
Hip pain during training is often dismissed as a minor issue. However, it may sometimes indicate a hip stress fracture — a potentially serious overuse injury that requires early recognition.
The most clinically important subtype is the femoral neck stress fracture, which affects the load-bearing region of the hip. Although relatively uncommon, delayed diagnosis can lead to fracture displacement and complications such as avascular necrosis, significantly impacting long-term outcomes.
One of the main challenges is the subtle presentation. Symptoms are often gradual and non-specific, making early diagnosis difficult in clinical and athletic settings. If left untreated, a hip stress fracture can end an athlete’s season — or career.
This article provides a clinically grounded overview of hip stress fractures, with a focus on femoral neck stress fractures, including their mechanisms, risk factors, diagnosis, and management.
Key Clinical Points – Hip Stress Fracture
- Hip stress fractures represent a spectrum of bone stress injury, ranging from early stress reaction to complete femoral neck fracture.
- The most common presentation is exercise-related groin pain, often subtle in early stages and easily misdiagnosed.
- High-risk groups include long-distance runners, marathon athletes, military recruits, and individuals with low energy availability.
- Femoral neck stress fractures are clinically important due to the risk of displacement, avascular necrosis, and long-term hip damage.
- MRI is the gold standard for early diagnosis, as plain radiographs are frequently normal in early disease.
- Treatment is classification-driven: compression-sided injuries are often managed conservatively, while tension-sided and displaced fractures usually require surgery.
- Early diagnosis is critical and significantly improves outcomes, while delayed diagnosis increases complication risk exponentially.
What is a Hip Stress Fracture?
A hip stress fracture is part of a broader group of conditions known as bone stress injuries, which represent a continuum of bone overload rather than a single sudden event. Instead of breaking from one traumatic impact, the bone gradually accumulates microscopic damage when repetitive loading exceeds its natural ability to repair.
This process typically follows a predictable spectrum. It begins with periostitis, an early inflammatory response of the bone surface to mechanical stress. If loading continues without adequate recovery, this progresses into a stress reaction, where bone marrow edema and microstructural changes develop, even though a true fracture line may not yet be visible. The final stage is a stress fracture, where microscopic cracks coalesce into a visible structural break in the bone.
The hip is particularly vulnerable to this process because it is a high-load weight-bearing joint, exposed to repetitive forces during walking, running, jumping, and directional changes. Among all regions of the hip, the femoral neck is biomechanically critical. It acts as a narrow bridge transferring load from the femoral head to the shaft, meaning it is subjected to significant bending forces with every step.
In simple terms, a hip stress fracture can be understood as a “bone fatigue failure from repetitive loading”—similar to bending a paperclip back and forth until it eventually breaks. The key difference is that in bone, this failure develops gradually over weeks to months, often with subtle early symptoms that are easy to overlook.
Who Gets It? Epidemiology & Risk Groups
Hip stress fractures are relatively uncommon but clinically important injuries within sports medicine, accounting for approximately 3% of all stress fractures in athletes. Although the overall incidence is low, the consequences can be significant, particularly when diagnosis is delayed and the injury progresses to displacement.
The condition is most frequently seen in high-impact, repetitive loading sports, especially:
- long-distance running
- marathon running
- military training and basic recruit programs
- endurance-based athletic disciplines with rapid load progression
Among these, running is by far the dominant mechanism, as the femoral neck is exposed to repetitive cyclical loading over thousands of steps. Military recruits represent a particularly well-described risk group due to abrupt increases in training intensity combined with load-bearing activities.
From a demographic standpoint, hip stress fractures tend to affect:
- younger, physically active individuals
- female athletes (higher incidence overall)
- athletes undergoing rapid changes in training load or intensity
The female predominance is strongly associated with the interaction between energy availability and bone health. Low energy availability, menstrual dysfunction, and reduced bone mineral density—collectively described as relative energy deficiency in sport (RED-S)—significantly reduce bone tolerance to repetitive loading.
A key and often underestimated contributor is training load error. The most common scenarios include sudden increases in running volume, insufficient recovery periods, and rapid progression in intensity or terrain difficulty. Importantly, hip stress fractures are rarely caused by a single factor; instead, they arise from the combination of mechanical overload and reduced biological capacity for bone repair.
