

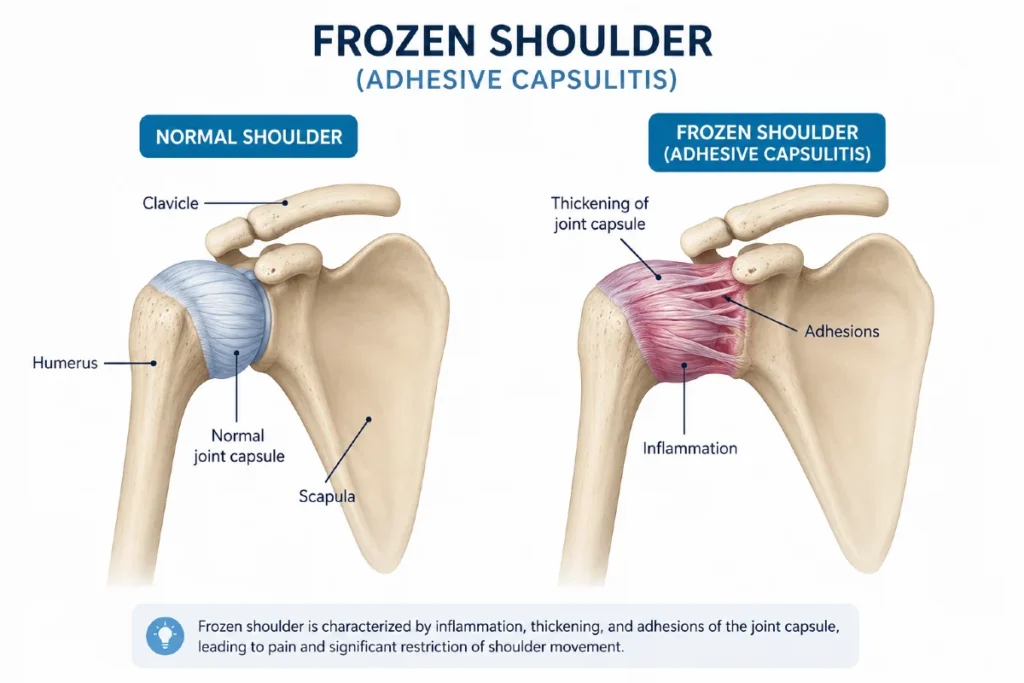
Frozen shoulder (also known as adhesive capsulitis) is a painful condition that causes a gradual loss of shoulder mobility. It develops when the capsule surrounding the shoulder joint becomes inflamed, thickened, and tight — a process called fibrosis — which restricts movement and leads to significant stiffness. Although the exact cause is still not fully understood, frozen shoulder is more common in people with certain medical conditions and often appears after a shoulder injury or period of immobilization.
Recovery can be slow, typically lasting two to three years, and the combination of pain and limited mobility can significantly affect daily activities such as dressing, reaching overhead, or sleeping on the affected side. The good news is that most people improve with proper treatment, which may include physical therapy, pain‑relief medications, corticosteroid injections, and in some cases, minimally invasive surgery.
In this guide, we’ll break down why frozen shoulder happens, how to recognize the early signs, which treatments work best, and which exercises can help speed up recovery.
Key Clinical Points – Frozen Shoulder (Adhesive Capsulitis)
- Frozen shoulder, also known as adhesive capsulitis, is a condition characterized by progressive shoulder pain and stiffness caused by inflammation and thickening of the joint capsule.
- The hallmark clinical finding is the shoulder capsular pattern — a predictable loss of motion where external rotation is most limited, followed by abduction and internal rotation.
- Frozen shoulder typically progresses through three stages (freezing, frozen, thawing), with a total duration of 1–3 years depending on severity and treatment.
- The condition is most common in adults aged 40–60 years and is strongly associated with diabetes, thyroid disorders, prolonged immobilization, and previous shoulder injury.
- Frozen shoulder treatment is primarily conservative and includes NSAIDs, corticosteroid injections, physical therapy, and structured home exercise programs.
- Approximately 50% of patients experience meaningful pain reduction and improved mobility after a corticosteroid injection, especially in the early painful stage.
- Hydrodilatation and arthroscopic capsular release are reserved for patients who fail to improve after several months of non‑operative management.
- Most patients ultimately achieve near‑full recovery, although mild residual stiffness may persist in some cases.
What Causes Frozen Shoulder?
The exact cause of frozen shoulder is still not fully understood, but the condition most commonly affects adults between the ages of 40 and 60 and is slightly more common in women. What we do know is that the shoulder capsule — the connective tissue surrounding the joint — becomes inflamed, thickened, and tight, gradually restricting movement.
Several factors can increase the risk:
- Diabetes and metabolic conditions — People with diabetes are significantly more likely to develop frozen shoulder. Thyroid disorders and heart disease also raise the risk. In these cases, symptoms often develop slowly and subtly.
