

Heel spurs are small bony growths that develop on the calcaneus (heel bone) as a result of chronic traction and micro‑stress at tendon or fascia attachment sites. They are extremely common findings on X‑ray, and in most cases they do not cause any symptoms. Many adults discover a heel spur incidentally during imaging performed for unrelated reasons.
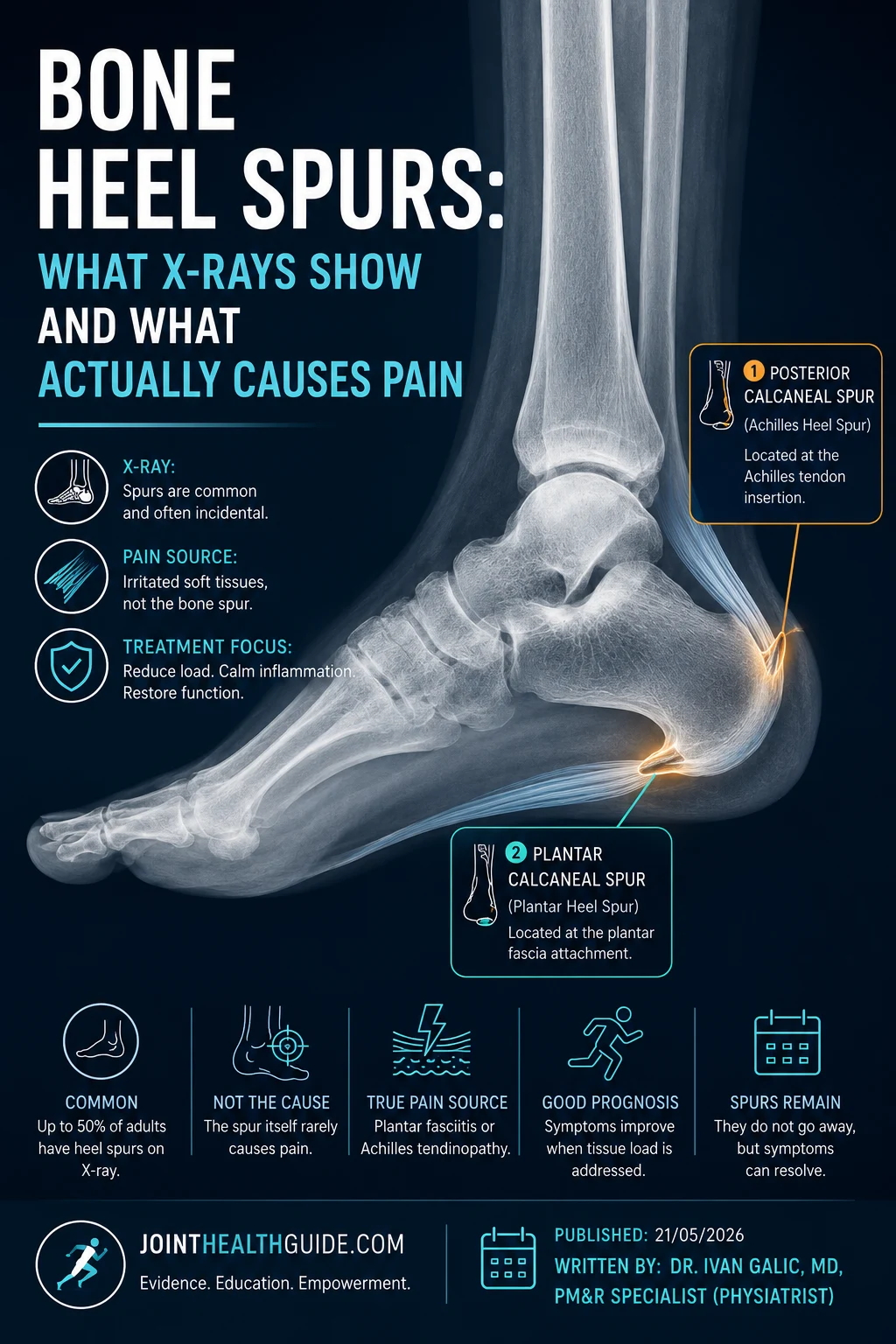
Two main types are clinically relevant: the plantar heel spur, located on the underside of the heel, and the Achilles heel spur, found at the back of the heel where the Achilles tendon inserts. Although both develop through similar adaptive mechanisms, their clinical presentation and treatment differ.