Summary
Hip stress fractures occur at the intersection of load, recovery, and bone resilience, making them a classic multifactorial overuse injury in sport.
Why Hip Stress Fractures Happen: Biomechanics Explained Simply
Hip stress fractures occur when there is a mismatch between repetitive mechanical loading and the bone’s ability to remodel and repair itself. In healthy bone, normal loading stimulates adaptation and strengthening. However, when training volume or intensity exceeds the capacity for recovery, microscopic damage begins to accumulate faster than it can be repaired, eventually progressing into a stress fracture.
From a biomechanical perspective, the femoral neck behaves like a bending beam that transmits forces between the femoral head and the femoral shaft. Every step, jump, or running stride generates complex loading patterns that include both compressive and tensile forces.
These forces are distributed unevenly across the femoral neck:
- The inferior aspect of the femoral neck is predominantly exposed to compressive forces, which tend to “push” the bone surfaces together. Compression-sided stress injuries are generally more stable and progress more slowly.
- The superior aspect of the femoral neck is exposed to tensile forces, which “pull” the bone apart. Tensile loading is mechanically less favourable, making tension-sided stress fractures significantly more dangerous and more likely to progress to displacement.
A key contributor to this imbalance is fatigue of the hip abductor muscles, particularly the gluteus medius and minimus. When these muscles become fatigued during prolonged or intense activity, their ability to stabilize the pelvis decreases. This leads to increased bending forces across the femoral neck and a relative rise in tensile stress on the superior cortex.
Ultimately, hip stress fractures develop when training overload is combined with insufficient recovery time, creating a chronic mismatch between stress and repair. Over time, this leads to microdamage accumulation, structural weakening, and eventual failure of the bone under normal physiological loads.
Summary
In simple terms, the femoral neck is constantly “bending” under load — and when recovery is inadequate, it gradually loses its ability to withstand that bending stress.
Risk Factors You Should Never Ignore
Hip stress fractures rarely occur due to a single cause — they are almost always the result of a combination of increased mechanical load, reduced bone tolerance, and insufficient recovery capacity.
- Sudden increase in training volume or intensity (rapid mileage progression)
- Inadequate recovery between sessions (training load–recovery mismatch)
- Low bone mineral density (osteopenia or osteoporosis)
- Female athlete triad / RED-S (low energy availability, menstrual dysfunction, low bone health)
- Poor nutritional intake (especially low calorie and low calcium/vitamin D intake)
- Previous history of stress fractures
- Biomechanical factors (e.g., coxa vara, altered hip loading mechanics)
- Hip abductor fatigue leading to increased femoral neck stress during running
- High-volume endurance sports (especially long-distance and marathon running)
- Sudden change in terrain, footwear, or running surface
Hip Stress Fracture Symptoms: Early Warning Signs
Hip stress fractures often present insidiously, which is one of the main reasons diagnosis is frequently delayed. Early symptoms are subtle and easily mistaken for more common soft tissue injuries, particularly in runners and active individuals.
In the early stage, the most typical symptom is a vague, poorly localized groin pain that appears during running or high-impact activity. Athletes often describe it as a “deep discomfort” rather than sharp pain. At this stage, symptoms usually resolve with rest, which can falsely reassure both patients and clinicians.
As the condition progresses, pain becomes more consistent and appears earlier in exercise sessions, sometimes after only a short period of activity. There is often a noticeable decline in performance, with athletes reporting reduced running efficiency, slower pace, or inability to complete usual training loads. Pain may also become more persistent between sessions.
In the late stage, symptoms become significantly more concerning. Pain may be present during walking, at rest, or even at night, indicating that the structural integrity of the bone is increasingly compromised. At this point, the risk of progression to a complete fracture or displacement is significantly higher.
Several red flags should immediately raise suspicion of a hip stress fracture:
- Limping or antalgic gait
- Inability to hop on the affected leg
- Pain with weight-bearing activities
These findings suggest that the injury is no longer limited to early stress reaction but may have progressed toward a structural fracture.
