

Multilevel disc degeneration is a condition in which multiple intervertebral discs in the spine undergo progressive wear and tear over time. It is commonly associated with aging, repetitive mechanical stress, and reduced disc hydration, leading to structural changes that can affect spinal function.
When these degenerative changes become painful, the condition is often referred to as multilevel discogenic disease, meaning that the intervertebral discs themselves are the primary source of back pain.
Understanding the difference between structural disc degeneration and discogenic pain is essential for accurate diagnosis and effective treatment—especially in patients with chronic lower back pain involving multiple spinal levels.
- Multilevel disc degeneration is a condition in which multiple intervertebral discs undergo progressive structural wear and loss of height.
- It is commonly associated with aging, repetitive mechanical stress, and reduced disc hydration.
- When degeneration becomes painful, the condition is often referred to as multilevel discogenic disease.
- Discogenic pain originates from the intervertebral discs and may present as chronic lower back pain with or without nerve symptoms.
- Diagnosis is based on clinical evaluation and imaging, including MRI as the gold standard for assessing disc degeneration.
- Most cases are managed conservatively with physical therapy, exercise, and lifestyle modifications.
Key Differences Between Multilevel Disc Degeneration and Discogenic Disease
Although closely related, multilevel disc degeneration and multilevel discogenic disease describe different aspects of spinal pathology. Degeneration refers to structural changes affecting multiple intervertebral discs over time, while discogenic disease specifically refers to pain originating from these degenerative discs.
The table below highlights the key clinical and structural differences between these two conditions to improve understanding, diagnosis, and treatment planning.
| Feature | Multilevel Disc Degeneration | Multilevel Discogenic Disease |
|---|---|---|
| Definition | Structural degeneration of multiple intervertebral discs, including loss of hydration, height reduction, and disc wear. | A condition where degenerative discs become a source of chronic back pain (discogenic pain). |
| Primary Focus | Anatomical and structural changes within the spine. | Pain generation originating from damaged intervertebral discs. |
| Symptoms | May be asymptomatic or cause stiffness and reduced mobility. | Chronic lower back pain, often worsened by sitting, bending, or spinal loading. |
| Cause | Aging, repetitive mechanical stress, poor posture, and loss of disc hydration. | Degenerated discs that become sensitized and act as a source of pain. |
| Diagnosis | Imaging studies such as MRI showing disc height loss, desiccation, and structural changes. | Clinical correlation of symptoms with imaging findings; discogenic pain may require diagnostic confirmation. |
| Treatment Approach | Focus on slowing degeneration through exercise, physical therapy, and lifestyle modification. | Pain management, rehabilitation, and in some cases interventional or surgical options. |
What Is Multilevel Disc Degeneration?
Multilevel disc degeneration is a condition in which two or more intervertebral discs undergo progressive structural changes due to aging, mechanical stress, and reduced biological resilience. Unlike single-level degeneration, this process affects multiple segments of the spine, most commonly in the lumbar and cervical regions, leading to a broader impact on spinal function.
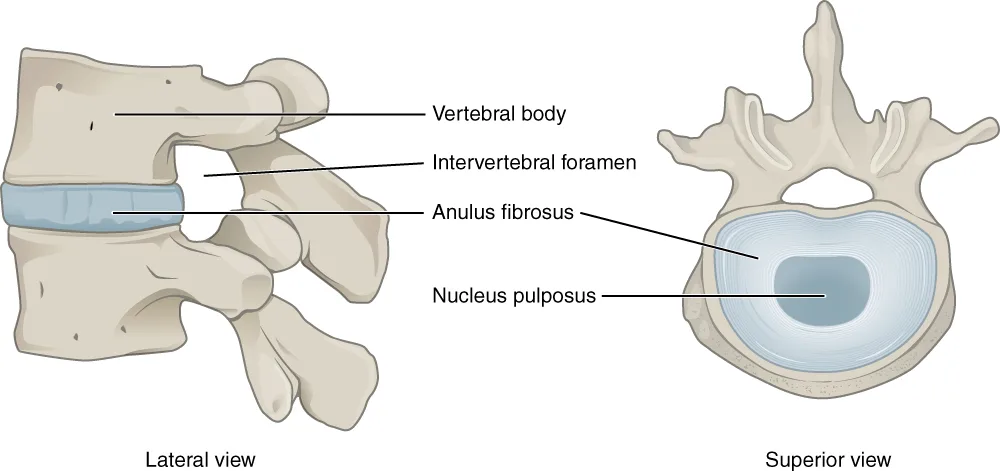
At its core, disc degeneration involves loss of hydration (disc desiccation), decreased disc height, and gradual breakdown of the disc’s internal structure. The intervertebral disc, composed of the nucleus pulposus and annulus fibrosus, loses its ability to absorb and distribute load effectively over time.
