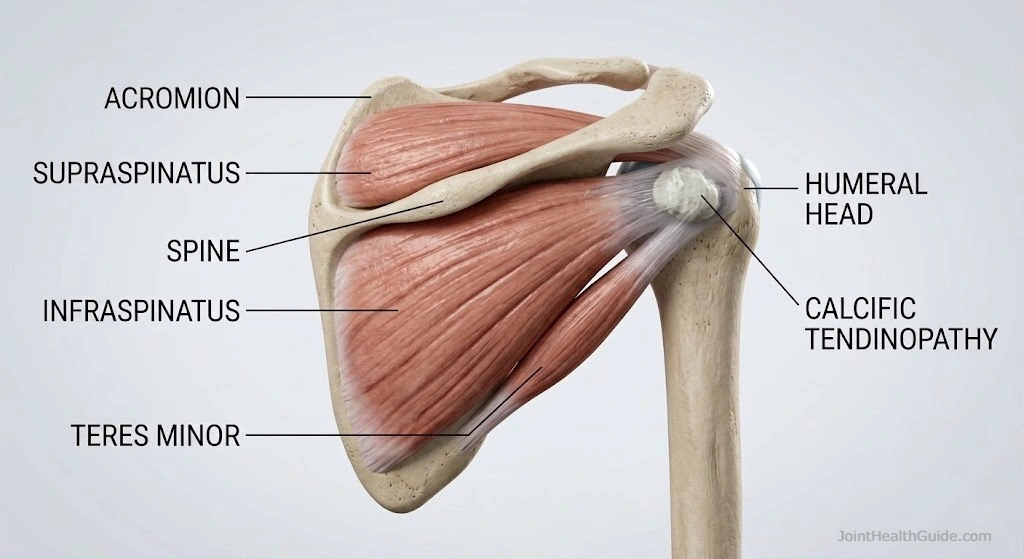
- Calcific tendonitis is caused by calcium deposition within the rotator cuff tendons, most commonly the supraspinatus.
- The condition progresses through three biological phases — precalcific, calcific (formative, resting, resorptive), and post‑calcific repair.
- Reactive calcifications are the clinically significant type and can cause sudden, severe pain during the resorptive phase.
- Not all deposits are symptomatic; calcium is found in 3–20% of asymptomatic individuals and in 10–40% of those with chronic shoulder pain.
- Diagnosis requires correlating clinical findings with imaging (X‑ray, ultrasound, MRI). Ultrasound is the best tool for determining the phase of the deposit.
- Acute severe pain is treated with rest, NSAIDs, and often ultrasound‑guided corticosteroid injection into the subacromial bursa.
- Chronic symptoms are managed with NSAIDs, physical therapy, ESWT, or ultrasound‑guided barbotage when conservative care fails.
- Surgery is rarely required and is considered only after ≥6 months of unsuccessful conservative treatment.
What Is Calcific Tendonitis?
Calcific tendonitis is a condition in which calcium deposits form inside a tendon, most commonly within the rotator cuff tendons of the shoulder. These deposits can irritate the surrounding tissues, trigger inflammation, and lead to episodes of both chronic and acute shoulder pain.
Although calcium buildup can occur in other tendons throughout the body, the shoulder is by far the most frequently affected site — which is why the term calcific tendonitis shoulder is so commonly used in clinical practice.
The terms calcific tendonitis and calcific tendinopathy are often used interchangeably. In everyday clinical language, calcific tendonitis typically refers to the painful, inflammatory phase, while calcific tendinopathy is a broader term that includes all stages of the condition, from the formation of the deposit to its resorption.
Where Does Calcific Tendonitis Most Commonly Occur?
Calcium deposits can develop in different parts of the rotator cuff, but some tendons are affected far more frequently than others. Clinical studies show the following distribution:
- Supraspinatus tendon — 63% The most common site due to mechanical stress and relatively poor vascular supply.
- Supraspinatus and subscapularis tendons — 20% Combined involvement often indicates larger or more complex calcium deposits.
