

Traumatic shoulder injuries are common in falls, sports collisions, and everyday accidents. The shoulder is the most mobile joint in the human body, but that mobility comes at a cost — it is also one of the least stable. When a strong external force acts on the arm or shoulder girdle, the structures that keep the joint centered can fail, leading to tears, dislocations, or fractures.
Trauma can affect both soft tissues (such as the rotator cuff or labrum) and bony structures like the humerus or clavicle. Without timely diagnosis and proper management, these injuries may progress to chronic pain, weakness, instability, and long‑term loss of function.
This guide focuses on the most important traumatic shoulder injuries — how they happen, the symptoms they cause, and the treatment options available — explained in clear, accessible language for patients and clinicians alike.
Quick Overview – Traumatic Shoulder Injuries
- Traumatic shoulder injuries most often result from falls, sports collisions, or sudden traction forces that overload stabilizing structures.
- The most common injuries include rotator cuff tears, shoulder dislocations, SLAP tears, and AC joint separations.
- Mechanisms of injury typically involve a fall on an outstretched hand, a direct blow to the shoulder, or forceful rotation of the arm.
- Diagnosis relies on clinical examination supported by imaging such as X‑ray, ultrasound, or MRI to identify soft‑tissue or bony damage.
- Management ranges from rest and physiotherapy to surgical repair, depending on the severity, displacement, and functional demands.
- Most patients achieve good recovery with timely evaluation and appropriate treatment, reducing the risk of chronic pain or instability.
Overview of Traumatic Shoulder Injuries
Traumatic shoulder injuries are a common consequence of falls, sports collisions, and sudden high‑energy impacts. Because the shoulder is the most mobile joint in the body, it relies heavily on soft‑tissue structures for stability. When a strong external force acts on the arm or shoulder girdle, these stabilizing tissues can fail, resulting in a shoulder injury such as a tear, dislocation, or fracture.
Why the Shoulder Is Prone to Trauma
- The glenohumeral joint has a shallow socket, providing mobility but limited inherent stability.
- Stability depends on dynamic soft‑tissue control (rotator cuff, scapular muscles) that can be overwhelmed by sudden force.
- The shoulder is frequently placed in vulnerable positions during falls, overhead movements, and contact sports.
- Rapid twisting, traction, or impact can exceed the joint’s ability to stay centered.
Common Mechanisms of Injury
- Fall on an outstretched hand (FOOSH) — classic cause of dislocations, labral tears, and fractures.
- Direct blow to the shoulder — common in contact sports and cycling or skiing accidents.
- Sudden traction or pulling force — may injure the rotator cuff or superior labrum.
- Forceful rotation of the arm — can lead to dislocation or tearing of stabilizing structures.
- High‑energy trauma — such as motor‑vehicle accidents, often associated with fractures.

Common Traumatic Shoulder Injuries
Some traumatic shoulder injuries occur far more frequently than others, and this section focuses on the core group of injuries seen most often in clinical practice.
- Traumatic Rotator Cuff Tear
- Shoulder Dislocation (including Bankart and Hill‑Sachs lesions)
- SLAP Tear
- AC Joint Separation
1. Traumatic Rotator Cuff Tear
What Structure Is Injured
A traumatic rotator cuff tear happens when one of the shoulder’s stabilizing tendons suddenly rips during an accident. The supraspinatus is most often involved.
Mechanism of Injury
People usually describe a clear moment when the injury happens. Most often, they fall and reach out with the arm to protect themselves, and the shoulder takes the full force. Others try to catch something heavy that slips from their hands, and the arm gets pulled downward faster than the shoulder can react.
Athletes may feel a sharp pain during a strong overhead movement — a serve, a swing, or a sudden stop — when the arm is forced back unexpectedly. In all these situations, the tendon is pushed beyond what it can safely handle, and it tears in that instant.
Symptoms
- Sudden, sharp pain at the moment of injury
- Immediate weakness, especially when lifting the arm
- Difficulty or inability to raise the arm overhead
- Night pain, especially when lying on the injured side
- Limited active motion with relatively preserved passive motion
How Serious Is It?
This is a meaningful shoulder injury because strength drops right away. Larger tears can retract quickly, and delaying treatment may reduce long‑term recovery potential. If someone cannot lift the arm after trauma, they should be evaluated promptly.