Understanding the difference between these two types of heel spurs — and when they actually matter clinically — is essential for accurate diagnosis and effective treatment planning.
Quick Overview – Bone Heel Spurs
- Bone heel spurs (calcaneal enthesophytes) are bony projections that form at the plantar fascia or Achilles tendon insertion due to long‑term traction and micro‑stress.
- Most heel spurs are asymptomatic and discovered incidentally on X‑ray; the spur itself is rarely the true source of heel pain.
- Symptoms typically arise from soft‑tissue irritation such as plantar fasciitis or insertional Achilles tendinopathy, not from the spur.
- X‑ray is the most accurate method for detecting heel spurs, while ultrasound is best for assessing associated soft‑tissue pathology.
- Treatment focuses on reducing soft‑tissue overload, calming local irritation, and minimizing direct heel pressure rather than attempting to remove or shrink the spur.
- Heel spurs do not regress and may enlarge with age, but their size is not correlated with symptom severity; long‑term prognosis is excellent once soft‑tissue overload is addressed.
What Are Bone Heel Spurs?
Bone heel spurs — medically known as calcaneal enthesophytes — are small, pointed bony projections that form on the calcaneus (heel bone) at the attachment sites of the plantar fascia or the Achilles tendon. They develop gradually as an adaptive response to long‑term mechanical stress — a combination of traction forces, micro‑tears, and low‑grade inflammation at the enthesis (the point where soft tissue meets bone).
There are two clinically distinct types of heel spurs:
- Plantar calcaneal spur — located on the underside of the heel, where the plantar fascia attaches. These spurs may be associated with plantar fasciitis, but the spur itself is rarely the true cause of pain.
- Achilles heel spur — located at the back of the heel, near the insertion of the Achilles tendon. These spurs are more likely to contribute to symptoms when combined with insertional Achilles tendinopathy.

Understanding the difference between these two types — and when they actually matter clinically — is essential before diving into symptoms, diagnosis, and treatment.
Why Heel Spurs Develop
Bone heel spurs (calcaneal enthesophytes) form as a long‑term adaptive response to repetitive mechanical loading at the enthesis, the point where tendons or fascia attach to the calcaneus. When these structures are exposed to chronic traction, micro‑stress, or reduced tissue elasticity, the body responds by depositing new bone to reinforce the area. This slow remodeling process can eventually create a bony projection – bone spur.
The development of both plantar and posterior heel spurs follows the same principle: Repeated pulling forces + micro‑damage at the attachment site → adaptive bone formation.
Risk Factors for Developing Heel Bone Spurs
Factors that increase repetitive traction and mechanical stress at the heel’s soft‑tissue attachment sites also increase the likelihood of developing calcaneal enthesophytes.
- Age 40+ — natural stiffening of fascia and tendons increases traction forces
- Obesity — higher mechanical load on the heel during standing and walking
- Foot deformities — flat feet, high arches, overpronation
- Reduced calf flexibility — increases tension on both the plantar fascia and Achilles tendon
- Prolonged standing — especially on hard surfaces
- High‑impact activities — running, jumping, sudden directional changes
- Inadequate footwear — poor cushioning or rigid soles
- Previous heel or foot injuries — altered biomechanics increase enthesis stress
Plantar Calcaneal Spur (Plantar Calcaneal Enthesophyte)
A plantar heel spur, or plantar calcaneal enthesophyte, is a bony projection that forms on the underside of the calcaneus at the attachment of the plantar fascia. It is extremely common in adults and is found incidentally on X‑ray in a large portion of the population. Studies show that up to 45–55% of adults with heel X‑rays have a plantar spur, yet the majority are completely asymptomatic. In fact, research indicates that only about 5–10% of plantar heel spurs are directly associated with pain.

When symptoms do occur, they typically include localized pain at the bottom of the heel, discomfort during the first steps in the morning, and tenderness when pressing directly over the spur region. However, in most cases, the spur itself is not the true generator of pain — it is simply a structural adaptation.
Achilles Heel Spur (Posterior Calcaneal Enthesophyte)
An Achilles heel spur, or posterior calcaneal enthesophyte, forms at the back of the calcaneus where the Achilles tendon inserts. It is less common than the plantar variant but still frequently seen on imaging, especially in middle‑aged and older adults.
Like plantar spurs, most posterior enthesophytes are asymptomatic, though they are more likely to become clinically relevant when combined with tendon irritation. Estimates suggest that only 10–20% of Achilles heel spurs are associated with symptoms.