- Subscapularis tendon — 3% Less common, but can cause significant pain during internal rotation.
- Infraspinatus tendon — 7% Deposits here may mimic posterior impingement symptoms.
- Subacromial bursa — 7% Calcium can migrate into the bursa during the resorptive phase, often triggering sudden, intense shoulder pain.
Who Is Most Affected by Calcific Tendonitis?
Calcific tendonitis or calcific tendinopathy most commonly affects adults between 30 and 60 years of age, and research consistently shows that women are slightly more affected than men. Despite extensive study, there is no clear link between the development of calcium deposits and factors such as physical workload, use of the dominant arm, the presence of other medical conditions, or specific occupations.
These findings suggest that calcific tendonitis develops independently of external mechanical stress and is more likely influenced by individual biological factors.
How and Why Does Calcific Tendonitis Develop?
There are two main types of calcium deposits based on their underlying mechanism, and both can occur within the rotator cuff region. Although they share a similar final appearance on imaging, they develop through completely different biological pathways, which is why their symptoms, progression, and treatment response can vary significantly.
The two primary forms are:
- Degenerative (dystrophic) calcifications
- Reactive calcific tendonitis
Degenerative (Dystrophic) Calcifications
Degenerative, or dystrophic, calcifications develop as a consequence of age‑related tendon degeneration, most commonly at the tendon’s attachment to bone — the enthesis. With aging, the tendon undergoes structural changes:
- the quality of collagen fibers decreases
- water content within the tendon increases
- the tendon becomes mechanically weaker
- small micro‑tears gradually accumulate
During the incomplete healing of these micro‑tears — a process that becomes less efficient with age — calcium may be deposited at the site of injury. This type of calcification is a slow, chronic process that progresses over time.
On imaging (X‑ray or ultrasound), dystrophic calcifications often appear as bony spurs, enthesophytes, or small areas of calcification at the tendon insertion. They are frequently found incidentally in the foot, hip, knee, elbow, and other joints, and usually do not cause symptoms.
Reactive Calcific Tendonopathy
Reactive calcifications are the classic form associated with calcific tendonitis of the shoulder and are the type most clinicians refer to when discussing calcific tendinopathy. The exact cause is not fully understood, but several theories share a common mechanism:
Tenocytes (tendon cells) transform into chondrocytes (cartilage‑like cells).
Once this transformation occurs, the altered cells begin depositing calcium salts within the rotator cuff tendons. Unlike dystrophic calcifications, reactive deposits do not form at the tendon insertion, but rather within the tendon substance itself.
These deposits can remain silent for months or years, but during the resorptive phase, they may trigger intense inflammation and severe shoulder pain.
Phases of Calcific Tendonopathy
Before a calcium deposit becomes visible on imaging or causes shoulder pain, it passes through a predictable biological cycle. These stages explain why some patients have no symptoms for months, while others suddenly develop severe, disabling pain. Understanding these phases is essential for interpreting symptoms, choosing the right treatment, and predicting recovery.
The development of a calcium deposit in the shoulder is traditionally divided into three major phases:
- Pre‑calcific phase
- Calcific phase (with three sub‑phases)
- Post‑calcific (repair) phase
Each phase has distinct cellular processes, imaging characteristics, and clinical presentations.
