

De Quervain’s tenosynovitis is a painful condition affecting the tendons on the thumb side of the wrist. It develops when the tendon sheath around the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons becomes irritated and thickened, making thumb movements painful and restricted.
The condition commonly affects adults between 30 and 50 years of age, especially women, new mothers, and people who perform repetitive gripping, lifting, twisting, or pinching motions with the hand and wrist.
Common symptoms include pain near the base of the thumb, tenderness along the wrist, swelling, and difficulty gripping or lifting objects. Symptoms often worsen during activities such as texting, typing, opening jars, carrying a child, or repetitive hand use.
First described by Swiss surgeon Fritz de Quervain in 1895, it remains one of the most common causes of radial‑sided wrist pain today.
This article explains the causes, symptoms, diagnosis, and evidence-based treatment options for De Quervain’s tenosynovitis, along with practical tips to reduce pain and improve hand function.
Key Clinical Points – De Quervain’s Tenosynovitis
- De Quervain’s tenosynovitis is a stenosing tenosynovitis of the APL and EPB tendons within the first dorsal compartment, causing radial-sided wrist pain.
- The condition typically presents with dorsal–radial wrist pain aggravated by gripping, lifting, ulnar deviation, or repetitive thumb movements.
- Finkelstein’s test is the most sensitive clinical maneuver, producing sharp pain along the radial styloid during passive ulnar deviation.
- Early management includes activity modification, NSAIDs, and continuous use of a thumb spica brace for 3–4 weeks.
- Corticosteroid injection into the tendon sheath is the most effective non‑surgical treatment, with 65–100% symptom resolution after a single injection.
- Targeted exercises (stretching and strengthening) improve tendon gliding and support recovery once acute pain decreases.
- Surgical release of the first dorsal compartment is reserved for persistent or recurrent cases and generally yields excellent outcomes.
Mechanism and Causes of De Quervain’s Tenosynovitis
To understand what happens in De Quervain’s tenosynovitis, it is useful to briefly review the relevant anatomy.
The condition involves two tendons of the thumb — the abductor pollicis longus (APL) and extensor pollicis brevis (EPB). These are the primary tendons responsible for thumb movement, allowing the thumb to move away from the hand and assist in extension. Both originate in the forearm muscles and travel together toward the thumb, passing through a tight fibro-osseous tunnel on the radial side of the wrist.
Tendons are strong, cable-like structures that connect muscle to bone and transmit force to produce movement. At the wrist, they are surrounded by a synovial tendon sheath, which contains a thin lubricating membrane (synovial lining) that allows smooth gliding during motion by reducing friction.
The APL and EPB tendons pass through a narrow channel called the first dorsal compartment, approximately 2 cm in length. The floor of this tunnel is formed by the radial styloid groove of the radius, while the roof is formed by the extensor retinaculum, a strong fibrous band that stabilizes the tendons in place.
In De Quervain’s tenosynovitis, there is thickening of both the tendons and the surrounding synovial sheath, most likely driven by a chronic inflammatory process.
This leads to a relative narrowing of the already confined first dorsal compartment. As the available space decreases, tendon gliding becomes restricted, increasing friction during movement.