How Does Multilevel Disc Degeneration Develop?
Disc degeneration is a multifactorial and progressive process influenced by:
- Age-related changes (natural wear and tear)
- Reduced disc nutrition and hydration
- Repetitive mechanical stress on the spine
- Poor posture and prolonged sitting
- Genetic predisposition
As degeneration progresses across multiple levels, the spine experiences cumulative structural changes, rather than isolated damage at a single segment.
Which Spinal Levels Are Affected?
Multilevel degeneration most commonly affects:
- Lumbar spine (L4–L5, L5–S1) → due to high load-bearing demands
- Cervical spine (C5–C6, C6–C7) → due to mobility and repetitive motion
These regions are particularly vulnerable because they experience the greatest mechanical load and movement stress during daily activities.
Why “Multilevel” Matters
The term “multilevel” is clinically important because it reflects a more widespread degenerative process affecting spinal biomechanics.
When multiple discs degenerate:
- Load distribution becomes uneven
- Adjacent segments are exposed to increased mechanical stress
- The spine may lose its normal alignment and flexibility
- There is a higher risk of chronic pain and functional limitation
In other words, multilevel degeneration is not just “more discs involved” — it represents a systemic decline in spinal function.
Biomechanics and Spinal Load
Healthy intervertebral discs act as shock absorbers, distributing forces evenly across the spine during movement. In multilevel disc degeneration, this function becomes impaired.
As discs lose height and elasticity:
- Axial load increases on facet joints
- Spinal stiffness increases
- Micro-instability may develop in certain segments
- Compensatory changes occur in surrounding structures
Over time, these biomechanical alterations can lead to a cycle of degeneration, where increased stress accelerates further disc damage.
What Is Multilevel Discogenic Disease?
Multilevel discogenic disease refers to a condition in which multiple intervertebral discs become a direct source of pain, rather than just showing structural degeneration on imaging. Unlike general disc degeneration, where changes may be asymptomatic, discogenic disease specifically involves pain generation from the disc itself.
Discogenic Pain: The Core Concept
At the center of this condition is discogenic pain, a type of nociceptive pain originating from damaged or structurally altered intervertebral discs.
Healthy discs are normally poorly innervated, meaning they do not generate pain signals easily. However, when degeneration progresses, the disc can become a pain-sensitive structure due to internal disruption and biochemical changes.
How the Disc Becomes a Source of Pain
The intervertebral disc consists of two key components:
- Annulus fibrosus – the outer fibrous ring that provides structural integrity
- Nucleus pulposus – the inner gel-like core responsible for shock absorption
With repeated stress and aging:
- The annulus fibrosus develops microtears
- The nucleus pulposus loses hydration and elasticity
- Internal disc pressure and load distribution become altered
These changes lead to internal disc disruption, which is a major trigger for discogenic pain.
Nociceptive Mechanism and Nerve Ingrowth
One of the most important pathological features of discogenic disease is nerve ingrowth.
As the disc degenerates:
- Small nerve fibers begin to grow deeper into the annulus fibrosus
- Inflammatory mediators are released within the disc
- Previously non-painful structures become pain generators
This process transforms the disc into an active nociceptive source, capable of producing:
- Deep, axial low back pain
- Pain worsened by sitting, bending, or prolonged loading
- Pain without clear nerve root compression (unlike radiculopathy)
Why “Multilevel” Matters
When discogenic disease affects multiple spinal levels, the clinical picture becomes more complex:
- Pain is often more diffuse and persistent
- Biomechanical stress is distributed across several segments
- There is a higher cumulative spinal load, which perpetuates degeneration
This multi-segment involvement makes both diagnosis and treatment more challenging, as symptoms may not localize to a single disc level.