- Shoulder injury or immobilization — A fracture, dislocation, or prolonged use of a sling can trigger stiffness and inflammation in the capsule.
- Post‑surgical stiffness — Frozen shoulder may appear after shoulder surgery or even after chest procedures where arm movement is limited.
- Other painful shoulder conditions — Rotator cuff injuries, impingement syndrome, bursitis, or calcific tendinopathy can all lead to reduced movement, which may trigger the cascade that results in adhesive capsulitis.
In short, anything that causes prolonged pain, inflammation, or reduced movement in the shoulder can increase the likelihood of developing frozen shoulder.
What Happens Inside the Shoulder During Frozen Shoulder?
The driving force behind frozen shoulder is inflammation of the shoulder capsule — the connective tissue that surrounds the glenohumeral joint. For reasons that are still not fully understood, this capsule becomes inflamed, thickened, and tight, a process known as fibrosis. As the capsule loses its normal elasticity, the joint gradually becomes stiffer and more painful.
Many patients instinctively try to avoid painful movements by “protecting” the arm, which leads to even less shoulder motion. Reduced movement accelerates the tightening of the capsule, giving the humeral head less space to glide. Over time, the joint may also lose synovial fluid, which normally lubricates the shoulder and allows smooth motion.
In more advanced stages, bands of scar tissue (adhesions) can form between the capsule and the humeral head. These adhesions further restrict movement and contribute to the characteristic stiffness of adhesive capsulitis.
In short, frozen shoulder is a combination of inflammation, fibrosis, loss of lubrication, and scar‑tissue formation — all of which progressively limit shoulder mobility.
Frozen Shoulder Symptoms
Frozen shoulder — also known as adhesive capsulitis or adhesive capsulitis of the shoulder — usually begins gradually and often without a clear trigger. In most people, the first symptom is shoulder pain, typically present even at rest and noticeably worse with movement. Although the onset is usually slow and subtle, in some cases symptoms can appear more suddenly.
Over the following days or weeks, pain is followed by progressive stiffness and a marked reduction in both active and passive range of motion. One of the hallmark findings of frozen shoulder is the shoulder capsular pattern — a characteristic sequence in which certain movements become restricted. The earliest and most pronounced limitation is external rotation, followed by abduction, and later internal rotation.
As adhesive capsulitis progresses, everyday activities become increasingly difficult:
- Limited overhead reach — such as hanging clothes, reaching for items on high shelves, or painting.
- Reduced ability to move the arm out to the side — making tasks like fastening a seatbelt or putting on a jacket challenging.
- Restricted rotational movements — causing difficulties with personal hygiene, dressing, or combing hair.
- Secondary neck pain — as neck muscles overwork to compensate for the loss of shoulder mobility.
Because frozen shoulder significantly affects both pain levels and mobility, it can interfere with work, sleep, and daily routines. The condition typically progresses through three distinct stages, each with its own symptom pattern and duration — which we’ll explain in the next section.
Frozen Shoulder Stages
Adhesive capsulitis of the shoulder — typically progresses through three overlapping stages. These stages are not sharply separated; symptoms often blend gradually from one phase to the next. While each stage has an approximate duration, the timeline can vary significantly from person to person.
Stage I: The “Freezing” Stage
This is the phase where pain is the dominant symptom. It usually begins gradually, with a deep, aching pain throughout the shoulder that is often worst at night. Over time, pain starts appearing even at rest and becomes sharper with movement.
A few days to weeks after the onset of pain, patients begin to notice progressive stiffness and a reduction in shoulder mobility. This is when the classic shoulder capsular pattern starts to appear — external rotation becomes limited first, followed by abduction and internal rotation.
Typical duration: 3 to 9 months.
Stage II: The “Frozen” Stage
During this stage, pain slowly decreases, but stiffness becomes the main problem. Range of motion is significantly restricted, making everyday activities difficult:
- reaching overhead
- fastening a seatbelt
- putting on a jacket
- washing or reaching behind the back
- combing or styling hair
Although mobility is severely limited, many patients tolerate this stage better because the pain is less intense than in the freezing phase.
Typical duration: 4 to 12 months.
Stage III: The “Thawing” Stage
In the final stage, the shoulder gradually begins to regain mobility. The capsule becomes less tight, adhesions soften, and range of motion improves month by month. Strength also returns as movement increases.