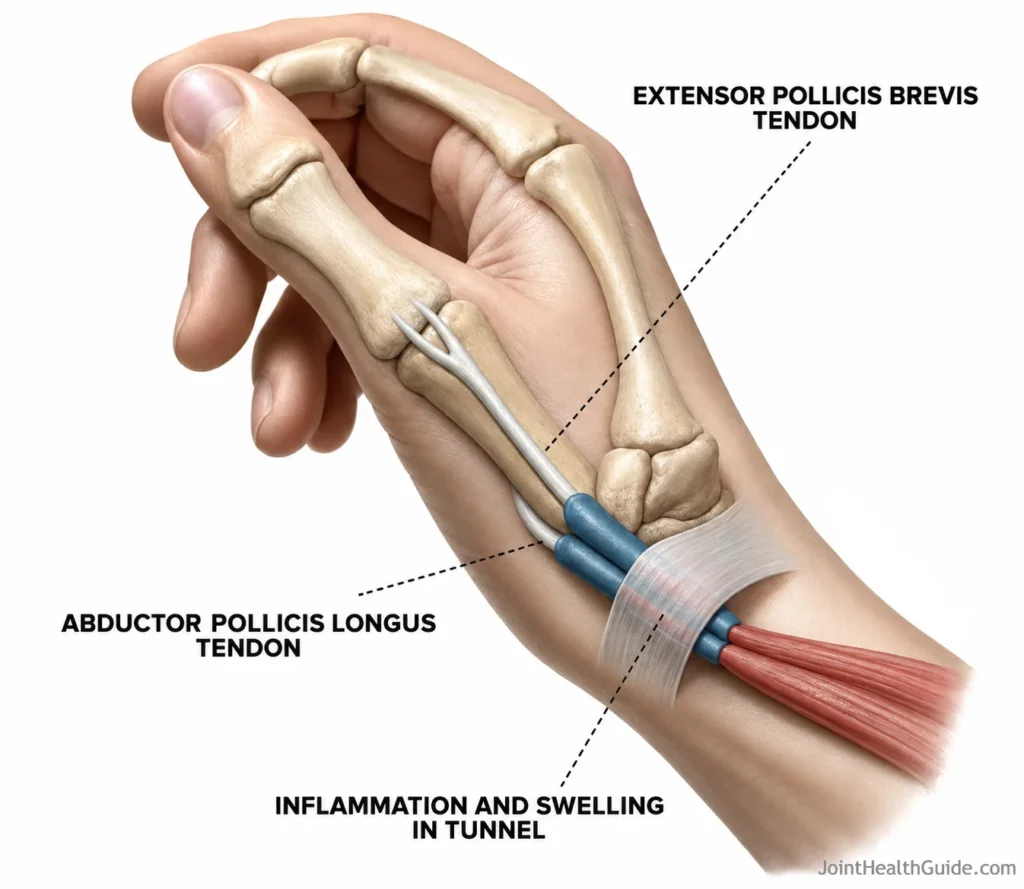
The result is mechanical impingement within the tunnel, where swollen tendons are forced through a tight space. This leads to increased friction within the first dorsal compartment, resulting in tendon irritation and inflammation. As a consequence, patients develop pain on the thumb side of the wrist, reduced thumb motion, and sometimes a catching or “sticking” sensation during wrist and thumb activities.
Risk Factors
Although the exact cause of De Quervain’s tenosynovitis is not fully understood, research shows that it does not develop solely due to overuse of the hand and wrist. Earlier theories linked the condition primarily to repetitive manual work, but newer evidence demonstrates that it occurs equally in people who perform manual labor and those who do not.
The condition is about three times more common in women, especially during pregnancy and the postpartum period, suggesting a possible hormonal influence — particularly the role of estrogen.
Relevant risk factors include:
- Female sex — De Quervain’s tenosynovitis affects approximately 0.5% of adult men and 1.3% of adult women, making it nearly three times more common in women.
- Pregnancy and postpartum period — Frequently seen in the third trimester and in the first months after childbirth, sometimes affecting both wrists. Hormonal changes and repetitive lifting of the baby are believed to contribute.
- Repetitive hand and wrist activities — Activities involving repeated gripping, twisting, pinching, or lifting increase mechanical stress on the APL and EPB tendons. Examples include typing, using tools (e.g., screwdrivers), knitting, gardening, golf, and tennis.
- Underlying medical conditions — Diseases such as diabetes and rheumatoid arthritis are associated with a higher risk of developing radial styloid tenosynovitis.
- Thumb tendonitis history — Previous episodes of tendon irritation or inflammation in the thumb region may predispose individuals to recurrence.
Symptoms of De Quervain’s Tenosynovitis
The primary symptom of De Quervain’s tenosynovitis is pain on the dorsal–radial side of the wrist, near the base of the thumb. The pain usually develops gradually, beginning over the radial styloid and sometimes radiating into the forearm. It intensifies during activities that require gripping, lifting, pinching, or twisting the wrist — for example opening jars, lifting objects, or using tools such as a screwdriver.
Additional symptoms include:
- Localized swelling — Swelling or thickening over the radial styloid, where the APL and EPB tendons pass through the first dorsal compartment.