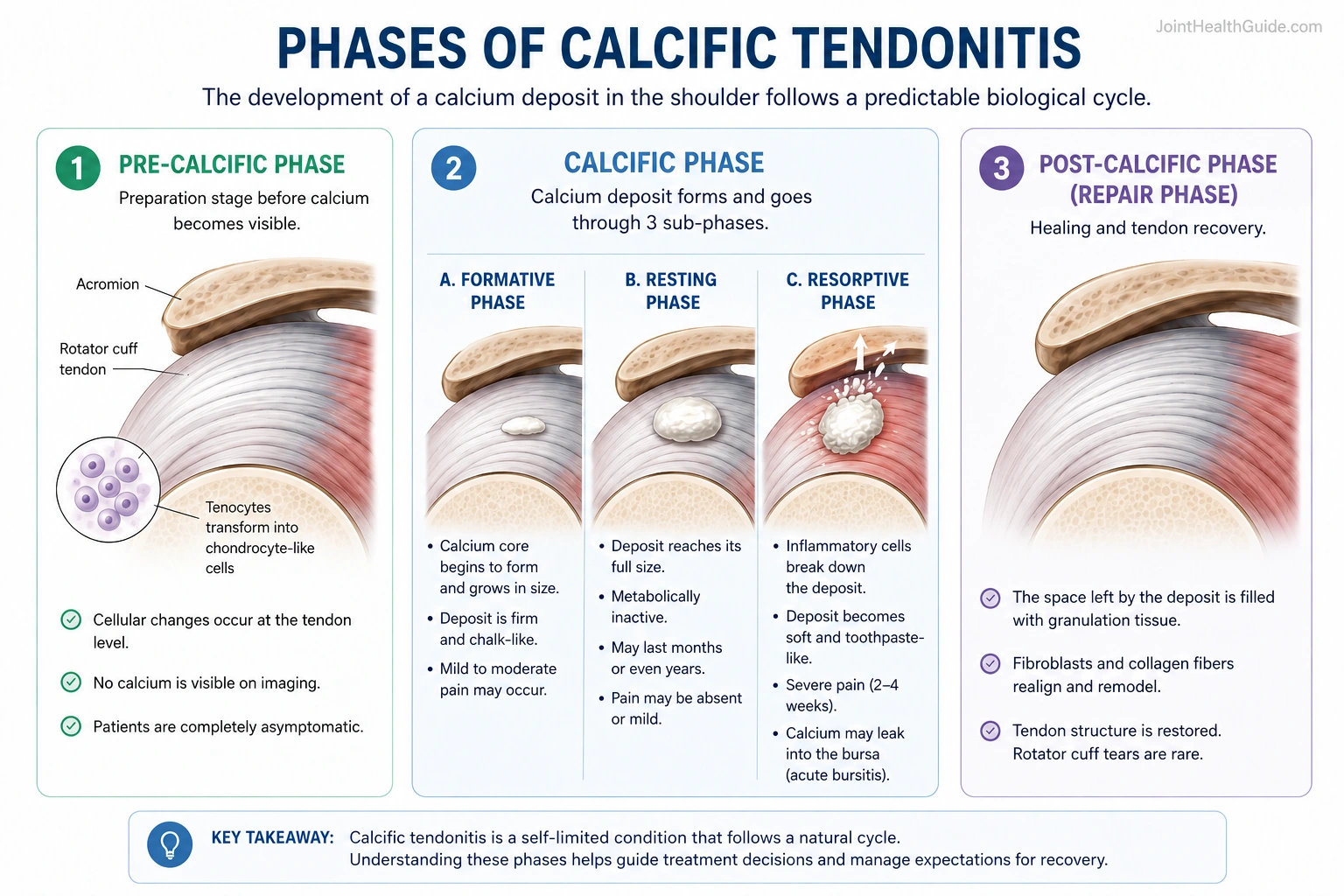
1. Pre‑Calcific Phase
The pre‑calcific phase represents the “preparation stage” for future calcium formation. Changes occur at the cellular level, long before any symptoms appear.
At a specific area within the tendon, tenocytes begin to transform into chondrocyte‑like cells (cells resembling cartilage). This cellular shift creates an environment that allows calcium to accumulate later.
Patients in this phase are completely asymptomatic, and the process is usually discovered only retrospectively.
2. Calcific Phase
The calcific phase is the central stage of the condition and is traditionally described using the model proposed by Uhthoff and colleagues, one of the most widely accepted explanations for how reactive calcific tendonitis develops. According to this model, the calcium deposit progresses through three distinct sub‑phases, each with its own biological activity and clinical presentation. These stages help explain why some patients experience mild discomfort while others suddenly develop severe, debilitating shoulder pain.