Diagnosis
Diagnosis includes a physical exam and imaging. Ultrasound or MRI confirms the tear and shows its size, while X‑rays help rule out fractures that can mimic a cuff injury.
Treatment Options
Smaller tears may improve with physical therapy focused on restoring motion and strength. Larger, sudden tears — especially in active individuals — often benefit from surgical repair to restore shoulder function.
Recovery and Prognosis
Non‑operative recovery usually takes 6–12 weeks. Surgical repair requires a longer timeline, with full recovery typically taking 4–6 months.comes are best when traumatic tears are diagnosed and treated early.
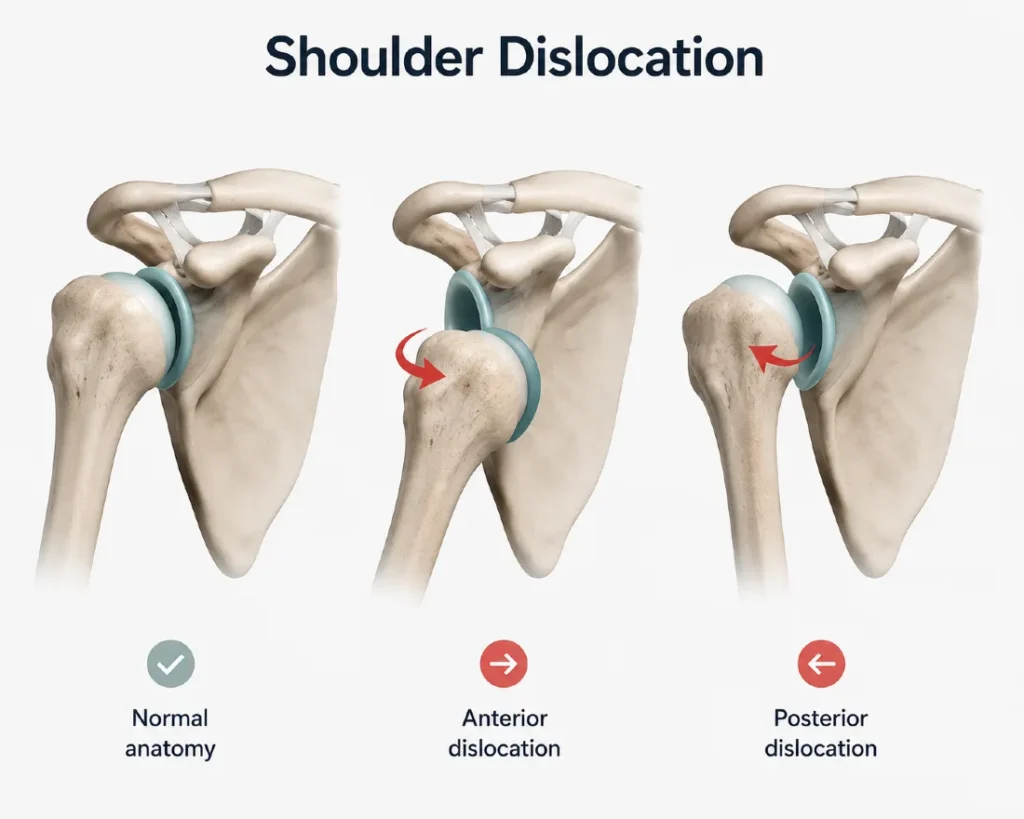
2. Shoulder Dislocation
What Structure Is Injured
A shoulder dislocation happens when the head of the humerus slips out of the shoulder socket. Most dislocations are anterior, meaning the arm moves forward out of place. This often stretches or tears the labrum and surrounding ligaments that normally keep the joint stable.
Mechanism of Injury
People usually describe a fall or sudden force that pushes the arm into an awkward position. A common scenario is falling on an outstretched hand, where the arm is forced backward and rotated outward. Others injure the shoulder during sports when the arm is hit or pulled while raised overhead. Some feel the shoulder “pop out” during a sudden twisting movement or when reaching behind them. The moment it happens is usually unmistakable — the shoulder shifts out of place, followed by sharp pain and loss of control.