In clinical practice, distinguishing multilevel disc degeneration (structural changes) from multilevel discogenic disease (pain-generating condition) is critical for choosing the right therapeutic approach.
Causes and Risk Factors
Understanding the causes and risk factors of multilevel disc degeneration and discogenic disease is essential for both prevention and long-term management. In most cases, the condition develops due to a combination of biological aging, mechanical stress, and lifestyle factors that gradually affect spinal structures.
Aging
- The most significant factor in disc degeneration
- Intervertebral discs naturally lose hydration and elasticity over time
- Reduced disc height leads to increased spinal load and mechanical stress
- Age-related changes affect multiple levels, contributing to multilevel involvement
Genetics
- Genetic predisposition plays a major role in early disc degeneration
- Some individuals inherit weaker disc structure or altered collagen composition
- Family history increases the risk of multilevel disc disease
Repetitive Stress
- Repeated loading of the spine accelerates disc wear and tear
- Common in occupations involving:
- Heavy lifting
- Prolonged sitting
- Repetitive bending or twisting
- Frequently seen in athletes exposed to chronic spinal stress
Poor Posture
- Sustained poor posture increases uneven disc pressure
- Forward head posture and prolonged sitting place excessive load on:
- Cervical spine
- Lumbar discs
- Over time, this contributes to progressive multilevel degeneration
Obesity
- Excess body weight significantly increases axial spinal load
- Leads to faster disc degeneration, especially in the lumbar spine
- Associated with reduced mobility and higher risk of chronic back pain
Smoking
- Smoking reduces blood supply and oxygenation to spinal discs
- Impairs nutrient delivery and accelerates disc degeneration
- Increases inflammation and delays healing processes
In most patients, multiple risk factors coexist, which explains why multilevel disc degeneration often progresses gradually and affects several spinal segments simultaneously.
| Risk Factor | How It Affects the Spine | Clinical Impact |
|---|---|---|
| Aging | Disc dehydration, loss of elasticity, reduced disc height | Progressive multilevel degeneration and increased spinal load |
| Genetics | Inherited disc weakness and altered collagen structure | Earlier onset and higher risk of multilevel disc disease |
| Repetitive Stress | Chronic mechanical loading and microtrauma to discs | Accelerated degeneration and increased risk of discogenic pain |
| Poor Posture | Uneven pressure distribution across spinal segments | Increased strain on cervical and lumbar discs over time |
| Obesity | Excess axial load on intervertebral discs | Faster degeneration, especially in the lumbar spine |
| Smoking | Reduced blood flow and impaired disc nutrition | Accelerated degeneration and delayed healing processes |
Symptoms and Clinical Presentation
Understanding the symptoms of multilevel disc degeneration vs discogenic disease is essential for accurate diagnosis, as these conditions can present differently despite affecting the same spinal structures.
Symptoms of Multilevel Disc Degeneration
Multilevel disc degeneration is often a gradual and sometimes asymptomatic condition, especially in early stages.
Common symptoms include:
- Spinal stiffness, especially after inactivity
- Reduced mobility and flexibility
- Mild to moderate chronic back or neck discomfort
- Occasional mechanical pain with movement
In many cases, imaging may show significant degeneration, while symptoms remain minimal or absent.
Symptoms of Multilevel Discogenic Disease
In contrast, multilevel discogenic disease is pain-driven, with the intervertebral discs acting as the primary source of symptoms.