However, hip stress fractures are frequently misdiagnosed in early stages as:
- Adductor muscle strain
- Hip flexor injury
- Pubic symphysis overload or “sports hernia” spectrum conditions
This overlap in symptoms often delays appropriate imaging and diagnosis.
Clinical Insight
Groin pain that worsens with impact should be considered a stress fracture until proven otherwise.
Learn how to recognize early warning signs before the condition worsens. Read more about signs of hip stress fracture and what symptoms to watch for.
Diagnosis: Clinical Examination & How We Confirm Hip Stress Fracture
The diagnosis of a hip stress fracture begins with a high index of clinical suspicion, as early findings are often subtle and easily overlooked. On clinical examination, patients typically report pain at the extremes of hip range of motion, with internal rotation being the most sensitive movement for reproducing symptoms. This reflects the biomechanical loading pattern of the femoral neck during rotational and weight-bearing activities.
Several bedside tests can support the suspicion of a femoral neck stress injury. The log roll test may reproduce deep groin pain, and axial loading or single-leg stance can also provoke symptoms. However, it is important to emphasize that physical examination findings are often non-specific, and normal examination does not exclude the diagnosis. For this reason, clinical assessment serves primarily as a trigger for imaging rather than a definitive diagnostic tool.
Initial imaging typically starts with a plain radiograph (X-ray) of the pelvis and hip. While this is an essential first step, radiographs are frequently normal in the early stages of a stress fracture, as bony changes may take several weeks to become visible. Delayed findings can include subtle sclerotic lines, cortical thickening, or a visible fracture line, but absence of these signs does not rule out pathology.
Because of these limitations, MRI is considered the gold standard for diagnosis. MRI can detect early bone marrow edema, which represents a stress reaction before a visible fracture develops. It also allows direct visualization of a fracture line and enables grading of injury severity, which is crucial for guiding management decisions.
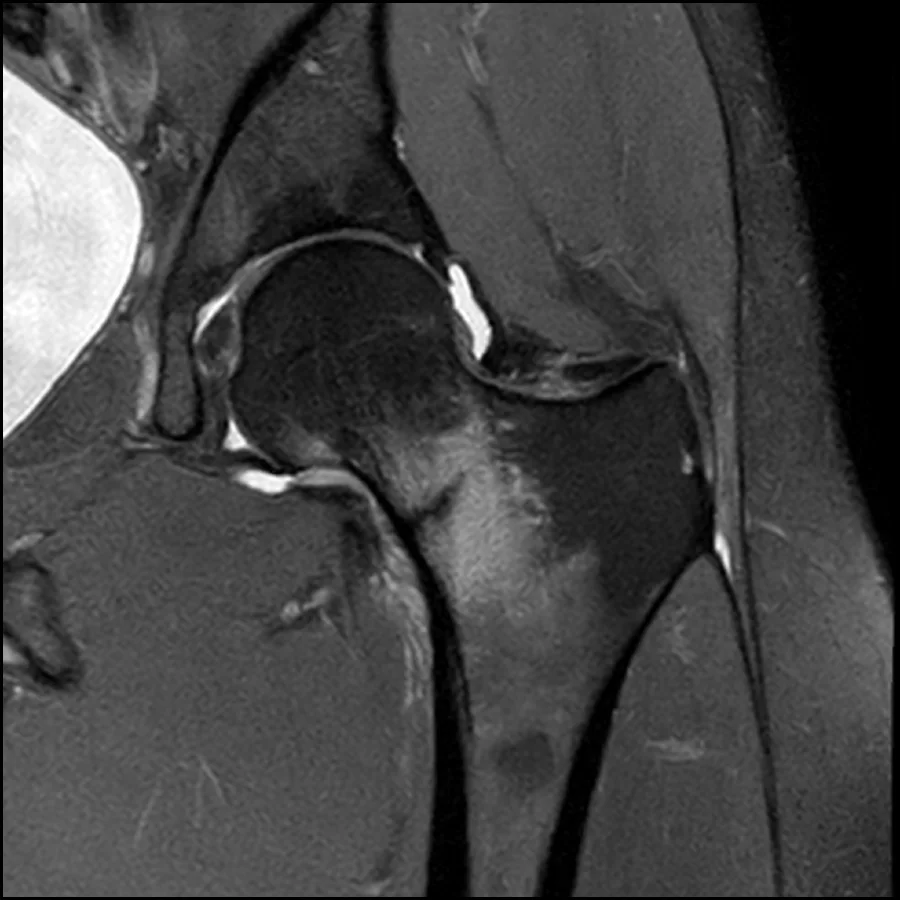
Importantly, MRI findings often change clinical management completely, distinguishing between cases that can be managed conservatively and those requiring urgent surgical intervention. This makes early imaging not only diagnostic but also prognostic in nature, directly influencing return-to-sport outcomes and complication risk.