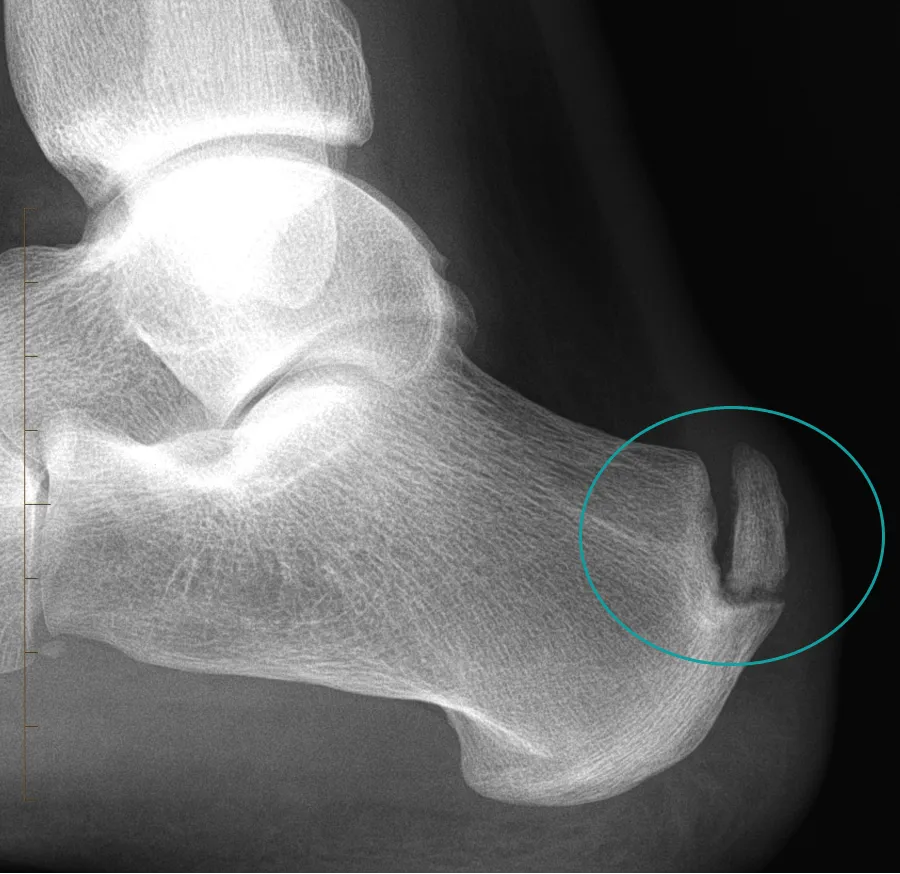
These spurs develop through the same mechanism: chronic traction and mechanical stress at the tendon insertion stimulate bone formation over time. When symptomatic, patients may experience pain at the back of the heel, discomfort when wearing rigid shoes, and tenderness directly over the bony prominence. Symptoms often worsen during activities that load the Achilles tendon, such as walking uphill or pushing off during running.
Diagnosis of Heel Bone Spurs
Heel bone spurs — calcaneal enthesophytes — are diagnosed primarily with imaging. Since most are asymptomatic, the goal is to confirm their presence and assess nearby soft tissues that may actually be causing pain.
- X‑ray — first‑line and most accurate for detecting both plantar and posterior heel spurs; clearly shows size and shape of the enthesophyte.
- Ultrasound — not reliable for visualizing plantar heel spurs, but excellent for posterior (Achilles) spurs; best tool for assessing plantar fasciitis or Achilles tendinopathy.
- MRI — rarely needed; used only for atypical heel pain, suspected stress fracture, or complex soft‑tissue pathology.
When Heel Bone Spurs Actually Matter Clinically
Most heel spurs do not cause pain. They are structural adaptations to long‑term mechanical loading and are frequently discovered incidentally on X‑ray in people who have no heel symptoms at all. This is why the presence of a spur alone is not enough to explain heel pain.
Heel spurs become clinically relevant only when they are associated with irritation of nearby soft tissues, such as the plantar fascia or the Achilles tendon. In these cases, the spur is not the primary problem but may contribute to local pressure, inflammation, or mechanical conflict during movement.