Full recovery to normal or near‑normal function can take 6 months to 2 years, depending on the severity of adhesive capsulitis and the consistency of rehabilitation.
| Phase | Characteristics and Duration |
|---|---|
| Phase I – “Freezing” | Gradual development of diffuse shoulder pain, initially more noticeable at night and later even at rest. Pain worsens with movement. After several days or weeks, progressive restriction of shoulder motion develops. Typically lasts about 3–9 months. |
| Phase II – “Frozen” | Pain gradually decreases, but shoulder mobility remains severely limited. Daily activities such as combing hair, fastening a bra, or reaching overhead shelves may become very difficult. Typically lasts about 4–12 months. |
| Phase III – “Thawing” | Gradual recovery and return of shoulder mobility. Pain significantly improves or disappears completely. Full functional recovery may take from 6 months up to 2 years. |
Ahesive Capsulitis of Shoulder Diagnosis
Diagnosing frozen shoulder (adhesive capsulitis) — is based on a combination of patient history, a detailed physical examination, and, when needed, imaging studies. There are no specific blood tests for this condition; in most cases, the diagnosis is made clinically because the symptoms and movement limitations are highly characteristic.
Physical Examination
A thorough physical exam is the most important step in diagnosing frozen shoulder. Your clinician will compare the active (you move the arm) and passive (the clinician moves your arm while you relax) range of motion on both the affected and unaffected sides.
Key findings include:
- Reduced shoulder range of motion in all directions
- Pain during testing, especially at the end range
- Significant loss of both active and passive movement — a hallmark feature that helps distinguish frozen shoulder from rotator cuff tears
- Most pronounced limitations in external rotation and abduction, consistent with the classic shoulder capsular pattern
- Muscle strength may appear reduced, but this is usually due to pain rather than true weakness
Because pain can limit cooperation during the exam, the clinician may need to assess movement gently and gradually.
Imaging Studies
Imaging is not always required to diagnose frozen shoulder, but it can be helpful when symptoms are unclear or when other conditions need to be ruled out.
X‑ray (Radiograph)
An X‑ray does not confirm frozen shoulder, but it is useful to exclude other causes of stiffness such as arthritis, fractures, or bone abnormalities.
Ultrasound and MRI
Ultrasound and MRI provide a better look at the soft tissues of the shoulder. They can help identify:
- rotator cuff tears
- bursitis
- calcific tendinopathy
- other soft‑tissue injuries
MRI can also support the diagnosis of adhesive capsulitis by showing:
- thickening of the joint capsule
- thickening of the inferior glenohumeral ligament
- reduced joint volume
These findings are typical for frozen shoulder but are not always necessary to make the diagnosis.
Clinical Insight
The diagnosis of frozen shoulder is primarily clinical, based on the characteristic loss of both active and passive shoulder motion, with imaging used mainly to rule out other conditions — and in unclear cases, MRI may be required to confirm the diagnosis.
Frozen Shoulder Treatment
Most cases of frozen shoulder improve gradually over time, even without aggressive intervention. Recovery typically takes 18 to 30 months, and the majority of patients eventually experience significant improvement or complete resolution of symptoms.
The goals of frozen shoulder treatment are twofold:
- reduce pain and inflammation
- restore shoulder mobility and function
In the early “freezing” stage of the adhesive capsulitis of shoulder, inflammation and severe pain dominate, while in later stages stiffness becomes the primary issue. Treatment may include medications, corticosteroid injections, physical therapy, and in resistant cases, procedures such as hydrodilatation or surgery.
Medications
Pain‑relief medications and NSAIDs (ibuprofen, diclofenac, ketoprofen, naproxen) are commonly used to reduce pain and inflammation. These should always be taken under medical supervision to minimize the risk of side effects.
Corticosteroid Injections
Corticosteroid injections are an available treatment option within the broader approach to frozen shoulder treatment, particularly useful in the early, painful “freezing” stage. These powerful anti‑inflammatory medications help reduce swelling inside the joint capsule and can provide rapid pain relief. When injected directly into the shoulder joint, ideally under ultrasound guidance, they offer the best accuracy and the lowest risk of complications.
Importantly, around half of all patients experience a meaningful reduction in pain and an improvement in shoulder mobility after a corticosteroid injection 1 — making this one of the more effective early interventions for adhesive capsulitis.
Because repeated steroid use can weaken tendons and cartilage, injections should generally be limited to no more than three per year.
Physical Therapy and Exercises
Physical therapy is a cornerstone of adhesive capsulitis treatment, helping control pain and gradually restore mobility. It may include:
- gentle stretching and soft‑tissue mobilization of the shoulder, scapula, and neck
- therapeutic modalities such as ultrasound, heat therapy, TENS, LASER, or diathermy
- strengthening exercises for the rotator cuff and scapular stabilizers
Range‑of‑Motion Exercises
Rehabilitation should focus heavily on therapeutic exercises, especially stretching in all directions to lengthen the tight joint capsule. Strengthening exercises are added progressively.
In the early painful stage, some patients tolerate stretching poorly — but gentle, supervised exercises are still recommended to slow the progression of stiffness.
Daily home exercises are strongly encouraged.