Classification: Why It Matters for Treatment
Classification of hip stress fractures is not merely descriptive — it directly determines treatment strategy, weight-bearing status, and urgency of intervention. In clinical practice, the most important distinction is between compression-sided and tension-sided injuries, as well as whether the fracture is incomplete, complete, or displaced.
| Classification Type | Clinical Meaning | Management Implication |
|---|---|---|
| Compression-sided | Lower biomechanical risk; located on the inferior femoral neck; more stable fracture pattern | Often managed conservatively if incomplete and low symptoms |
| Tension-sided | High-risk location on superior femoral neck; exposed to tensile forces; unstable pattern | Usually requires surgical fixation due to high risk of displacement |
| Incomplete fracture | Early-stage stress injury without full cortical disruption | May be managed non-operatively with strict load modification and monitoring |
| Complete fracture | Full cortical break across femoral neck | Typically requires surgical fixation |
| Displaced fracture | Loss of anatomical alignment; high risk of vascular compromise | Orthopaedic emergency – urgent reduction and fixation required |
In essence, classification functions as a treatment algorithm in disguise. Compression-sided incomplete injuries sit on the conservative end of the spectrum, while tension-sided and displaced fractures shift rapidly into surgical territory. This distinction is critical because outcomes are strongly time-dependent — particularly in displaced injuries, where delay significantly increases the risk of complications such as avascular necrosis.
Hip Stress Fracture Treatment
The treatment of hip stress fractures is fundamentally guided by one central principle: fracture stability combined with the presence or absence of displacement determines the management pathway. Because outcomes can deteriorate rapidly in high-risk patterns, early and correct stratification is essential.
Conservative management
Non-operative treatment is reserved for carefully selected low-risk injuries, most commonly incomplete compression-sided femoral neck stress fractures. These injuries occur on the inferior aspect of the femoral neck, where compressive forces provide relative mechanical stability.
Conservative management typically includes:
- Strict non-weight bearing with crutches
- Activity cessation from impact loading (running, jumping)
- Gradual and closely supervised return to partial loading only after symptom resolution
- Regular clinical review and repeat imaging (usually MRI or radiographs depending on protocol)
The key objective in conservative care is to prevent progression of the stress injury. Even within this group, careful monitoring is essential, as increasing pain or radiological progression may indicate impending structural failure and necessitate surgical intervention.
Surgical management
Surgical treatment is indicated in higher-risk patterns, where mechanical instability or fracture propagation significantly increases the risk of displacement and complications. This includes:
- Tension-sided fractures (superior femoral neck involvement)
- Complete fractures (full cortical disruption)
- Any displaced fracture (loss of anatomical alignment)
These injuries are inherently unstable due to tensile loading forces acting across the femoral neck, making non-operative treatment unsafe in most cases.
The primary goals of surgery are:
- Restore and maintain anatomical alignment
- Prevent fracture displacement or progression
- Preserve femoral head vascularity
- Enable safe rehabilitation and return to function
Common fixation methods include:
- Cannulated screws (multiple screw fixation): commonly used for compression-sided and some complete fractures, providing stable internal fixation with minimal invasiveness.
- Dynamic Hip Screw (DHS): preferred in more vertical, unstable, or tension-sided fracture patterns due to superior mechanical resistance to shear forces.
In displaced fractures, fixation is often combined with urgent reduction to minimize the risk of complications such as avascular necrosis.
