

Carpal tunnel syndrome is a compressive neuropathy caused by pressure on the median nerve as it passes through the narrow carpal tunnel in the wrist. It is by far the most common entrapment neuropathy, accounting for nearly 90% of all nerve compression syndromes. The condition typically appears between the ages of 40 and 60, and women are affected up to ten times more often than men.
The hallmark symptoms include pain, tingling, numbness, and paresthesias in the hand — especially in the thumb, index, and middle finger. Symptoms often worsen at night, disrupting sleep and daily functioning. If left untreated, carpal tunnel syndrome can lead to permanent nerve damage, muscle weakness, and long‑term loss of hand function.
This guide will help you understand what carpal tunnel syndrome is, why it develops, how to recognize its symptoms early, and which treatment and prevention strategies can reduce your risk and protect long‑term hand health.
Key Clinical Points – Carpal Tunnel Syndrome (CTS)
- Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy, caused by compression of the median nerve at the wrist.
- Typical symptoms include numbness, tingling, night-time pain, and reduced fine motor control in the thumb, index, and middle fingers.
- Nearly 90% of patients with mild to moderate CTS respond well to conservative treatment such as splinting, activity modification, physiotherapy, and corticosteroid injections.
- Progressive or long-standing compression may lead to permanent nerve damage, weakness of thumb opposition, and thenar muscle atrophy.
- Electrodiagnostic testing (EMNG) is essential for assessing severity and identifying patients at risk of irreversible nerve injury.
- Surgical decompression (open or endoscopic) is indicated when conservative treatment fails or when severe nerve damage is present.
- Carpal tunnel release has an initial success rate of over 90%, though symptoms may recur in a subset of patients over time.
- Recovery typically takes weeks to months, with sensory improvement depending on the degree of preoperative nerve damage.
- CTS can be bilateral, especially in patients with systemic conditions such as diabetes, hypothyroidism, rheumatoid arthritis, or pregnancy.
What Is the Carpal Tunnel? Anatomy and the Role of the Median Nerve
The carpal tunnel is a narrow, rigid passageway located on the palm side of the wrist. To understand why carpal tunnel syndrome develops, it helps to first understand the structure of this tunnel and the function of the median nerve that passes through it.
Carpal Tunnel Anatomy
The carpal tunnel is formed by two key anatomical components:
- The floor and walls — made of the carpal bones, arranged in a curved, bowl‑like shape.
- The roof — a strong fibrous band called the transverse carpal ligament (flexor retinaculum), which closes the tunnel from above.
Through this tight space pass:
- Nine flexor tendons responsible for bending the fingers
- The median nerve, which is particularly vulnerable because it shares limited space with the tendons
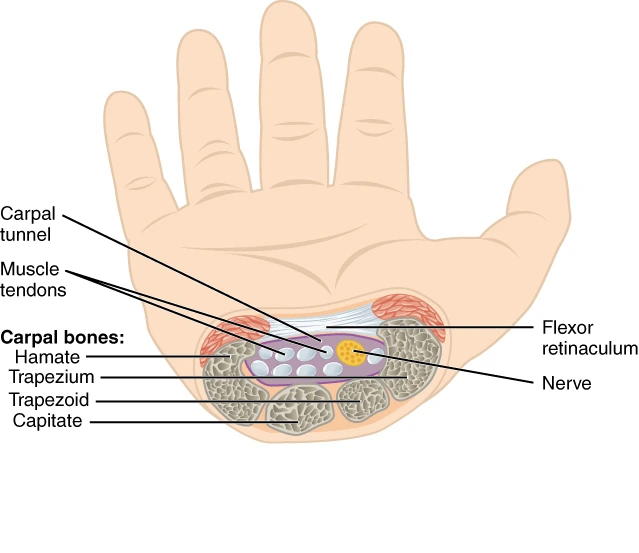
Because the tunnel is rigid and cannot expand, any swelling of the tendons or thickening of the ligament increases pressure inside the tunnel. This is the core mechanism behind median nerve compression.
During surgical treatment of carpal tunnel syndrome, the transverse carpal ligament is released to reduce pressure and create more space for the nerve.