- Painful thumb movement — Movements involving thumb abduction or extension often provoke sharp discomfort.
- Catching or “sticking” sensation — Some individuals feel snapping, catching, or creaking (crepitus) when moving the thumb.
- Reduced grip strength — Pain and swelling can weaken grip and make lifting or twisting motions difficult.
- Functional limitation — Everyday tasks such as holding a cup, lifting a child, typing, or opening containers may become challenging.

Diagnosis
The diagnosis of De Quervain’s tenosynovitis is based on the patient’s characteristic symptoms and a focused clinical examination. Imaging is used selectively to confirm tendon sheath inflammation or to rule out other causes of radial‑sided wrist pain, such as thumb carpometacarpal osteoarthritis (rhizarthrosis).
Clinical Examination
During the examination, the clinician palpates the dorsal–radial side of the wrist to reproduce symptoms. Pain is typically felt at the base of the thumb and over the radial styloid, sometimes radiating up the forearm. To support the diagnosis, one or more clinical maneuvers may be performed, most commonly the Finkelstein maneuver — often referred to as the De Quervain’s tenosynovitis test.
- Finkelstein test — The patient makes a fist with the thumb tucked inside the fingers. The examiner then gently moves the wrist into ulnar deviation. The test is positive if this movement provokes sharp pain along the dorsal–radial aspect of the wrist, where the APL and EPB tendons run.
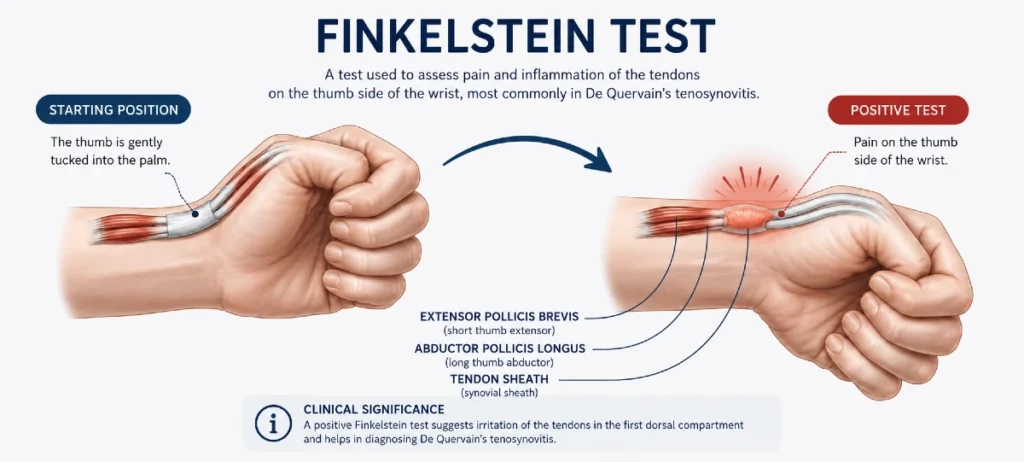
This maneuver stretches the inflamed tendon sheath within the first dorsal compartment, making it a highly sensitive clinical tool for diagnosing radial styloid tenosynovitis.
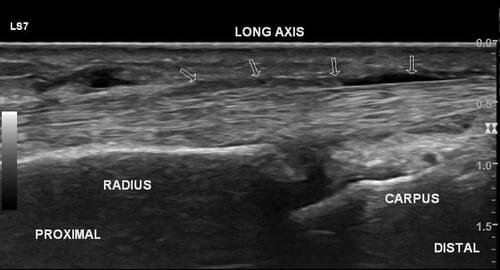
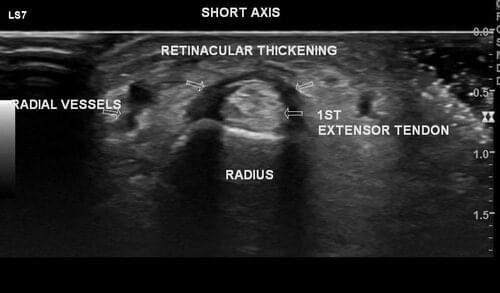
Ultrasound
Ultrasound imaging is the preferred method for confirming tendon sheath inflammation. It can demonstrate:
- Thickening of the APL and EPB tendons
- Fluid accumulation within the tendon sheath
- Thickening of the retinaculum over the first dorsal compartment
- Increased vascularity on Power Doppler in cases of active inflammation
Ultrasound is also valuable for image‑guided corticosteroid injections, ensuring precise delivery into the tendon sheath.