Symptoms
- Immediate, intense shoulder pain
- Visible deformity or the feeling that the shoulder is “out of place”
- Inability to move the arm normally
- Muscle spasm around the shoulder
- Numbness or tingling down the arm in some cases
How Serious Is It
A dislocation is a significant shoulder injury because it can damage the labrum, ligaments, and sometimes nearby nerves. Once the shoulder dislocates, the risk of it happening again increases, especially in younger and active individuals. Prompt reduction and evaluation are important to prevent complications.
Diagnosis
Diagnosis is based on the clinical appearance and confirmed with X‑rays to ensure the shoulder is out of place and to rule out fractures. MRI may be used later to assess labral or ligament injuries, especially if instability persists.
Treatment Options
The first and most important step is for the patient to go to the emergency department, where the shoulder can be safely evaluated and relocated by medical staff. Once the shoulder is back in place, a short period of rest and a sling may be recommended, followed by physical therapy to restore strength and stability. Recurrent dislocations or significant labral injuries may require surgical stabilization, particularly in younger athletes.
Recovery and Prognosis
Most people regain basic function within a few weeks, but full recovery of strength and stability typically takes 6–12 weeks. Those with repeated dislocations or major labral tears may need surgery for long‑term stability.
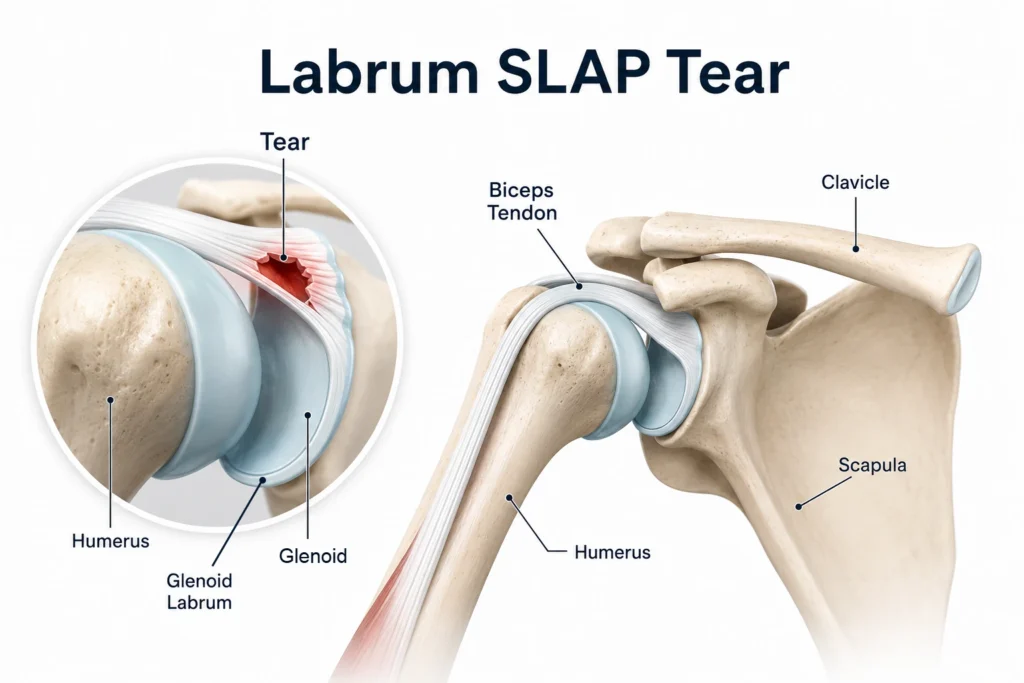
3. SLAP Tear
What Structure Is Injured
A SLAP tear is an injury to the superior labrum, the ring of cartilage that deepens the shoulder socket. The tear occurs at the top part of the labrum, where the long head of the biceps tendon attaches. When this area is damaged, the shoulder may feel unstable, painful, or “catchy” during certain movements.
Mechanism of Injury
People often describe a sudden pulling or twisting force on the arm. A common scenario is trying to stop a fall by grabbing onto something, which puts a strong traction force on the biceps tendon. Others feel the injury during overhead sports — a serve, a throw, or a powerful swing — especially when the arm is forced backward or when the motion suddenly stops. Some notice the pain after lifting something heavy with the arm extended. In all these situations, the top part of the labrum is stressed beyond its limit, and the attachment area tears.