Function of the Median Nerve
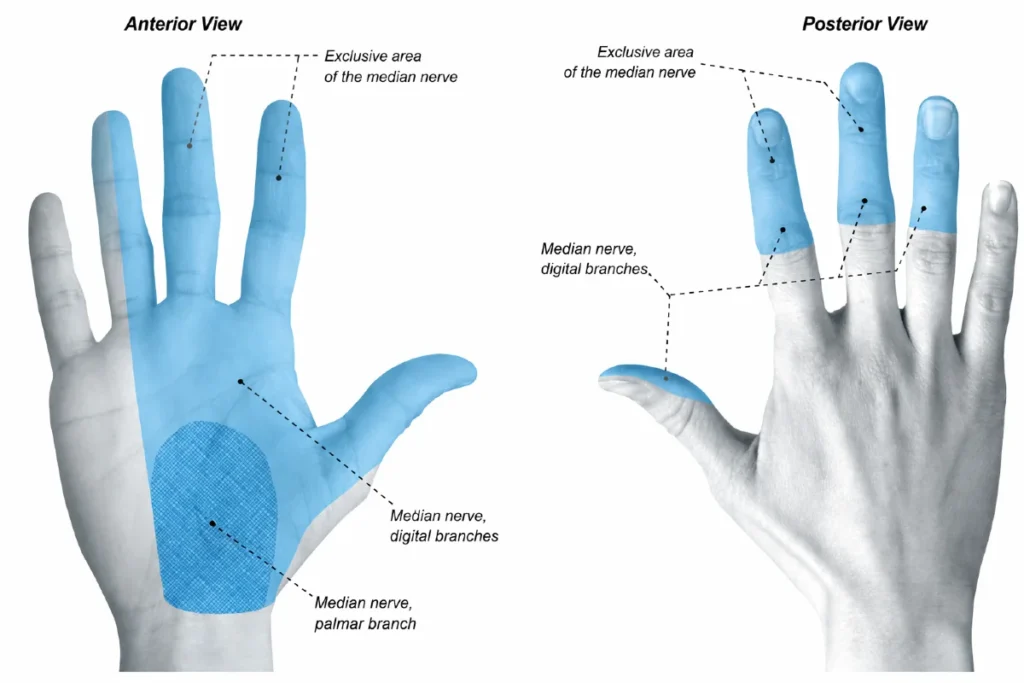
The median nerve is essential for both sensation and motor control in the hand. It provides:
- Sensation to the thumb, index finger, middle finger, and half of the ring finger
- Motor supply to several important hand muscles, especially those at the base of the thumb (thenar muscles), enabling fine movements like pinching, gripping, and precision tasks
When the median nerve is compressed, these sensory and motor functions become impaired, leading to the classic symptoms of numbness, tingling, pain, and reduced thumb strength.
What Is Carpal Tunnel Syndrome (CTS)?
When people search what is carpal tunnel syndrome, they are usually looking for a clear explanation of why pain, tingling, or numbness appear in the hand. Carpal tunnel syndrome (CTS) — the medical abbreviation commonly used in clinical practice — refers to a condition in which the median nerve becomes compressed as it passes through the narrow carpal tunnel in the wrist.
CTS develops when the space inside the tunnel becomes too tight for the structures that pass through it, most notably the median nerve and the flexor tendons. Because the tunnel is rigid and cannot expand, even mild swelling or thickening of surrounding tissues can increase pressure on the nerve. This pressure leads to the characteristic symptoms: numbness, tingling, pain, and reduced thumb strength.
Understanding what carpal tunnel syndrome is provides the foundation for recognizing early warning signs and choosing the right treatment strategies before long‑term nerve damage occurs.
What Causes Carpal Tunnel Syndrome?
Carpal tunnel syndrome occurs when the pressure inside the carpal tunnel rises above what the median nerve can tolerate. Because the tunnel is a rigid anatomical space — formed by carpal bones below and the transverse carpal ligament above — it cannot stretch or expand when additional volume appears inside it. Even small changes in the structures within the tunnel can disrupt the delicate balance between available space and the tissues that occupy it.
When the pressure increases, the median nerve’s blood supply becomes compromised, leading to nerve swelling, impaired conduction, and the characteristic symptoms of CTS. The mechanism is similar to stepping on a garden hose: once compressed, the flow is disrupted and the system stops functioning normally.