X‑ray
A hand and wrist X‑ray is not required to diagnose De Quervain’s tenosynovitis but may be performed when symptoms resemble other conditions, particularly thumb CMC osteoarthritis (rhizarthrosis) or when trauma is suspected.
Conditions Commonly Confused With De Quervain’s Tenosynovitis
Several disorders can produce radial‑sided wrist pain and may be confused with De Quervain’s tenosynovitis. Recognizing these conditions helps ensure accurate diagnosis and appropriate treatment.
Najčešća stanja koja mogu nalikovati na De Quervainovu bolest uključuju:
- Thumb carpometacarpal osteoarthritis (rhizarthrosis) — Degenerative changes at the base of the thumb cause pain during gripping and pinching, often mistaken for tendon‑related pain.
- Scaphoid fracture — A fracture of the scaphoid bone can present with radial wrist pain and tenderness, especially after trauma.
- Wartenberg’s syndrome — Irritation of the superficial radial nerve leads to burning, tingling, or sharp pain over the dorsal–radial wrist, sometimes resembling tendon inflammation.
- Trigger thumb — Stenosing tenosynovitis of the flexor pollicis longus causes pain and catching in the thumb, but the pain is typically on the volar side, not the dorsal–radial side.
Treatment Options for De Quervain’s Tenosynovitis
The primary goal of treating De Quervain’s tenosynovitis is to reduce inflammation of the tendon sheath, relieve pain, and restore normal thumb and wrist function. Most patients improve with conservative treatment, including activity modification, anti‑inflammatory medication, splinting, physical therapy, and corticosteroid injections. Surgery is reserved for persistent or recurrent cases.
Conservative Treatment
NSAIDs
Non‑steroidal anti‑inflammatory drugs (ibuprofen, naproxen) may be taken orally or applied topically. They help reduce pain and swelling, although medication alone rarely leads to complete resolution.
Activity modification
Avoiding activities that provoke pain — gripping, twisting, lifting, or repetitive thumb movements — allows the irritated tendon sheath to settle.
Thumb Spica Splint (Brace)
A thumb spica splint, often searched as “de Quervain’s tenosynovitis brace”, is one of the most effective early treatments. This brace immobilizes the wrist and thumb, reducing mechanical stress on the APL and EPB tendons.
Key recommendations:
- Wear the brace continuously for 3–4 weeks, day and night
- Remove it only during prescribed exercises
- Immobilization reduces friction and allows the tendon sheath to heal
This is the most important non‑invasive tool for reducing symptoms in the early phase.
Physical Therapy
Physical therapy may include:
- Therapeutic ultrasound
- LASER therapy
- Manual techniques to improve tendon gliding
- Later‑stage strengthening exercises
These interventions help restore mobility and reduce irritation.
Physical therapy alone leads to full recovery in a smaller percentage of patients but is valuable as part of a combined approach.
De Quervain’s Tenosynovitis Injection
A corticosteroid injection is considered the most effective non‑surgical treatment.
The corticosteroid medication is injected directly into the tendon sheath, and the procedure may be performed either “blind” or under ultrasound guidance. Using ultrasound improves accuracy and lowers the risk of accidentally injecting into the tendon itself.
After a single injection, between 65 and 100 percent of patients experience complete relief of symptoms. Wearing a de Quervain’s tenosynovitis brace for three to four weeks after the injection further enhances the treatment effect. If symptoms persist, a second injection can be administered after three to four weeks, while a third injection is generally not recommended if the first two have not produced sufficient improvement.
Surgical Treatment
Surgery is considered when:
- Symptoms do not improve with conservative treatment
- Symptoms recur after two corticosteroid injections
The procedure involves a small incision (≈2 cm) over the radial styloid to expose the first dorsal compartment. The surgeon releases the tendon sheath (extensor retinaculum) to create more space for the APL and EPB tendons. Excess synovial tissue may also be removed.