Typical symptoms include:
- Chronic lower back pain (deep, axial pain)
- Pain that worsens with prolonged sitting
- Increased pain during forward bending (flexion)
- Referred pain to the buttocks or thighs (without clear nerve compression)
- Pain triggered by spinal loading or sustained posture
Unlike nerve-related pain, discogenic pain is usually localized and mechanical, but can become persistent and functionally limiting.
| Feature | Multilevel Disc Degeneration | Multilevel Discogenic Disease |
|---|---|---|
| Pain Presence | Often mild or absent | Primary symptom (chronic pain) |
| Pain Type | Mechanical, occasional | Deep, axial, discogenic pain |
| Stiffness | Common | May be present |
| Mobility | Reduced over time | Limited due to pain |
| Pain Triggers | Movement, prolonged activity | Sitting, flexion, spinal loading |
| Referred Pain | Less common | Common (buttocks, thighs) |
| Clinical Significance | May be incidental finding | Clinically significant pain generator |
Key Clinical Difference
The most important distinction:
- Multilevel disc degeneration → may be asymptomatic or mildly symptomatic
- Multilevel discogenic disease → pain is the dominant feature
This difference is crucial when correlating MRI findings with clinical symptoms, as not all degenerative changes are clinically relevant.
Diagnosis and Imaging
Accurate diagnosis of multilevel disc degeneration and multilevel discogenic disease requires a combination of clinical evaluation and targeted imaging. Because structural changes on imaging do not always correlate with symptoms, it is essential to match clinical findings with radiological evidence.
Clinical Examination
The clinical assessment focuses on identifying pain patterns, functional limitations, and mechanical triggers.
Typical findings may include:
- Axial low back or neck pain without clear radiculopathy
- Pain reproduced with spinal flexion, loading, or prolonged sitting
- Reduced range of motion and segmental stiffness
- Absence of significant neurological deficits (in pure discogenic pain)
A key clinical goal is to distinguish discogenic pain from other causes such as facet joint pain or nerve root compression.
MRI (Gold Standard)
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating disc pathology, especially in multilevel disease.
MRI provides detailed visualization of:
- Disc degeneration (signal loss, disc desiccation)
- Disc height loss across multiple levels
- Annular tears and internal disc disruption
- Nerve structures and potential compression
A particularly important MRI finding is:
- Modic changes – signal changes in the vertebral endplates associated with disc degeneration
- Type I → inflammation and edema
- Type II → fatty degeneration
- Type III → sclerosis
Modic changes are often correlated with discogenic pain, making MRI essential not just for structure, but for clinical interpretation.
X-ray
X-rays are useful as an initial imaging tool, especially for assessing spinal alignment and structural changes.
They can show:
- Disc height loss
- Osteophyte formation
- Alignment abnormalities (e.g., lordosis changes)
However:
- X-rays cannot assess soft tissues or disc integrity
- They are limited in detecting early degeneration or discogenic pain
X-ray is helpful for overview, but insufficient alone for diagnosis of discogenic disease.
Discogenic Pain Testing (Provocative Tests)
In selected cases, provocative disc testing (discography) may be used to confirm the disc as the source of pain.
This involves:
- Injection of contrast into the disc
- Reproduction of the patient’s typical pain pattern
- Imaging to assess internal disc structure
While controversial, discography can help identify the symptomatic disc level, especially in complex multilevel cases.
The table below summarizes the most important diagnostic methods used to evaluate multilevel disc degeneration and discogenic disease.
| Diagnostic Method | What It Shows | Clinical Value |
|---|---|---|
| Clinical Examination | Pain patterns, mobility limitations, mechanical triggers | Helps differentiate discogenic pain from other causes |
| MRI (Gold Standard) | Disc degeneration, disc height loss, annular tears, Modic changes | Most accurate method for correlating structure with symptoms |
| X-ray | Disc height loss, osteophytes, spinal alignment | Useful for structural overview but limited for soft tissue |
| Discography (Provocative Testing) | Pain reproduction and internal disc structure | Identifies symptomatic disc level in complex cases |
Key Diagnostic Insight
- Multilevel disc degeneration → structural findings (may be asymptomatic)
- Multilevel discogenic disease → diagnosis requires clinical correlation + pain reproduction
The most important principle:
Not all degenerated discs cause pain—but symptomatic discs must match the clinical picture.
Treatment Options
The treatment of multilevel disc degeneration and discogenic disease depends on symptom severity, functional limitation, and whether pain is structural or discogenic in origin. In most cases, conservative treatment is the first-line approach, with surgical options reserved for more severe or refractory cases.