Common Mechanisms That Increase Pressure in the Carpal Tunnel
- Previous wrist fractures or poorly healed injuries can alter the shape of the carpal tunnel and reduce available space.
- Advanced degenerative changes of the wrist, including osteophyte formation, may mechanically narrow the tunnel.
- Inflammatory arthritides, such as rheumatoid arthritis, can cause swelling of the joint capsule and flexor tendons.
- Systemic conditions like obesity, diabetes, and thyroid dysfunction often lead to soft‑tissue swelling and fluid retention within the wrist.
- Hormonal changes during pregnancy or menopause can increase fluid accumulation, raising tunnel pressure.
- Repetitive wrist movements — typing, assembly‑line work, tool use — may irritate the flexor tendons and cause thickening or inflammation.
- Prolonged exposure to vibration, especially from power tools, can impair microcirculation of the nerve and contribute to chronic irritation.
- Space‑occupying lesions such as ganglion cysts or tumors are less common but can directly compress the nerve.
In many patients, multiple factors act together, gradually increasing pressure until the median nerve becomes symptomatic.
Carpal Tunnel Symptoms
Understanding carpal tunnel symptoms is essential for recognizing the condition early and preventing long‑term nerve damage. Many people search what does carpal tunnel feel like or where does carpal tunnel hurt because the symptoms can be confusing at first — they may come and go, appear only at night, or feel like they are coming from the fingers rather than the wrist.
What Does Carpal Tunnel Feel Like?
The earliest signs are usually tingling, pins‑and‑needles sensations, and intermittent numbness in the fingers supplied by the median nerve — the thumb, index finger, middle finger, and half of the ring finger. Patients often describe the feeling as “electric,” “buzzing,” or “ants crawling under the skin.”
These sensations are typically worse at night, often waking people from sleep. Many instinctively shake or flick the hand to relieve the discomfort, which temporarily improves symptoms by restoring blood flow to the compressed nerve.
Where Does Carpal Tunnel Hurt?
Carpal tunnel pain can be felt:
- in the wrist, especially on the palm side
- radiating into the hand and fingers
- occasionally traveling up the forearm toward the elbow
The pain is usually linked to activities that increase pressure in the carpal tunnel — gripping, typing, repetitive wrist flexion, or using vibrating tools.
Progression of Symptoms
As compression of the median nerve worsens, symptoms become more persistent:
- Daytime symptoms begin to appear, often triggered by specific tasks
- Weakness in the hand develops, especially when pinching or gripping
- Patients may notice dropping objects or difficulty with fine motor tasks
- Some experience a false sensation of swelling in the fingers, even though no visible swelling is present
In advanced stages, long‑standing nerve compression can lead to:
- Atrophy of the thenar muscles (the muscles at the base of the thumb)
- Permanent sensory loss in the affected fingers
- Marked loss of thumb strength and dexterity
Recognizing these symptoms early is crucial, as timely evaluation by a healthcare professional can prevent irreversible nerve damage.
Diseases That Can Mimic Carpal Tunnel Syndrome
Although carpal tunnel syndrome (CTS) primarily affects the hand and wrist, its symptoms can sometimes radiate up the arm toward the elbow, creating confusion with other conditions. Understanding these differential diagnoses is crucial for accurate evaluation and treatment.
Conditions That May Resemble CTS
- Degenerative cervical spine disease — wear‑and‑tear changes in the neck can irritate nerve roots, producing pain, tingling, or numbness that may extend down the arm, similar to CTS.
- Myofascial pain syndrome of the upper back and neck — trigger points in shoulder or neck muscles can cause referred pain and paresthesias in the hand, mimicking nerve compression.
- Cervical radiculopathy or spinal cord compression — pressure on cervical nerve roots can lead to sensory disturbances and weakness in the same distribution as the median nerve.
- Inflammatory or degenerative tendon disorders — conditions such as De Quervain’s tenosynovitis or thumb base osteoarthritis (rhizarthrosis) may cause localized wrist pain and functional limitation that resemble CTS.