Key decision principle
Ultimately, management decisions can be simplified into a practical clinical framework:
Stability + displacement = treatment pathway
- Stable, incomplete compression injuries → conservative management
- Unstable, tension-sided or complete fractures → surgical fixation
- Displaced fractures → emergency orthopaedic intervention
This structured approach ensures that patients are treated according to biomechanical risk rather than symptoms alone, which is critical in preventing progression to catastrophic hip failure.
| Fracture Type | Incomplete (<50% Femoral Neck Width) | Complete (>50% Femoral Neck Width) |
|---|---|---|
| Compression | Conservative – unless significant pain or inability to straight-leg raise | Surgical fixation (Cannulated hip screws or Dynamic Hip Screw) |
| Tension | Surgical fixation (Dynamic Hip Screw) | Surgical fixation (Dynamic Hip Screw) |
| Displaced | — | Immediate reduction and surgical fixation (Dynamic Hip Screw ± derotation screw) |
| Atypical tension | Conservative | Surgical fixation (Dynamic Hip Screw) |
Recovery & Rehabilitation
Recovery from a hip stress fracture is a structured, phase-based process, where progression is guided by symptoms, clinical response, and imaging rather than fixed timelines alone. The main goal is to allow bone healing while progressively restoring safe mechanical loading across the femoral neck.
Phased rehabilitation approach
Rehabilitation is typically divided into three key stages:
- Protection phase
The primary aim is to reduce stress across the affected femoral neck. This may include non-weight bearing or partial weight bearing depending on severity. The priority is to prevent progression of the injury. - Progressive loading phase
Gradual reintroduction of load is initiated once symptoms improve. Bone responds positively to controlled mechanical stress, which is essential for remodeling. However, excessive loading at this stage increases recurrence risk. - Functional reconditioning phase
Focus shifts toward restoring lower-limb strength, endurance, and movement quality in preparation for return to higher-level activity.
Physiotherapy focus
Key rehabilitation targets include:
- Gluteal strengthening (gluteus medius and minimus)
- Restoration of hip stability and pelvic control
- Correction of biomechanical load patterns
- Progressive lower-limb conditioning
Hip abductor fatigue is particularly important, as it increases tensile stress across the femoral neck during repetitive loading such as running.
Return to Activity and Sport
Return to activity after a hip stress fracture should be understood as a criteria-based progression rather than a fixed timeline. The key principle is that the athlete must demonstrate both biological healing of the bone and functional readiness of the entire kinetic chain before any return to impact loading is allowed.
Return to basic activity (low-impact function)
The first milestone is return to pain-free daily activity. This includes:
- walking without pain or limp
- ability to perform normal stair climbing
- absence of pain at rest and during sleep
- tolerance of low-impact conditioning (e.g., cycling or swimming if symptom-free)
Only when these criteria are met can progression toward higher loading begin. At this stage, the goal is to restore baseline functional capacity without provoking symptoms.
Return to impact preparation
Before running is reintroduced, the athlete should demonstrate:
- full, pain-free range of hip motion
- good single-leg control (no pelvic drop or instability)
- restored strength of hip abductors and extensors
- ability to tolerate progressive strengthening without symptom recurrence
This phase bridges rehabilitation and sport-specific loading and is often where inadequate progression leads to recurrence.
Return to running and sport
Impact loading is reintroduced gradually using structured walk–run progressions. Running is increased in volume and intensity only if the athlete remains completely asymptomatic. Key principles include:
- gradual load progression (no sudden spikes in volume or intensity)
- avoidance of pain during or after sessions
- ongoing monitoring of fatigue and biomechanics
Full return to sport is typically achieved once the athlete can tolerate continuous running and sport-specific drills without symptoms.
Clinical Insight
Return to sport should never be based on time alone. Instead, it must reflect:
Pain-free function + restored strength + controlled loading capacity + confirmed healing
Failure to respect these criteria significantly increases the risk of recurrence or progression of injury.
Complications: Why Early Diagnosis Saves Hips
Hip stress fractures, particularly those involving the femoral neck, carry significant risk if diagnosis is delayed or missed. While early-stage injuries are highly treatable, progression to more severe structural failure can result in long-term morbidity, especially in young and active individuals.