The three sub‑phases are:
- Formative phase — tenocytes transform into chondrocytes and begin producing calcium
- Resting phase — the deposit remains stable and often causes minimal symptoms
- Resorptive phase — the body attempts to break down the deposit, triggering acute inflammation and severe pain
Formative Phase
Under the influence of transformed chondrocytes, a central “core” of calcification begins to form. Calcium salts gradually accumulate around this core, creating a deposit that may range from a few millimeters to 2–3 centimeters in size.
Some patients may experience mild or moderate shoulder pain, either at rest or during specific movements. In this stage, the deposit is firm and chalk‑like, similar to school chalk.
Resting Phase
Once the deposit reaches its full size, it becomes metabolically inactive and enters a prolonged resting period. This phase can last months or even years.
Symptoms vary: some patients remain pain‑free, while others experience discomfort due to mechanical irritation caused by the size and location of the deposit.
Resorptive Phase
This is the most dramatic and clinically significant stage. The body initiates an inflammatory response: macrophages and multinucleated giant cells surround the deposit and begin breaking it down.
Key features of this phase:
- intense inflammation
- severe, often unbearable shoulder pain
- possible leakage of calcium into the subacromial bursa, causing acute calcific bursitis
- the deposit becomes soft and toothpaste‑like in consistency
The severe pain typically lasts 2–4 weeks, after which symptoms gradually improve as the repair process begins. The deposit may be partially or completely resorbed, depending on its size and structure.
3. Post‑Calcific Phase (Repair Phase)
The repair phase begins as soon as the resorptive phase starts. The space left behind by the dissolved calcium deposit is filled with granulation tissue, which gradually matures into organized scar tissue.
Fibroblasts and collagen fibers realign and remodel, restoring the tendon’s normal structure. In most cases, the tendon heals fully, and rotator cuff tears are rare in association with calcific tendonitis. This supports the idea that the primary mechanism behind calcific tendonitis is not tendon degeneration, but a distinct biological process.
Symptoms of Calcific Tendonitis
Calcific tendonitis can present with acute or chronic symptoms, depending on the phase of the calcium deposit. Importantly, not all patients experience pain — many people have a calcium deposit in the shoulder without ever knowing it.
Population studies show:
- calcium deposits are found in 3–20% of people without shoulder pain
- they appear in 10–40% of individuals with chronic shoulder pain
This means that the presence of a deposit does not automatically indicate that the shoulder pain comes from calcific tendonitis.
Acute Calcific Tendonitis
Acute symptoms are characteristic of the resorptive phase, when the body actively breaks down the calcium deposit.
Patients typically present with:
- sudden onset of severe shoulder pain, often overnight
- no history of trauma or overuse
- intense muscle spasm around the shoulder
- very limited active and passive movement due to pain and guarding
- diffuse pain that cannot be localized to a single point
Clinically, this episode can resemble frozen shoulder, but the underlying mechanism is different. During this phase, inflammatory cells accumulate around the deposit and begin dissolving it. This increases intratendinous pressure, releases inflammatory mediators, and triggers extreme pain.
The acute painful phase usually lasts 2–4 weeks, after which symptoms gradually improve as the repair process begins.
Chronic Calcific Tendinopathy
Chronic symptoms are associated with the formative, resting, or post‑calcific (repair) phases.
Typical features include:
- mild to moderate shoulder pain
- pain not always linked to movement
- possible night pain
- mechanical irritation due to the size or location of the deposit
- symptoms during overhead activities or reaching behind the back
Larger deposits — especially those greater than 6 mm — are more likely to cause symptoms. A bulky deposit can protrude into the subacromial space, reducing the room available for the rotator cuff and leading to subacromial impingement‑like symptoms.
Patients often describe:
- intermittent pain episodes lasting several weeks
- discomfort during specific movements
- difficulty lifting the arm overhead
Chronic calcific tendonitis can be difficult to distinguish from rotator cuff tendinopathy, partial‑thickness tears, or subacromial impingement, as symptoms may overlap.
If you want a clear, visual way to understand what might be causing your shoulder pain, explore our step‑by‑step diagnostic chart: Shoulder Pain Diagnosis Chart.