Symptoms
- Deep shoulder pain, often hard to pinpoint
- Pain with overhead or throwing movements
- Clicking, catching, or popping inside the joint
- Weakness or loss of power in overhead activities
- Discomfort when lifting objects away from the body
How Serious Is It
A SLAP tear can significantly affect shoulder function, especially in people who rely on overhead strength or precision. While not dangerous, it can be persistent and frustrating, and symptoms often worsen with repeated overhead use. Early evaluation helps determine whether the tear is stable or likely to cause ongoing problems.
Diagnosis
Diagnosis is based on a combination of history, specific clinical tests, and imaging. MRI with contrast is the most reliable method for confirming a SLAP tear, as it shows the labrum and biceps anchor in detail. X‑rays are usually normal but help rule out other causes of shoulder pain.
Treatment Options
Many SLAP tears improve with physical therapy focused on restoring shoulder mechanics, strengthening the rotator cuff, and reducing stress on the biceps tendon. Activity modification is often helpful. Persistent symptoms, especially in athletes or those with mechanical catching, may require arthroscopic surgery to repair or debride the torn labrum.
Recovery and Prognosis
Non‑operative recovery typically takes 6–12 weeks, depending on activity demands. After surgery, recovery is longer: gradual strengthening begins after several weeks, and full return to overhead sports may take 4–6 months. Most people regain good shoulder function with appropriate treatment.
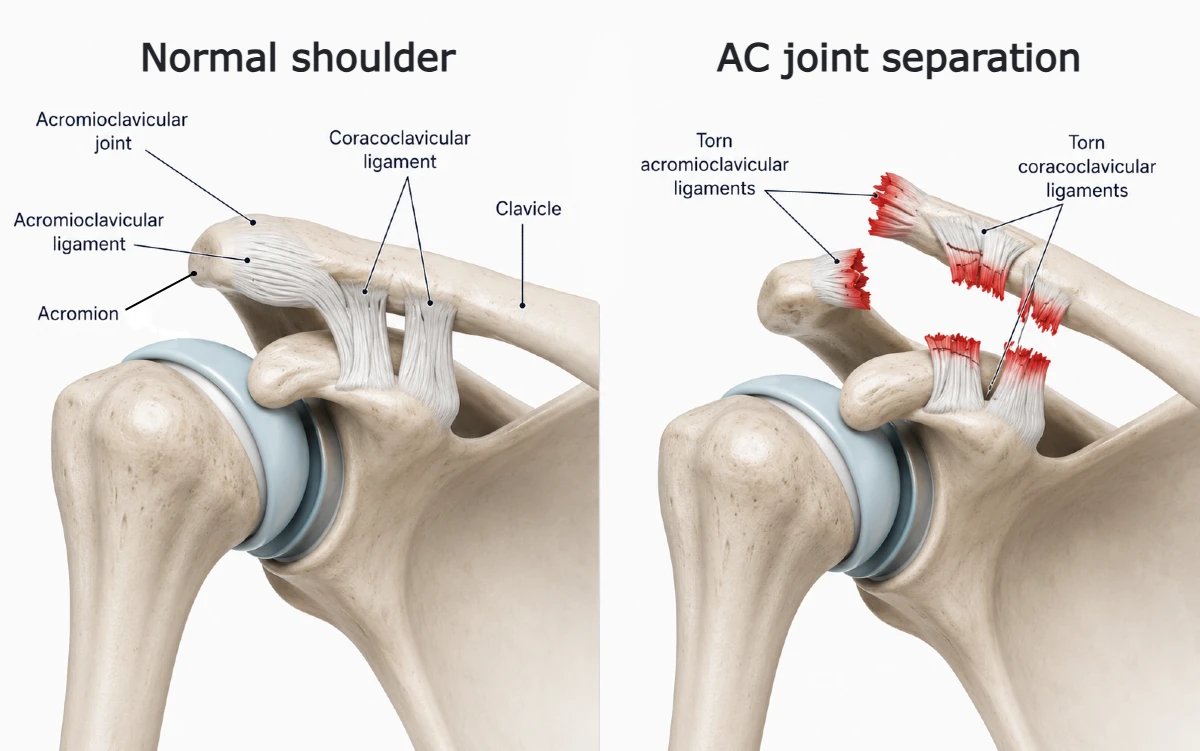
4. AC Joint Separation
What Structure Is Injured
An AC joint separation occurs when the ligaments that connect the collarbone (clavicle) to the top of the shoulder blade (acromion) are stretched or torn. Depending on the severity, the clavicle may sit slightly higher than normal or become visibly elevated.