The most serious complication is avascular necrosis (AVN) of the femoral head. This occurs when disruption of blood supply follows fracture displacement, potentially leading to irreversible bone death and joint collapse. Another important complication is non-union, where the fracture fails to heal due to continued mechanical stress or inadequate stabilization.
If the injury is not identified early, progression from an incomplete stress injury to a complete or displaced fracture may occur. Displacement significantly worsens prognosis and is strongly associated with higher complication rates and longer recovery times. Even with appropriate surgical management, outcomes are less predictable once displacement has occurred.
Long-term consequences can include early onset hip osteoarthritis, resulting from altered joint mechanics and cartilage degeneration. In severe cases, particularly following AVN or failed fixation, patients may ultimately require total hip replacement, which is a major concern in young athletic populations.
The key clinical principle is straightforward:
Delay in diagnosis leads to exponential increase in risk
Early recognition, prompt imaging (especially MRI), and appropriate load management are therefore critical in preventing progression to these complications. In clinical practice, timing is often the single most important determinant of outcome in hip stress fractures.
Prevention: Reducing the Risk of Hip Stress Fractures
Prevention of hip stress fractures relies on controlling the balance between training load, recovery, and bone health adaptation. The most important modifiable risk factor is rapid increases in training volume, particularly in runners. A gradual progression in mileage and intensity is essential to allow bone remodeling to adapt to mechanical stress.
Key preventive strategies include:
- avoiding sudden spikes in running volume or intensity
- ensuring adequate recovery between high-load sessions
- maintaining sufficient energy availability and nutritional intake
- early management of persistent groin pain with prompt imaging if needed
From a biomechanical perspective, improving hip stability and gluteal strength may reduce excessive femoral neck loading during repetitive activity. Screening high-risk athletes—especially endurance runners and those with low energy availability—can also help identify early stress reactions before fracture development.
Education is a central component of prevention. Athletes and coaches should understand that persistent groin pain in a runner should always be treated as a potential stress injury until proven otherwise.
In essence, prevention is not about eliminating load, but about optimizing the relationship between load, recovery, and bone capacity.
Key Takeaways
Hip stress fractures represent a continuum of bone stress injury, ranging from early stress reactions to complete and potentially displaced fractures. Although relatively uncommon, they are clinically important due to their potential to cause severe long-term complications in young and active individuals.
Early symptoms are often subtle, typically presenting as vague exercise-related groin pain, which can easily be misdiagnosed. This makes a high index of suspicion essential, particularly in runners and military recruits.
Imaging plays a central role in diagnosis. While X-rays are often normal in early stages, MRI is the gold standard for detecting early bone stress changes and guiding management decisions.
Treatment is entirely driven by fracture location, severity, and stability:
- compression-sided injuries → often managed conservatively
- tension-sided or complete fractures → usually require surgery
- displaced fractures → orthopaedic emergency
Recovery requires a structured, phase-based rehabilitation approach, with careful progression from protection to loading and finally return to sport.
The most important clinical principle remains:
Early diagnosis dramatically improves outcomes and prevents catastrophic progression
Ultimately, hip stress fractures are highly treatable when identified early, but potentially devastating when missed or delayed.
Robertson GA, Wood AM. Femoral Neck Stress Fractures in Sport: A Current Concepts Review. Sports Med Int Open. 2017;1(2):E58–E68. PubMed: Femoral neck stress fractures in sport review
Bernstein EM et al. Femoral Neck Stress Fractures: An Updated Review. J Am Acad Orthop Surg. 2022;30(7):302–311. PubMed: Updated review of femoral neck stress fractures
Arendt EA, Griffiths HJ. Femoral Neck Stress Fractures: MRI Classification and Prognostic Value. AJR Am J Roentgenol. MRI-based classification of femoral neck stress injuries
Ackerman KE, Misra M. Bone health and the female athlete triad in adolescent athletes. Phys Sportsmed. 2011;39(1):131–141. Female athlete triad and bone health in adolescents
StatPearls. Stress Fractures. NCBI Bookshelf. Comprehensive review of stress fracture diagnosis and management

