Although calcific tendonitis is often discussed as a single condition, symptoms can vary dramatically depending on the biological phase of the calcium deposit. Acute episodes are typically driven by active inflammation and calcium resorption, while chronic symptoms are more related to mechanical irritation and tendon dysfunction. The table below summarizes the key clinical differences between acute and chronic calcific tendonitis.
| Feature | Acute Calcific Tendonitis | Chronic Calcific Tendinopathy |
|---|---|---|
| Disease Phase | Typically occurs during the resorptive phase when the body actively breaks down the calcium deposit | Usually associated with the formative, resting, or post-calcific repair phases |
| Pain Onset | Sudden and severe, often developing overnight | Gradual or intermittent onset over time |
| Pain Intensity | Extreme pain with marked inflammatory reaction | Mild to moderate pain, usually less intense |
| Movement Restriction | Severe limitation of both active and passive shoulder movement due to pain and guarding | Movement usually preserved but painful during specific activities |
| Pain Localization | Diffuse pain that is difficult to localize | More activity-related discomfort, often linked to overhead motion |
| Night Pain | Very common and often severe | Possible but usually less intense |
| Mechanical Symptoms | Usually dominated by inflammation rather than mechanical irritation | Mechanical irritation from large deposits may cause impingement-like symptoms |
| Typical Trigger | Often occurs without trauma or overuse | Symptoms worsen during overhead activities or reaching behind the back |
| Duration | Acute painful phase usually lasts 2–4 weeks | Symptoms may persist intermittently for months or longer |
| Associated Findings | Inflammatory cell infiltration, increased tendon pressure, intense muscle spasm | Large deposits (>6 mm) may narrow the subacromial space and contribute to impingement |
Diagnosis of Calcific Tendonitis
Diagnosing calcific tendonitis shoulder involves a combination of clinical examination and imaging. Many patients present with shoulder pain, but only imaging can confirm the presence, size, and stage of the calcium deposit. Importantly, not all deposits cause symptoms, so diagnosis must always correlate clinical findings with imaging results.
Clinical Examination
During the physical exam, patients with symptomatic calcific tendonitis typically experience:
- pain during shoulder movement, especially in the so‑called painful arc
- the painful arc usually appears between 70° and 110° of abduction, likely due to impingement between the calcium deposit and the coracoacromial ligament or acromion
- preserved strength, although movement may be limited due to pain
- a localized point of maximal tenderness over the affected tendon
Clinical findings alone cannot confirm calcific tendonitis, so imaging is essential for accurate diagnosis.
Imaging Methods
To identify a calcium deposit and assess its characteristics, clinicians use:
- Shoulder X‑ray
- Ultrasound
- MRI (less commonly)
Each modality provides different information and has specific advantages.
Shoulder X‑ray
X‑ray is usually the first imaging test performed in patients with shoulder pain, regardless of symptom duration. It helps determine:
- size of the calcium deposit
- approximate location
- morphology (well‑defined and dense vs. fluffy and poorly defined)
Calcium deposits typically appear 1–2 cm from the tendon insertion. Images should ideally be taken in neutral, external rotation, and internal rotation to better localize the deposit.
During the resorptive phase, the deposit becomes:
- irregular
- less dense
- poorly defined
- sometimes barely visible on X‑ray
This is a major limitation of X‑ray, since the most painful phase often corresponds to the least visible deposit.
Ultrasound
Ultrasound is a fast, safe, inexpensive, and highly informative imaging method. It is the best tool for evaluating:
- exact location of the deposit
- size
- stage (formative, resting, or resorptive)
- associated conditions such as calcific bursitis or rotator cuff tears
Based on ultrasound appearance, deposits are classified into three types:
- Type 1 — hard, well‑defined, bone‑like; corresponds to formative or resting phase
- Type 2 — softer edges, less defined; early resorptive phase
- Type 3 — very poorly defined, cloudy; active resorptive phase


Ultrasound can also show increased blood flow around the deposit during the resorptive phase, indicating intense inflammation.