Conservative Treatment
Conservative management aims to reduce pain, improve function, and slow progression of degenerative changes.
Physical Therapy and Exercise
- Core strengthening to support spinal stability
- Postural correction to reduce mechanical stress
- Mobility exercises to improve flexibility
- Stabilization programs for long-term spinal health
This is the cornerstone of treatment for both conditions.
Pain Management
- NSAIDs for inflammation and pain relief
- Short-term analgesics when needed
- Muscle relaxants in selected cases
Lifestyle Modifications
- Weight management to reduce spinal load
- Ergonomic adjustments (workstation, posture)
- Activity modification to avoid excessive strain
Interventional Treatments
When conservative therapy is insufficient, interventional procedures may be considered.
- Epidural steroid injections
- Facet joint injections
- Nerve blocks
These treatments target pain pathways and inflammation, especially in cases of discogenic pain.
Surgical Treatment
Surgery is typically reserved for severe or progressive cases, especially when there is:
- Persistent, disabling pain
- Neurological deficits
- Structural instability
- Failure of conservative treatment
Common surgical options include:
- Spinal fusion (stabilizes affected segments)
- Artificial disc replacement (preserves motion in selected cases)
- Decompression procedures (if nerve compression is present)
Surgical decisions are highly individualized and based on imaging, symptoms, and patient function.
The table above summarizes the main treatment options for multilevel disc degeneration and discogenic disease, from conservative care to surgical intervention.
| Treatment Type | What It Targets | Key Benefits |
|---|---|---|
| Physical Therapy | Muscle strength, posture, spinal stability | Improves function, reduces pain, long-term support |
| Exercise & Rehabilitation | Core stability and mobility | Reduces spinal load and prevents progression |
| Medications (NSAIDs) | Inflammation and pain | Short-term pain relief and symptom control |
| Lifestyle Modifications | Risk factors such as obesity and poor posture | Slows degeneration and reduces recurrence |
| Injections (Epidural, Nerve Blocks) | Inflammation and pain pathways | Targeted pain relief, especially in discogenic disease |
| Surgical Treatment | Structural instability and severe pain | Stabilizes spine and relieves pressure on neural structures |
Treatment Strategy: Key Insight
- Multilevel disc degeneration → focus on prevention + functional preservation
- Multilevel discogenic disease → focus on pain control + targeted intervention
The goal is not only to treat imaging findings, but to treat the patient’s symptoms and improve quality of life.
Lifestyle Changes and Prevention
Making targeted lifestyle changes can significantly slow the progression of
multilevel disc degeneration and reduce discogenic pain.
The goal is to minimize spinal stress, improve stability, and support long-term spinal health.
| Area | Key Recommendation |
|---|---|
| Ergonomics | Maintain proper posture, use lumbar support, avoid prolonged sitting |
| Exercise | Core strengthening, low-impact activity, and mobility exercises |
| Weight Management | Maintain healthy body weight to reduce spinal load |
| Smoking Cessation | Improves disc nutrition and slows degeneration |
When to Seek Medical Help
Recognizing when to seek medical attention for multilevel disc degeneration or discogenic disease is essential to prevent complications and ensure timely treatment. While many cases can be managed conservatively, certain red flag symptoms require immediate evaluation by a healthcare professional.
Red Flag Symptoms
Seek medical help without delay if you experience:
- Severe or worsening pain that does not improve with rest or medication
- Pain radiating into the arms or legs (possible nerve involvement)
- Numbness, tingling, or weakness in the limbs
- Loss of coordination or difficulty walking
- Bowel or bladder dysfunction (possible serious nerve compression)
- Sudden pain after trauma or injury
- Rapidly progressing symptoms with functional impairment
These symptoms may indicate nerve compression, spinal instability, or other serious conditions requiring urgent assessment.
When Symptoms Should Not Be Ignored
Even in the absence of red flags, medical evaluation is recommended if:
- Pain persists for more than a few weeks
- Symptoms are progressively worsening
- Pain interferes with sleep, work, or daily activities
- There is no improvement with conservative treatment
Early diagnosis allows for timely imaging, accurate diagnosis, and targeted treatment, reducing the risk of long-term complications.