Because these disorders can overlap in symptoms, clinical examination and diagnostic testing (such as nerve conduction studies or imaging) are essential to distinguish true carpal tunnel syndrome from other causes of hand and wrist pain.
Diagnosis of Carpal Tunnel Syndrome
If you suspect you may have carpal tunnel syndrome, it’s important to consult a qualified healthcare professional for timely evaluation and treatment. The diagnosis is based on a careful assessment of symptoms, a targeted physical examination, and specific diagnostic tests. There are no blood tests that can confirm CTS.
Clinical Examination — Carpal Tunnel Syndrome Tests
During the physical examination, clinicians look for characteristic signs of carpal tunnel that indicate impaired median nerve function. Beyond provocative maneuvers, a focused neurological assessment of the hand is essential.
Sensory Findings
- Hypoesthesia in the first three fingers — reduced sensation in the thumb, index finger, and middle finger (and the radial half of the ring finger) is a classic indicator of median nerve involvement.
- Patients often describe the sensation as “dull,” “reduced,” or “as if the fingers are wrapped in cotton.”
Motor Findings
In more advanced cases, motor deficits become visible:
- Thenar atrophy — wasting of the muscles at the base of the thumb, reflecting long‑standing denervation.
- Weakness of thumb opposition — difficulty bringing the thumb across the palm to touch the fingertips, which affects precision grip and fine motor tasks.
- Reduced pinch and grip strength — a consequence of impaired thenar muscle function.
Provocative Tests (Carpal Tunnel Syndrome Tests)
- Tinel’s Sign — tapping over the median nerve at the wrist elicits tingling in the median‑innervated fingers.
- Phalen’s Test — holding the wrists in flexion for 30–60 seconds provokes paresthesias.
- Durkan’s Compression Test — direct pressure over the median nerve just below the wrist crease triggers symptoms within 30 seconds.
These findings, combined with patient history and diagnostic studies, form the foundation for confirming carpal tunnel syndrome
Imaging and Electrophysiological Studies
- Ultrasound — a quick, accessible test that can visualize nerve swelling and identify possible causes of compression. It also allows dynamic assessment of nerve movement during finger motion. In some cases, the nerve may appear “stuck” to the transverse ligament, limiting its mobility.
- Electromyoneurography (EMNG) — a diagnostic study that measures electrical activity in muscles and nerve conduction velocity. EMNG is considered essential for confirming CTS and assessing the degree of nerve damage, which helps guide treatment planning.
Together, these tests provide a comprehensive picture of carpal tunnel syndrome, ensuring accurate diagnosis and appropriate management.
Clinical Insight
Accurate diagnosis of carpal tunnel syndrome relies on a combination of clinical findings and electrodiagnostic testing. Early identification of nerve impairment is essential to prevent long‑term functional deficits.
Carpal Tunnel Treatment
Effective carpal tunnel treatment depends on the severity of median nerve compression and the patient’s individual needs. Treatment options fall into two main categories:
- Conservative (non‑surgical) treatment
- Surgical treatment — covered in the next chapter
Conservative therapy is recommended as the first‑line approach whenever there is no evidence of severe or advanced nerve damage.
Preventive and Lifestyle Measures
Preventive strategies aim to reduce mechanical stress on the median nerve and are often the first step in carpal tunnel treatment without surgery:
- Adjusting wrist position during work and daily activities
- Improving workstation ergonomics (e.g., correct keyboard height to avoid excessive wrist flexion)
- Using soft silicone wrist supports for the mouse
- Reducing repetitive wrist‑intensive tasks when possible
- Weight reduction and increased physical activity when appropriate
These measures help minimize symptom flare‑ups and slow disease progression.
Wrist Splints / Carpal Tunnel Braces
WWrist splints (orthoses) are commonly used in the early stages of carpal tunnel syndrome, especially when symptoms are most noticeable at night.
- Their primary role is to keep the wrist in a neutral position during sleep, preventing excessive flexion or extension that increases pressure in the carpal tunnel
- They are most effective for reducing night‑time numbness, tingling, and pain
- They do not reverse nerve damage and are not highly effective for persistent daytime symptoms
- Symptom improvement usually requires several weeks of regular night‑time use
- They can help patients sleep better and reduce nocturnal symptom flare‑ups
Splints are therefore a supportive measure, not a definitive treatment, and their benefit is mainly limited to night‑time symptom control in mild cases.