Determining the phase is crucial for planning treatment and avoiding unnecessary procedures. For example, during the acute phase, the best option is often a bursal corticosteroid injection under ultrasound guidance.
MRI
MRI is an excellent method for evaluating soft tissues, but it is not the first choice for detecting calcific tendonitis. Calcium deposits may be difficult to visualize clearly on MRI.
However, MRI is useful for identifying:
- rotator cuff tears
- bursitis
- bone marrow edema in cases where calcium migrates into the bone
MRI is typically reserved for cases where symptoms suggest additional shoulder pathology beyond calcific tendonitis.
Clinical Insight
Diagnosing calcific tendonitis requires correlating clinical findings with imaging. X‑ray helps identify the size and density of the deposit, ultrasound is the most accurate tool for determining its exact location and phase, and MRI is reserved for detecting associated shoulder pathology. Understanding the stage of the deposit is essential for choosing the right treatment and avoiding unnecessary interventions.
Treatment of Calcific Tendonitis
Treatment for calcific tendonitis shoulder depends on whether symptoms are acute or chronic, and on the phase of the calcium deposit. As mentioned earlier, the presence of a calcium deposit does not automatically require treatment — many deposits are asymptomatic and discovered incidentally.
Treatment is indicated only when symptoms are present, and the therapeutic approach aligns closely with the biological phase of the deposit:
- acute, severe pain → resorptive phase
- chronic, intermittent pain → formative or resting phase
The goal of treatment is not to dissolve or “break” the calcium deposit directly, but to reduce pain, control inflammation, and restore shoulder function.
Acute Phase (Severe Sudden Pain) Treatment
Patients in the acute phase typically present with sudden, intense shoulder pain, often without trauma. Movement is extremely painful, both actively and passively. This corresponds to the resorptive phase, where inflammation and intratendinous pressure are high, and calcium may leak into the bursa, causing acute calcific bursitis.
The primary goal is to calm inflammation:
- Rest — avoid painful movements but no immobilization or slings
- Analgesic and anti‑inflammatory medication
- Corticosteroid injection into the subacromial bursa (preferably ultrasound‑guided)
Rest
Rest prevents further irritation of inflamed tissue. Full immobilization is not recommended, as it may worsen stiffness.
Medication (NSAIDs)
Family physicians or physiatrists typically prescribe NSAIDs such as ibuprofen, ketoprofen, naproxen, or diclofenac for 7–14 days in anti‑inflammatory doses.
Corticosteroid Injection for Calcific Tendonitis
If pain remains severe despite medication — or if symptoms are extreme from the start — a bursal corticosteroid injection combined with a local anesthetic is the most effective option. Effects usually begin within 2–4 days, often providing dramatic relief. Ultrasound guidance improves accuracy and reduces side effects.
Chronic Phase
The chronic phase includes all stages except the resorptive phase. Symptoms may be persistent or episodic throughout the year. Pain arises from:
- calcium deposition during the formative phase
- mechanical impingement between the deposit and the acromion or coracoacromial ligament
Treatment focuses on pain reduction and functional improvement:
- Analgesics / NSAIDs
- Physical therapy
- Shockwave therapy (ESWT)
- Ultrasound‑guided lavage (barbotage)
- Surgery (rarely needed)
Medication
NSAIDs may be used intermittently for pain control, but long‑term use should be cautious due to gastrointestinal, renal, and cardiovascular risks.
Physical Therapy
Physical therapy includes:
- range‑of‑motion exercises
- strengthening of the scapular stabilizers and rotator cuff
- modalities such as ultrasound, LASER, HILT, TENS, or interferential currents
Shockwave Therapy (ESWT)

Shockwave therapy is a non‑invasive treatment that delivers high‑energy acoustic waves to the affected tendon. It is typically recommended when pain persists despite medication and physical therapy. The waves stimulate biological processes that help reduce pain and promote the breakdown and resorption of the calcium deposit.