As a general rule, any new neurological symptoms or rapidly worsening pain should be evaluated promptly by a healthcare professional.
💡 Key takeaway
- Don’t ignore neurological symptoms
- Don’t wait if pain is worsening or persistent
- Early evaluation leads to better outcomes and prevents complications
FAQ
What is the difference between multilevel disc degeneration and discogenic disease?
Multilevel disc degeneration refers to structural changes in multiple intervertebral discs, while discogenic disease describes when these degenerative discs become a source of pain. Degeneration may be present without symptoms, whereas discogenic disease is typically pain-driven.
Can multilevel disc degeneration be reversed?
Multilevel disc degeneration is generally considered a progressive and irreversible process. However, its progression can be slowed with proper treatment, including physical therapy, exercise, and lifestyle modifications.
Is discogenic pain the same as a herniated disc?
No. Discogenic pain originates from internal disc damage, while a herniated disc involves disc material pressing on nearby nerves. Although they can coexist, they are different conditions with different mechanisms.
What are Modic changes and why are they important?
Modic changes are MRI findings that reflect degenerative changes in the vertebral endplates. They are strongly associated with discogenic pain and help clinicians identify the source of chronic back pain.
How is disc height loss related to degeneration?
Disc height loss is a key sign of disc degeneration. As discs lose hydration and structure, they become thinner, which increases spinal load and mechanical stress on surrounding structures.
Can exercise worsen disc degeneration?
Properly guided exercise does not worsen degeneration. In fact, exercise is one of the most effective treatments. However, improper or excessive loading without guidance can potentially aggravate symptoms.
When should I worry about back pain?
You should seek medical attention if you experience:
- Neurological symptoms (numbness, weakness, tingling)
- Severe or worsening pain
- Loss of bladder or bowel control
- Pain that does not improve with rest
These may indicate more serious underlying conditions requiring prompt evaluation.
Conclusion
Multilevel disc degeneration and multilevel discogenic disease are closely related but fundamentally different conditions. While degeneration refers to structural wear and tear affecting multiple intervertebral discs, discogenic disease occurs when these changes become a direct source of chronic back pain.
Understanding this distinction is essential for accurate diagnosis and effective treatment. Many individuals with disc degeneration remain asymptomatic, while others develop significant discogenic pain due to internal disc disruption, inflammation, and nerve ingrowth.
Early diagnosis through clinical evaluation and imaging (especially MRI) allows for timely intervention and better outcomes. Conservative treatment—including physical therapy, exercise, and lifestyle modifications—remains the cornerstone of management, while interventional or surgical options are reserved for more advanced or persistent cases.
Kalichman L, Hunter DJ. Diagnosis and conservative management of degenerative lumbar spondylosis. Eur Spine J. 2008;17(5):551–565. PubMed
Modic MT, Steinberg PM, Ross JS, Masaryk TJ, Carter JR. Degenerative disk disease: assessment of changes in vertebral body marrow with MR imaging. Radiology. 1988;166(1):193–199. PubMed
Bogduk N. Degenerative joint disease of the spine and discogenic pain. Pain. 2012;153(9):1796–1801. PubMed
Adams MA, Roughley PJ. What is intervertebral disc degeneration, and what causes it? Spine. 2006;31(18):2151–2161. PubMed
Brinjikji W, Luetmer PH, Comstock B, et al. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015;36(4):811–816. PubMed
Urban JP, Roberts S. Degeneration of the intervertebral disc. Arthritis Res Ther. 2003;5(3):120–130. PubMed
Kjaer P, Leboeuf-Yde C, Sorensen JS, Bendix T. An epidemiologic study of MRI and low back pain. Spine. 2005;30(10):1170–1177. PubMed
StatPearls Publishing. Intervertebral Disc Degeneration. NCBI Bookshelf
StatPearls Publishing. Discogenic Low Back Pain. NCBI Bookshelf


















{kind=link}