- Most heel spurs are asymptomatic — the spur itself rarely generates pain
- Symptomatic cases are uncommon — pain usually arises from soft‑tissue overload, not the bone spur
- Incidental finding vs true cause — a spur on X‑ray does not automatically explain heel pain; clinical correlation is essential
- When symptoms occur — localized tenderness, pain with first steps, discomfort with pressure from footwear, or pain during activities that load the heel
Treatment of Heel Spurs
Calcaneal enthesophytes — are not treated directly, because the spur itself cannot be reduced or removed with conservative therapy. As the heel spur itself is not the source of pain but irritation of surrounding soft tissues, treatment focuses on reducing overload, calming inflammation, and minimizing direct heel pressure.
- We do not treat the spur itself — bone cannot be “shrunk” with exercises, medications, or therapy
- We treat the irritated soft tissues — such as plantar fasciitis or insertional Achilles tendinopathy
- We reduce repetitive traction — by improving flexibility, biomechanics, and load distribution
- We reduce direct pressure on the heel — through footwear modifications or cushioning to offload the enthesis
- We address contributing factors — such as calf tightness, poor footwear, or excessive impact loading
Once the surrounding tissues calm down and mechanical stress is reduced, the heel spur becomes clinically irrelevant, even though it remains visible on imaging.
Prognosis & Recovery
Bone heel spurs are long‑term structural adaptations, and once formed, they do not disappear. Over the years they may slowly increase in size, especially if repetitive traction and mechanical stress persist. As we know, the presence of a spur is usually not related to symptoms, and its size is not proportional to the severity of pain.
Most people with heel spurs remain completely asymptomatic, and even in symptomatic cases, recovery depends on calming the irritated soft tissues (plantar fascia or Achilles tendon), not on changing the spur itself. When the surrounding tissues heal and mechanical load is optimized, the spur becomes clinically irrelevant, even though it remains visible on imaging.
- Heel spurs do not regress — they may slowly enlarge with age
- Spur size does not predict symptoms — large spurs can be painless; small spurs can coexist with soft‑tissue irritation
- Symptoms improve by treating soft tissues — not by targeting the spur itself
- Long‑term outlook is excellent — most patients recover fully once overload is addressed
FAQ
Do heel spurs cause pain?
Most heel spurs do not cause pain. They are usually incidental findings on X‑ray, and symptoms—when present—come from irritated soft tissues (plantar fascia or Achilles tendon), not from the spur itself.
Can heel spurs go away?
No. Heel spurs do not regress. Once formed, they remain permanently and may slowly enlarge with age. Symptoms, however, can fully resolve because pain is not caused by the spur.
Do I need surgery?
Almost never. Surgery for heel spurs is rarely indicated because the spur is not the pain generator. Treatment targets soft‑tissue irritation, and most patients recover without any surgical intervention.
Are heel spurs dangerous?
No. Heel spurs are not dangerous. They are benign bony adaptations and only matter clinically if nearby tissues become irritated.
Can I exercise with a heel spur?
Yes. Exercising with a heel spur is usually safe as long as activities do not aggravate symptoms. Since the spur itself is not the source of pain, exercise is typically guided by comfort and soft‑tissue tolerance.
Summary
Heel spurs — calcaneal enthesophytes — are common, benign bony projections that form due to long‑term repetitive traction at the enthesis. They do not disappear over time, but their presence is usually not related to symptoms, and spur size does not correlate with pain intensity. The key clinical distinction is between:
- Plantar heel spurs — located on the underside of the heel, often incidental, rarely symptomatic
- Achilles heel spurs — located at the back of the heel, occasionally symptomatic when combined with tendon irritation
In both cases, symptoms arise from soft‑tissue overload, not from the spur itself. With proper management of plantar fasciitis or insertional Achilles tendinopathy, patients typically recover fully while the spur remains clinically irrelevant.
Velagala VR, Velagala NR, Kumar T, Singh A, Mehendale AM. Calcaneal Spurs: A Potentially Debilitating Disorder. Cureus. 2022 Aug 28;14(8):e28497. DOI: Calcaneal spur pathology and clinical overview
Allam AE, Chang KV. Plantar Heel Pain. StatPearls [Internet]. Updated 2024 Jan 4. Clinical review: diagnosis and management of plantar heel pain
Mohseni M, Mousavi E, Alebouyeh MR. Key Considerations When Targeting a Heel Spur. Anesth Pain Med. 2023 Oct 1;13(5):e139326. DOI: Clinical considerations in heel spur interventions
Kirkpatrick J, Yassaie O, Mirjalili SA. The plantar calcaneal spur: a review of anatomy, histology, etiology and key associations. J Anat. 2017 Jun;230(6):743–751. Wiley: Anatomy and pathology of plantar calcaneal spur

