Physical Therapy and Carpal Tunnel Exercises
Physical therapy plays a key role in relieving symptoms and improving function. Common modalities include:
- LASER therapy
- Therapeutic ultrasound
- Magnetotherapy
- Electrical stimulation
In addition, carpal tunnel exercises are used to:
- Improve wrist mobility
- Stretch tight soft tissues
- Enhance median nerve gliding
Some patients benefit from nerve‑gliding exercises, which help the median nerve move more freely and reduce adhesions to surrounding structures.
Injection Techniques
Local corticosteroid injections are an effective option for many patients and can significantly reduce carpal tunnel pain.
- Injected directly into the carpal tunnel
- Ideally performed under ultrasound guidance for accuracy and safety
- Corticosteroids reduce inflammation and nerve swelling
- When performed correctly, injections are safe and effective
Duration of Effect
- In early or mild cases: long‑term relief is possible
- In moderate to severe cases: improvement is often temporary
- Average duration: around one year, sometimes longer
- Can be repeated safely up to three times per year
Injections are especially useful for patients who are not yet candidates for surgery or who need temporary relief.
| Method | Advantages | Limitations |
|---|---|---|
| Wrist Splint (Night Brace) | Reduces night-time symptoms; keeps wrist in neutral position; non-invasive | Limited effect on daytime symptoms; does not reverse nerve damage; requires weeks of use |
| Physical Therapy & Exercises | Improves mobility; reduces soft-tissue tension; may enhance nerve gliding | Effect varies; requires regular sessions; slower onset of improvement |
| Nerve-Gliding Exercises | Improves median nerve mobility; helpful when adhesions are present | Not effective in severe compression; requires proper technique |
| Corticosteroid Injection | Fast symptom relief; reduces inflammation and nerve swelling; ultrasound guidance increases safety | Effect often temporary in moderate–severe cases; limited to several injections per year |
Carpal Tunnel Syndrome – When Is Surgery Necessary?
Surgical treatment becomes necessary when conservative measures no longer provide adequate relief or when diagnostic findings indicate advanced median nerve compression. In these situations, delaying treatment may increase the risk of permanent nerve damage, progressive weakness of thumb opposition, and visible thenar atrophy.
In clinical practice, surgery is considered when patients present with:
- Persistent symptoms despite properly conducted conservative therapy
- Progressive weakness of thumb opposition
- Visible thenar muscle atrophy
- Severe EMNG findings indicating significant nerve compression
The surgical procedure, known as carpal tunnel release, is typically performed by a hand surgeon or plastic surgeon. The goal is straightforward: to cut the transverse carpal ligament (flexor retinaculum), thereby increasing the available space within the carpal tunnel and reducing pressure on the median nerve. Most procedures are performed as outpatient surgeries, under either local anesthesia (numbing the hand and forearm) or general anesthesia.
Surgical Techniques
Although two different techniques exist, both aim to achieve the same outcome — safe and effective decompression of the median nerve.
Open Carpal Tunnel Release (Classic Approach)
In the open technique, the surgeon makes a small incision in the palm, allowing direct visualization of the carpal tunnel structures.
During the procedure:
- The transverse carpal ligament is carefully cut
- The space within the tunnel increases immediately
- Pressure on the median nerve is reduced
Over time, the ligament heals in a lengthened configuration, ensuring that the tunnel remains more spacious and the nerve remains decompressed.
Endoscopic Carpal Tunnel Release
The endoscopic technique involves one or two small skin incisions (portals) through which a miniature camera is inserted. The surgeon visualizes the inside of the wrist on a screen and uses a specialized instrument to cut the transverse carpal ligament.
Potential advantages include:
- Smaller skin incisions
- Faster recovery of soft tissues
- Less postoperative discomfort in the early days
However, in the long term, both techniques have equivalent success rates.