Mechanism of Injury
Most people injure the AC joint during a fall directly onto the top of the shoulder. Cyclists often describe landing on the shoulder after slipping or being pushed off balance. In contact sports, the injury happens when the shoulder is driven into the ground or hit from the side. Sometimes it occurs during a fall on an outstretched hand, but direct impact to the shoulder is the most common cause. The moment of injury is usually sharp and localized right at the top of the shoulder.
Symptoms
- Pain on the top of the shoulder
- Swelling or a visible bump over the AC joint
- Pain when lifting the arm or reaching across the body
- Tenderness when pressing on the joint
- Limited shoulder motion in the first few days
How Serious Is It
Most AC joint separations are mild to moderate and heal well with conservative care. Higher‑grade injuries, where the clavicle is clearly elevated, may cause long‑term discomfort or instability if not treated properly. Although not dangerous, the injury can be very painful in the first days and may limit daily activities.
Diagnosis
Diagnosis is based on physical examination and X‑rays, which help determine the severity of the separation. Stress views or comparison with the opposite shoulder may be used to assess ligament damage.
Treatment Options
Most AC joint separations are treated without surgery. Rest, ice, and a short period in a sling help reduce pain. Physical therapy focuses on restoring motion and strengthening the shoulder girdle. Surgery is considered for high‑grade separations, persistent pain, or athletes who require strong overhead stability.
Recovery and Prognosis
Mild injuries often improve within 2–4 weeks, while moderate cases may take 6–8 weeks. High‑grade injuries or surgical cases require a longer recovery, but most people return to normal activities with good shoulder function.
Less Common Traumatic Shoulder Injuries