Although the exact mechanism is not fully understood, ESWT appears to combine a mechanical effect on the calcification with a controlled inflammatory response that enhances healing. Most patients tolerate the treatment well, and any temporary soreness or redness usually resolves quickly. For many individuals with chronic calcific tendonitis, ESWT offers meaningful symptom relief without the need for invasive procedures.
Ultrasound‑Guided Barbotage (Lavage)
Barbotage is a minimally invasive procedure designed to remove the calcium deposit directly from the tendon using one or two needles under ultrasound guidance. It is typically considered when symptoms persist despite medication, physical therapy, or ESWT, and is especially effective when the deposit is in a semi‑liquid (Type II or Type III) state during the resorptive phase. In these cases, the calcium is softer, intratendinous pressure is high, and aspiration becomes significantly easier.
The procedure is performed in an outpatient setting under local anesthesia. Ultrasound ensures precise needle placement and allows the clinician to monitor the consistency of the deposit in real time. When the calcium is soft, it can often be aspirated directly; when it is firm, saline is injected to break it down before removal. After the procedure, a corticosteroid is typically injected into the subacromial bursa to reduce inflammation and prevent excessive post‑procedural pain.
Procedure steps:
- Local anesthetic is injected into the soft tissues and subacromial bursa
- One or two needles are inserted into the calcium deposit under ultrasound guidance
- If the deposit is semi‑liquid (Type II), it is aspirated directly into a syringe
- If the deposit is firm (Type I), saline is injected to soften and dissolve the material before aspiration
- A corticosteroid injection is administered into the bursa at the end of the procedure to minimize inflammation
Barbotage is most successful when the deposit is soft and under pressure, which is why timing matters. In hard, chalk‑like deposits (Type I), the results are less predictable and may not outperform corticosteroid injection alone. Still, for many patients with persistent symptoms, barbotage offers a meaningful reduction in pain and faster return of shoulder function without the need for surgery.
Surgery
Surgery is considered when:
- symptoms persist despite 6 months of conservative treatment
- pain continues after lavage
- the deposit is large and mechanically problematic
Surgical removal is typically performed arthroscopically, using small incisions and a camera to access and remove the deposit.
FAQ – Calcific Tendonitis of the Shoulder
Is frozen shoulder the same as calcific tendonitis?
No. Frozen shoulder involves inflammation, thickening, and tightening of the joint capsule, leading to pain and significant stiffness. Calcific tendonitis, on the other hand, is caused by calcium deposits within the rotator cuff tendons. These two conditions can sometimes appear similar, especially during the acute resorptive phase of calcific tendonitis, when pain and guarding are so intense that the shoulder becomes almost immobile. Ultrasound is the best way to distinguish them: a calcium deposit (and sometimes calcific bursitis) is clearly visible in calcific tendonitis. Pain relief after a subacromial corticosteroid injection is also typical for calcific tendonitis but not for frozen shoulder.
Does every calcium deposit in the shoulder cause pain?
No. Many calcium deposits are completely asymptomatic and discovered incidentally during imaging for unrelated reasons. Up to 20% of people without shoulder pain have a calcium deposit. Pain occurs only when the deposit becomes inflamed, mechanically irritating, or enters the resorptive phase.
Does the calcium deposit need to disappear for the pain to go away?
No. After the acute phase resolves, the deposit often remains visible on imaging. It is usually smaller but rarely disappears completely, especially if it was large. Most patients become pain‑free even though the deposit is still present.
Which calcium deposits are painful?
Severe, sudden pain occurs when the deposit enters the resorptive phase, where inflammation and intratendinous pressure rise sharply. Chronic pain is more closely related to the size of the deposit — those larger than 6 mm are more likely to cause symptoms.
I have a calcium deposit in my shoulder. What can I expect?
Several scenarios are possible:
- You may have no symptoms at all. Pain may or may not appear in the future.
- You may experience acute, severe pain lasting 2–4 weeks, typical of the resorptive phase. Pain improves spontaneously or with NSAIDs or a corticosteroid injection.