Outcomes and Long‑Term Results
Regardless of the technique used, carpal tunnel release is considered a highly successful procedure:
- Initial success rates exceed 90%
- Complications are rare when performed by an experienced surgeon
- Most patients experience significant symptom relief within days or weeks
Still, it is important to note that approximately one‑third of patients may experience some recurrence of symptoms over several years. This can be related to:
- Scar tissue formation
- Incomplete release of the ligament
- Progression of underlying conditions such as diabetes or arthritis
Because both surgical methods are effective, the choice of technique typically depends on:
- The surgeon’s experience and preference
- The patient’s anatomy and medical history
- Functional demands and expectations regarding recovery time
Recovery After Carpal Tunnel Surgery
Recovery after carpal tunnel release varies from person to person, influenced by factors such as the severity of nerve compression, the type of surgical technique, overall health, and how consistently the patient follows postoperative instructions. Although individual experiences differ, most patients can expect a recovery period ranging from several weeks to a few months.
In the first few days, it is normal to experience:
- Pain and soreness around the incision
- Swelling of the hand and fingers
- Reduced mobility of the wrist and thumb
During this early phase, simple measures such as ice application, keeping the hand elevated, and avoiding heavy gripping can significantly reduce discomfort and swelling.
Early Recovery (First 2–3 Weeks)
As the initial inflammation subsides, patients gradually regain comfort and mobility. Stitches are typically removed within the first two weeks, depending on the surgeon’s protocol. Light daily activities are usually allowed, but forceful gripping, lifting, or repetitive wrist movements should still be avoided.
Around 2–3 weeks after surgery, most patients begin physical therapy or guided home exercises. The goals at this stage include:
- Restoring wrist and finger range of motion
- Improving flexibility of the soft tissues
- Preventing scar adhesions
- Gradually strengthening the hand and thumb muscles
Therapy is especially important for patients who had significant preoperative symptoms, stiffness, or thenar weakness.
Progressive Improvement (Weeks to Months)
As healing continues, most patients notice:
- Reduction of numbness and tingling
- Improved grip and pinch strength
- Better hand coordination
- Return to normal daily activities
Full recovery of strength may take several months, especially in cases where the median nerve was severely compressed before surgery. Patients with long‑standing symptoms or marked thenar atrophy may experience slower or incomplete recovery, although most still benefit from significant symptom relief.
Long‑Term Outlook
For the majority of patients, carpal tunnel surgery provides:
- Lasting reduction of pain and paresthesias
- Improved hand function
- Better sleep due to the absence of night‑time symptoms
However, recovery is not instantaneous — it is a gradual process
Disease Progression and Prognosis
Carpal tunnel syndrome can follow very different paths depending on the severity of nerve compression and how early treatment begins. Nearly 90% of patients with mild to moderate symptoms respond well to conservative treatment, such as splinting, activity modification, physical therapy, or corticosteroid injections. For many of them, symptoms improve or stabilize without the need for surgery.
However, in a portion of patients the condition continues to progress, even with appropriate therapy. As the median nerve remains compressed, symptoms gradually intensify — numbness becomes more persistent, hand strength declines, and fine motor tasks become increasingly difficult. Over time, untreated or advanced carpal tunnel syndrome can lead to permanent nerve damage, resulting in chronic sensory loss, weakness, and reduced hand function.
In the advanced stage, visible thenar muscle atrophy is often present. Patients who show severe abnormalities on EMNG or already have muscle wasting generally have a poorer prognosis, because the nerve may not fully recover even after surgical decompression. For this reason, timely diagnosis and treatment are essential to prevent irreversible changes.
Overall, the prognosis is excellent when the condition is treated early, but significantly less favorable once permanent nerve injury has developed.
Frequently Asked Questions About Carpal Tunnel Syndrome
1. Does computer use increase the risk of developing carpal tunnel syndrome?
No. Regular computer use does not increase your risk of developing carpal tunnel syndrome. Although typing may temporarily worsen symptoms in people who already have CTS, it is not a proven cause of the condition.
2. Can certain exercises increase the risk of carpal tunnel syndrome?
Generally no. However, any activity that keeps the wrist in a prolonged flexed position or applies sustained pressure to the carpal tunnel can contribute to symptoms. This includes weightlifting with poor wrist alignment or repetitive forceful gripping.