Some traumatic shoulder injuries occur less frequently but are still clinically important, especially after high‑energy trauma or direct impact. This section covers injuries that are not seen every day but should always be considered in patients with significant shoulder pain after an accident.
- Greater Tuberosity Fracture
- Proximal Humerus Fracture
- Sternoclavicular Joint Injury
- Glenoid Fracture
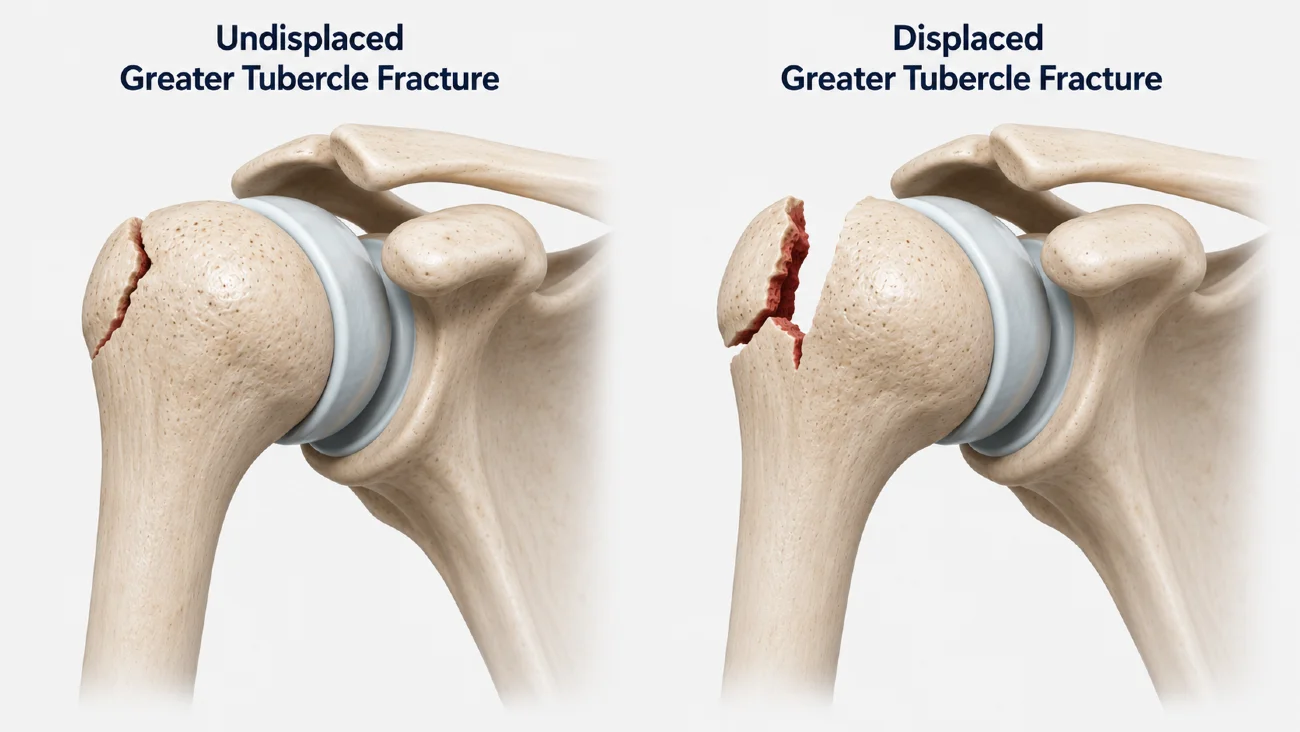
5. Greater Tuberosity Fracture
What Structure Is Injured
A greater tuberosity fracture is a break in the upper part of the humerus where the supraspinatus and infraspinatus attach. Even small shifts in this area can affect shoulder strength and rotation.
Mechanism of Injury
Most injuries happen after a fall onto the shoulder or an outstretched hand. The force pulls sharply on the rotator cuff tendons, causing the bone fragment to crack. It also commonly occurs together with an anterior shoulder dislocation. Patients usually describe a fall followed by immediate pain on the outer shoulder.
Symptoms
- Pain over the outer shoulder
- Difficulty lifting the arm
- Weakness in elevation or rotation
- Swelling or bruising
How Serious Is It
Most fractures are mild and heal well, but displacement can affect rotator cuff function. Proper assessment is important to avoid long‑term weakness.
Diagnosis
X‑rays confirm the fracture and its displacement. MRI or ultrasound may be used if a rotator cuff tear is suspected.
Treatment Options
Nondisplaced fractures are treated with rest, a sling, and gradual physical therapy. Surgery is considered when the fragment is significantly displaced or shoulder function is limited.
Recovery and Prognosis
Most nondisplaced fractures heal in 6–8 weeks. Surgical cases take longer but generally recover well with proper rehabilitation.
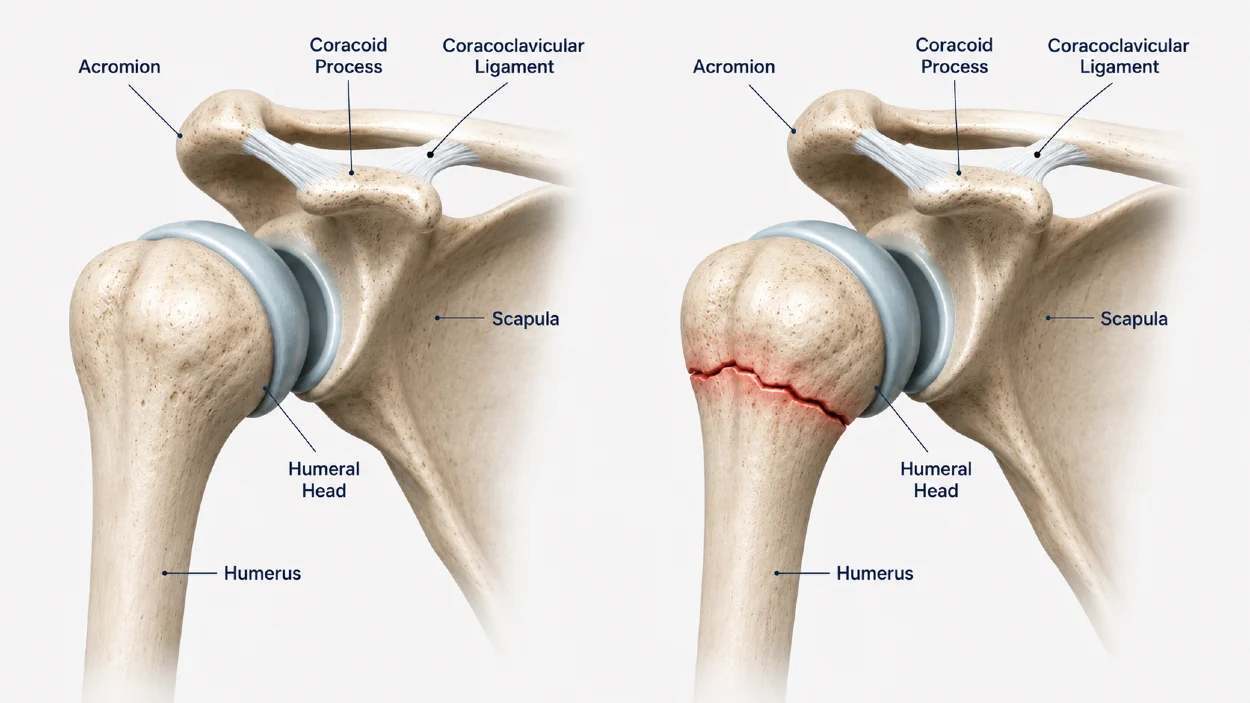
6. Proximal Humerus Fracture
What Structure Is Injured
A proximal humerus fracture is a break in the upper part of the arm bone, near the shoulder joint. It can involve the surgical neck, the greater tuberosity, or both.