Aggressive stretching is not recommended, as it may worsen symptoms without providing additional benefits or improving long-term outcomes.
Hydrodilatation (Capsular Distension)
Hydrodilatation involves slowly injecting a larger volume of sterile fluid into the shoulder joint to stretch and expand the tight capsule. It is usually performed by an orthopedic surgeon, physiatrist, or radiologist under ultrasound or fluoroscopic guidance.
This procedure can reduce pain and improve range of motion, especially in patients who do not respond to standard conservative treatment.
Surgical Treatment of Adhesive Capsulitis
Surgery for frozen shoulder is considered only when symptoms persist despite 6 months or more of non‑operative treatment, and typically after the freezing stage has passed.
The goal is to release the tight capsule and restore mobility. The two main surgical options are:
Manipulation Under Anesthesia (MUA)
Performed under general anesthesia, the surgeon moves the shoulder through its full range of motion to stretch or tear the tight capsule and adhesions.
Shoulder Arthroscopy
Through small incisions, the surgeon uses a camera and instruments to cut and release the contracted capsule under direct visualization.
In many cases, MUA and arthroscopic release are combined to achieve the best results. Most patients experience significant improvement after these procedures.
Frequently Asked Questions (FAQ)
How often should I do exercises for frozen shoulder?
Regular exercise is one of the most important parts of frozen shoulder treatment. Most patients benefit from performing mobility and stretching exercises once or twice daily, for 15 to 30 minutes. Consistency matters far more than intensity — improvements come gradually, but daily movement helps reduce pain and improve range of motion over time.
Which medications are recommended for frozen shoulder?
For symptom relief, doctors commonly consider NSAIDs such as ibuprofen or diclofenac, which help reduce pain and inflammation. Oral corticosteroids are generally not recommended for adhesive capsulitis. Any medication should be taken only according to medical advice to minimize potential side effects.
How long does recovery from frozen shoulder take?
Recovery from adhesive capsulitis of the shoulder typically takes 1 to 3 years, depending on symptom severity, age, and associated medical conditions. Although the condition often improves on its own, proper treatment — including physical therapy and structured exercise — can shorten the duration and improve long‑term outcomes.
When should I see a doctor for frozen shoulder?
You should consult a healthcare professional if shoulder pain persists for more than a few weeks, especially if it is accompanied by stiffness or loss of motion. Early evaluation helps rule out other conditions and allows timely initiation of frozen shoulder treatment, which can significantly improve quality of life.
How can I tell if it’s frozen shoulder or another shoulder condition?
Frozen shoulder can mimic other causes of shoulder pain such as rotator cuff tendinopathy, impingement syndrome, or arthritis. The key difference is the loss of both active and passive range of motion — in frozen shoulder, even a doctor cannot move your arm fully when examining you. Other conditions usually limit movement because of pain, not stiffness.
To learn how to distinguish frozen shoulder from other causes of shoulder pain, read our detailed guide on Shoulder Pain Diagnosis Chart: A Clinician’s Quick Guide.
Can frozen shoulder return after recovery?
Recurrence in the same shoulder is uncommon, but frozen shoulder can develop in the opposite shoulder — sometimes within a few years. Prevention includes regular shoulder mobility exercises, avoiding prolonged immobilization, and addressing shoulder pain or injuries promptly.
Date A, Rahman L. Frozen Shoulder: Overview of Clinical Presentation and Review of the Current Evidence Base for Management Strategies. Future Science OA. Evidence-based review: Frozen shoulder pathophysiology, diagnosis, and treatment strategies
Smith CB, Ryan V, Annison D, Cairns M, Chester R, Lewis J. Corticosteroid Injections for Frozen Shoulder: A Global Online Survey of Health Professionals’ Current Practice and Opinion. Musculoskeletal Care. PubMed: Current clinical practice and opinions on corticosteroid injections for frozen shoulder
Li D, St Angelo JM, Taqi M. Adhesive Capsulitis (Frozen Shoulder). StatPearls Publishing. Evidence-based review: Frozen shoulder diagnosis, stages, and management
Dias R, Cutts S, Massoud S. Frozen Shoulder. BMJ. BMJ clinical review: Frozen shoulder diagnosis and treatment overview
BMJ Best Practice. Frozen Shoulder (Adhesive Capsulitis). BMJ clinical decision guide: Frozen shoulder evaluation and management
Moosmayer S, Ekeberg OM, Hallgren HB, Heier I, Kvalheim S, Juel NG, Blomquist J, Pripp AH, Brox JI. Ultrasound Guided Lavage with Corticosteroid Injection Versus Sham Lavage with and Without Corticosteroid Injection for Calcific Tendinopathy of Shoulder. BMJ. Randomized clinical trial: Ultrasound-guided shoulder injection procedures and outcomes

