3. Can carpal tunnel syndrome return after surgery?
Yes. Although surgery is highly effective, the carpal tunnel can narrow again over time, and some patients may require a second procedure. Recurrence is more common in people with diabetes, inflammatory arthritis, or heavy repetitive hand use.
4. Is numbness and tingling normal after surgery?
Yes. Sensory recovery depends on the degree of nerve damage before surgery.
- Many patients with mild disease feel improvement immediately.
- Patients with moderate disease improve over weeks to months.
- In severe cases, full sensation may take 6–12 months, and some patients may never regain completely normal feeling. Even in these cases, surgery is still important to prevent further deterioration.
5. When does grip strength return after carpal tunnel surgery?
Most patients regain grip strength within 2–3 months. If the nerve was severely damaged before surgery, strength may take 6–12 months to recover. In very advanced cases, pre‑injury strength may never fully return, although function usually improves.
6. Can carpal tunnel syndrome affect both hands? (Bilateral CTS)
Yes. Carpal tunnel syndrome is frequently bilateral, although symptoms are often worse in the dominant hand. Bilateral CTS is more common in people with systemic conditions such as diabetes, hypothyroidism, rheumatoid arthritis, or pregnancy.
7. Does sleeping position affect carpal tunnel symptoms?
Absolutely. Many patients worsen symptoms by sleeping with the wrist fully flexed or by placing pressure on the palm. Wearing a night splint helps keep the wrist neutral and reduces night‑time numbness and tingling.
8. Is carpal tunnel syndrome hereditary?
There is a genetic component. Some people are born with a naturally narrower carpal tunnel, which increases susceptibility. Family history can therefore play a role.
9. Can pregnancy cause carpal tunnel syndrome?
Yes. Fluid retention and hormonal changes during pregnancy can increase pressure in the carpal tunnel. Symptoms usually improve after delivery, but splinting and activity modification may help during pregnancy.
10. Can carpal tunnel syndrome go away on its own?
Mild cases may improve with rest, ergonomic changes, and splinting. However, progressive or long‑standing symptoms rarely resolve spontaneously
Sevy JO, Sina RE, Varacallo MA. Carpal Tunnel Syndrome. StatPearls Publishing. StatPearls review: Carpal tunnel syndrome overview, diagnosis, and treatment
Bland JD. Carpal tunnel syndrome. BMJ. BMJ clinical review: Evidence-based overview of carpal tunnel syndrome
Burke FD, Ellis J, McKenna H, Bradley MJ. Primary care management of carpal tunnel syndrome. Postgraduate Medical Journal. Primary care guide: Conservative and clinical management of carpal tunnel syndrome
InformedHealth.org (IQWiG). Overview: Carpal tunnel syndrome. Patient-friendly overview: Symptoms, causes, diagnosis, and treatment options
BMJ Clinical Review. Carpal tunnel syndrome. BMJ 2014. BMJ review article: Clinical assessment and management of carpal tunnel syndrome
Chammas M, Boretto J, Burmann LM, et al. Carpal tunnel syndrome – Part I (anatomy, physiology, etiology and diagnosis). Revista Brasileira de Ortopedia. Scientific review: Anatomy, pathophysiology, and diagnosis of carpal tunnel syndrome
Milczarek C, Czyzewski B, Kozlowski K, et al. Carpal Tunnel Syndrome: A Comprehensive Review. Cureus. Comprehensive review: Modern evidence on diagnosis and treatment of carpal tunnel syndrome
Đilvesi Đ, Jelača B, Knežević A, et al. Evolution of Carpal Tunnel Syndrome Treatment: A Narrative Review. NeuroSci. Narrative review: Evolution of surgical and non-surgical carpal tunnel treatments
Evers S, Bryan AJ, Sanders TL, et al. Corticosteroid Injections for Carpal Tunnel Syndrome: Long-Term Follow-Up in a Population-Based Cohort. Plastic and Reconstructive Surgery. Evidence review: Effectiveness of corticosteroid injections for carpal tunnel syndrome
InformedHealth.org (IQWiG). Carpal tunnel syndrome: Learn More – How effective are steroids? Evidence summary: Benefits and limitations of steroid injections for carpal tunnel syndrome

