Mechanism of Injury
Most occur after a fall directly onto the shoulder or upper arm, especially in older adults with weaker bone density. Patients usually describe a fall, immediate pain, and difficulty moving the arm.
Symptoms
- Pain around the upper arm and shoulder
- Swelling and bruising
- Difficulty lifting the arm
- Pain with any shoulder movement
How Serious Is It
Many fractures are stable and heal well without surgery. More complex fractures, especially those with displacement or multiple fragments, may affect shoulder function and require specialist evaluation.
Diagnosis
X‑rays confirm the fracture pattern. CT scans may be used for complex or multi‑fragment injuries.
Treatment Options
Most stable fractures are treated with a sling, rest, and gradual physical therapy. Surgery is considered for displaced fractures, multi‑fragment injuries, or cases where joint alignment is compromised.
Recovery and Prognosis
Healing usually takes 6–12 weeks, depending on the fracture type. Early motion is important to prevent stiffness.
7. Sternoclavicular (SC) Joint Injury
What Structure Is Injured
An SC joint injury affects the joint between the collarbone and the sternum. Ligaments can stretch or tear, causing instability.
Mechanism of Injury
These injuries usually occur after a strong impact to the chest or shoulder, such as a fall, sports collision, or car accident. Patients often describe a direct blow followed by pain near the center of the chest.
Symptoms
- Pain at the base of the neck or upper chest
- Swelling or tenderness over the SC joint
- Pain with arm elevation or reaching
How Serious Is It
Most injuries are mild, but posterior dislocations (rare) can be serious because the clavicle can press on vital structures behind the sternum. Any suspected posterior injury requires urgent evaluation.
Diagnosis
X‑rays may show the injury, but CT scans are often needed for accurate assessment.
Treatment Options
Most injuries are treated with rest, a sling, and gradual return to activity. Severe instability or posterior displacement may require surgical management.
Recovery and Prognosis
Most patients recover within 4–8 weeks, depending on severity.
8. Glenoid Fracture
What Structure Is Injured
A glenoid fracture is a break in the socket portion of the shoulder blade. It can affect joint stability and cartilage alignment.
Mechanism of Injury
These fractures typically occur during high‑energy trauma, such as a fall from height, a sports collision, or a shoulder dislocation where the humeral head impacts the glenoid rim.
Symptoms
- Deep shoulder pain
- Limited motion
- Pain with any attempt to lift the arm
How Serious Is It
Because the glenoid forms the socket of the shoulder, fractures can affect joint stability. Some are small and stable, while others require surgical repair to restore joint alignment.
Diagnosis
X‑rays may show the fracture, but CT scans provide the best detail for treatment planning.
Treatment Options
Small, stable fractures are treated with rest and physical therapy. Larger rim fractures or those affecting joint stability often require surgery.
Recovery and Prognosis
Recovery varies but typically ranges from 8–12 weeks, with full return to activity depending on fracture size and treatment.
Key Takeaways
- Traumatic shoulder injuries most often result from falls, sports collisions, or sudden traction forces, leading to rotator cuff tears, dislocations, SLAP tears, or AC joint separations.