- You may have chronic mild or moderate pain, either constant or episodic. In this case, treatment such as physical therapy, ESWT, or barbotage may be needed.
Calcium deposits form slowly over months or years, and they also resolve slowly — sometimes over 5–10 years.
Does a calcium deposit damage the tendon?
Tendon tears at the site of the deposit are rare. After the resorptive phase, the tendon usually heals completely and regains normal structure and mechanical properties.
Do corticosteroid injections interfere with the natural resorption process?
No. Although corticosteroids reduce inflammation, they do not disrupt the natural breakdown of the deposit or the tendon’s remodeling process.
How long does calcific tendonitis last?
The acute painful phase typically lasts 2–4 weeks, but the entire biological cycle of the deposit — from formation to resorption — may span months to years. Chronic symptoms often fluctuate over time.
Can calcific tendonitis come back?
Recurrence is possible but not common. Once a deposit fully resorbs and the tendon remodels, most patients do not experience a new deposit in the same location.
What natural treatments can help with calcific tendonitis?
Several natural approaches may help reduce symptoms:
- Cold therapy during the acute phase to reduce inflammation
- Heat therapy during chronic phases to improve circulation
- Massage of the neck and scapular muscles to reduce tension
- Herbal anti‑inflammatory supplements (turmeric, ginger, devil’s claw, bromelain), though scientific evidence is limited
- Rest during acute inflammation
- Regular exercise to improve mobility and strengthen the shoulder girdle
Always consult a healthcare professional before starting supplements or new treatments.
Is calcific tendonitis serious?
Calcific tendonitis can be extremely painful, especially during the resorptive phase, but it is not considered a dangerous condition. The inflammation can be intense, movement can be severely limited, and the pain may mimic more serious shoulder disorders — but the condition is self‑limiting and the tendon typically heals fully. Most patients recover with conservative treatment, and long‑term complications such as tendon rupture are rare. If symptoms persist or worsen, it is important to consult a healthcare professional for proper evaluation and management.
Can calcific tendonitis be prevented?
There is no proven way to fully prevent calcific tendonitis because the exact cause of calcium deposition is still not fully understood. It does not appear to be related to overuse, occupation, or trauma. However, maintaining good shoulder mobility, balanced rotator cuff strength, and healthy biomechanics may help reduce irritation around the tendon and lower the likelihood of chronic symptoms. Early evaluation of shoulder pain can also help identify other conditions that may mimic or coexist with calcific tendonitis.
Chianca V, Albano D, Messina C, Midiri F, Mauri G, Aliprandi A, Catapano M, Pescatori LC, Monaco CG, Gitto S, Pisani Mainini A, Corazza A, Rapisarda S, Pozzi G, Barile A, Masciocchi C, Sconfienza LM. Rotator cuff calcific tendinopathy: from diagnosis to treatment. Acta Biomed. Evidence-based review: Diagnosis and treatment of rotator cuff calcific tendinopathy
Harvie P, Pollard TC, Carr AJ. Calcific tendinitis: natural history and association with endocrine disorders. J Shoulder Elbow Surg. Clinical study: Natural history and endocrine associations of calcific tendinitis
Mouzopoulos G, Stamatakos M, Mouzopoulos D, Tzurbakis M. Extracorporeal shock wave treatment for shoulder calcific tendonitis: a systematic review. Skeletal Radiol. Systematic review: Shock wave therapy for calcific shoulder tendonitis
Chiou HJ, Chou YH, Wu JJ, Huang TF, Ma HL, Hsu CC, Chang CY. The role of high-resolution ultrasonography in management of calcific tendonitis of the rotator cuff. Ultrasound Med Biol. Ultrasound imaging guide: Management of rotator cuff calcific tendonitis
Uhthoff HK, Loehr JW. Calcific Tendinopathy of the Rotator Cuff: Pathogenesis, Diagnosis, and Management. J Am Acad Orthop Surg. Classic orthopedic review: Pathogenesis, diagnosis, and management of calcific tendinopathy

