When performed correctly, surgery reliably relieves symptoms without affecting wrist or thumb function.
Possible complications are rare and may include:
- Local wound infection or delayed healing
- Irritation or injury to the superficial radial nerve
- Tendon instability or snapping if the retinaculum is excessively released
- Hypertrophic or thickened scar formation
Prognosis
The overall prognosis for De Quervain’s tendinitis is very good. Most patients experience full resolution of symptoms with conservative treatment or, when necessary, surgery.
Studies show that 50–80% of patients improve using non‑surgical methods such as splinting, NSAIDs, activity modification, and corticosteroid injection. Those who do not respond adequately to conservative therapy typically achieve excellent outcomes after surgical release of the first dorsal compartment.
Long‑term recurrence is uncommon when the underlying inflammation is resolved and proper rehabilitation is followed.
Conclusion
De Quervain’s tenosynovitis is a common and treatable cause of dorsal–radial‑sided wrist pain. With early recognition, appropriate rest, use of a brace, and targeted exercises, symptoms may improve in milder cases. Corticosteroid injections remain the most effective non‑surgical treatment option for De Quervain’s tenosynovitis.
Surgery is reserved for persistent or recurrent cases and generally provides excellent results. A structured rehabilitation plan and avoidance of repetitive strain help prevent recurrence and support full return to daily activities.
FAQ (Frequently Asked Questions)
What causes De Quervain’s tenosynovitis?
The condition develops due to irritation and thickening of the tendon sheath around the APL and EPB tendons. It is often associated with repetitive thumb and wrist movements, hormonal influences (especially in pregnancy and postpartum), and sometimes underlying conditions such as diabetes or rheumatoid arthritis.
How is De Quervain’s tenosynovitis diagnosed?
Diagnosis is based on clinical symptoms, physical examination, and the Finkelstein maneuver, which provokes pain on the dorsal–radial side of the wrist. Ultrasound can confirm tendon sheath inflammation.
What is the most effective treatment?
Many patients improve with splinting, NSAIDs, and activity modification, but the highest success rate is achieved with a corticosteroid injection.
How long does recovery take?
Mild cases improve within a few weeks. After a corticosteroid injection, relief is often rapid. Post‑surgical recovery typically takes several weeks, followed by gradual return to full activity.
Can exercises help?
Yes. Once pain decreases, gentle stretching and strengthening exercises improve tendon mobility and reduce recurrence risk.
When is surgery needed?
Surgery is considered when symptoms persist despite conservative treatment or recur after two corticosteroid injections. Surgical release of the first dorsal compartment usually provides excellent long‑term results.
Ferrara PE, Codazza S, Cerulli S, Maccauro G, Ferriero G, Ronconi G. Physical modalities for the conservative treatment of wrist and hand’s tenosynovitis: A systematic review. Semin Arthritis Rheum. 2020 Dec;50(6):1280–1290. doi: 10.1016/j.semarthrit.2020.08.006. Epub 2020 Aug 29. PMID: 33065423. Systematic review: Physical therapy modalities for wrist and hand tenosynovitis
Challoumas D, Ramasubbu R, Rooney E, Seymour‑Jackson E, Putti A, Millar NL. Management of De Quervain Tenosynovitis: A Systematic Review and Network Meta‑Analysis. JAMA Netw Open. 2023 Oct 2;6(10):e2337001. doi: 10.1001/jamanetworkopen.2023.37001. PMID: 37889490; PMCID: PMC10611995. Evidence synthesis: Comparative effectiveness of treatments for De Quervain’s tenosynovitis
Fakoya AO, Tarzian M, Sabater EL, Burgos DM, Maldonado Marty GI. De Quervain’s Disease: A Discourse on Etiology, Diagnosis, and Treatment. Cureus. 2023 Apr 24;15(4):e38079. doi: 10.7759/cureus.38079. PMID: 37252462; PMCID: PMC10208847. Comprehensive review: Etiology, diagnosis, and management of De Quervain’s disease
Satteson E, Tannan SC. De Quervain Tenosynovitis. [Updated 2023 Nov 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan–. Clinical overview: Pathophysiology and treatment of De Quervain’s tenosynovitis

