- The shoulder is highly mobile but structurally vulnerable, making it prone to injury when exposed to sudden impact, twisting, or overload.
- Early recognition of symptoms — pain, weakness, deformity, or loss of motion — helps guide timely evaluation and prevents long‑term complications.
- Most injuries improve with structured rehabilitation, while some (especially dislocations and larger tears) may require surgical treatment.
- Less common injuries such as greater tuberosity fractures, proximal humerus fractures, SC joint injuries, and glenoid fractures should be considered after high‑energy trauma.
When to Seek Medical Attention
Seek medical attention promptly if you experience any of the following after a shoulder injury:
- Inability to lift the arm — especially if the arm suddenly became weak or cannot be raised overhead.
- Visible deformity — such as the shoulder looking “out of place” or the collarbone appearing elevated.
- Severe or worsening pain — especially if it does not improve with rest or simple movement.
- Numbness or tingling — which may indicate nerve involvement.
- Significant swelling or bruising — particularly if it spreads down the arm.
- Suspected dislocation or fracture — these require urgent evaluation in the emergency department.
- Pain after high‑energy trauma — such as a cycling crash, skiing fall, or motor‑vehicle accident.
Early assessment helps prevent complications such as chronic instability, persistent weakness, or long‑term loss of shoulder function.
Who Is Most at Risk
Certain groups are more likely to experience traumatic shoulder injuries due to biomechanics, activity level, or bone and soft‑tissue vulnerability. The highest‑risk groups include:
- Athletes in overhead sports — tennis, volleyball, handball, baseball, and swimming place repeated stress on the shoulder, increasing susceptibility to acute tears and dislocations.
- Older adults — reduced bone density and slower reaction times make falls more likely to result in fractures or rotator cuff tears.
- People with previous shoulder injuries — prior dislocations, labral tears, or instability episodes significantly increase the chance of reinjury.
- Cyclists, skiers, and contact‑sport athletes — these activities involve high‑energy impacts and falls that commonly lead to AC separations, fractures, or dislocations.
- Individuals exposed to frequent falls — including manual laborers, construction workers, and people with balance issues.
- People performing sudden heavy lifting — unexpected traction forces can injure the rotator cuff or superior labrum.
Understanding these risk groups helps guide prevention strategies and early recognition of symptoms after trauma.
Prevention Tips
Preventing traumatic shoulder injuries starts with maintaining strong and well‑coordinated shoulder muscles. Strengthening the rotator cuff helps keep the joint centered, while good scapular control stabilizes the shoulder blade during overhead and impact activities. It is also important to avoid sudden heavy lifting, as unexpected traction forces can overload the labrum or rotator cuff.
In contact sports, protective gear reduces the impact on the AC joint and clavicle, and fall‑prevention strategies are especially valuable for older adults or anyone with balance issues. For athletes, gradually increasing the intensity of overhead training helps prevent overload and reduces the risk of acute injury.
Mastrantonakis K, Karvountzis A, Yiannakopoulos CK, Kalinterakis G. Mechanisms of shoulder trauma: Current concepts. World Journal of Orthopedics. Review article: Current concepts in shoulder trauma mechanisms and injury patterns
Bao MH, DeAngelis JP, Wu JS. Imaging of traumatic shoulder injuries – Understanding the surgeon’s perspective. European Journal of Radiology Open. Imaging review: Traumatic shoulder injuries and surgical decision-making
Abdelwahab A, Ahuja N, Iyengar KP, Jain VK, Bakti N, Singh B. Traumatic rotator cuff tears – Current concepts in diagnosis and management. Journal of Clinical Orthopaedics and Trauma. Current concepts review: Diagnosis and treatment of traumatic rotator cuff tears
Pak T, Kim AM. Anterior Glenohumeral Joint Dislocation. StatPearls Publishing. Evidence-based overview: Anterior shoulder dislocation diagnosis and management
Kiel J, Taqi M, Kaiser K. Acromioclavicular Joint Injury. StatPearls Publishing. Clinical review: Acromioclavicular joint injury evaluation and treatment
Familiari F, Huri G, Simonetta R, McFarland EG. SLAP lesions: Current controversies. EFORT Open Reviews. Review article: Current evidence and controversies in SLAP lesion diagnosis and treatment

















