

Chondromalacia patella is a degenerative change where the hyaline cartilage on the posterior patellar surface loses its normal density and begins to soften. As the cartilage weakens, it becomes more susceptible to tearing, fissuring, and early erosion. These structural changes are often visible on MRI even before symptoms appear, and are sometimes described clinically as chondromalacia patellae.
The condition can develop after trauma, repetitive microtrauma, abnormal loading patterns, or iatrogenic factors such as corticosteroid injections. Chondromalacia patella is more common in women and in individuals with biomechanical factors that increase stress on the patellofemoral joint. It represents one of the earliest forms of patellar cartilage degeneration.
Many people with chondromalacia patella have no symptoms at all. When symptoms do occur, the typical presentation is anterior knee pain, especially during stairs, squatting, or prolonged sitting. Understanding how these cartilage changes progress and how they are classified is essential for early recognition and effective management.
Quick Overview – Chondromalacia Patella
- Chondromalacia patella is the softening and early wear of cartilage on the back of the kneecap, causing anterior knee pain.
- It often results from patellar maltracking, muscle imbalance, or overuse during activities that increase patellofemoral stress.
- Symptoms include dull retropatellar pain, crepitus, and discomfort when climbing stairs, squatting, or sitting for long periods.
- Diagnosis relies on clinical examination and imaging (MRI or arthroscopy) to assess cartilage integrity and patellar alignment.
- Conservative treatment—physiotherapy, quadriceps and hip strengthening, and activity modification—usually leads to full recovery.
- Advanced cases may require surgical realignment or cartilage procedures, but most patients improve without surgery.
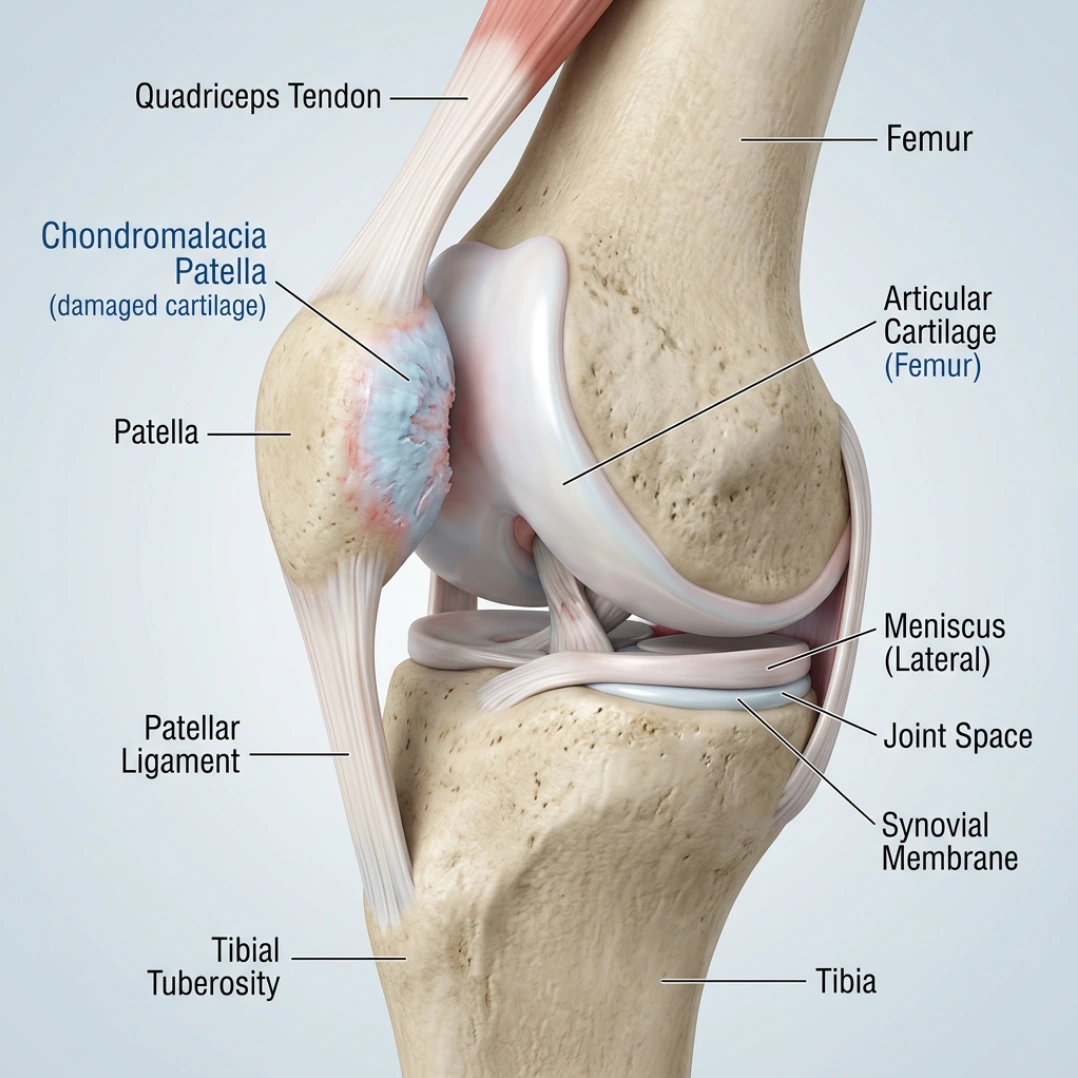
Patellofemoral Joint Anatomy
The patellofemoral joint is formed by the patella and the femoral trochlear groove. It functions as a dynamic gliding interface that increases the mechanical efficiency of the quadriceps and distributes load across the anterior knee. The posterior surface of the patella is covered with thick hyaline cartilage—one of the densest cartilage layers in the human body. Its role is to provide a smooth, low‑friction surface that absorbs load and protects the underlying bone.
During daily activities such as walking, stair climbing, or squatting, the patellofemoral joint is exposed to substantial compressive forces that make it vulnerable to early cartilage changes. Once the cartilage begins to soften, lose density, or develop fissures, the smooth gliding mechanics of the joint become disrupted and movement becomes less efficient.
You are free to share, copy, redistribute, and adapt the content for educational and informational purposes, including commercial use,
as long as proper attribution is given to JointHealthGuide.com and a link to the license is included.
What is Chondromalacia Patella?
Chondromalacia patella refers to the softening and degeneration of the articular hyaline cartilage on the posterior surface of the patella, which articulates with the trochlear groove of the femur. The term chondromalacia originates from the Greek words chrondros (cartilage) and malakia (softening).
In its healthy state, patellar hyaline cartilage appears bluish‑white, smooth, glistening, and resilient. The earliest pathological change in chondromalacia patellae is loss of this sheen — the cartilage becomes dull, sometimes yellowish‑white, soft, swollen, and edematous. Lesions typically appear on the medial patellar facet or just distal to it, measuring roughly half an inch or more in diameter. As the condition progresses, the cartilage undergoes fibrillation, fissuring, fragmentation, and eventual erosion.
Causes of Chondromalacia Patella (Etiology & Pathophysiology)
Chondromalacia patellae develops through several interacting pathways, and the exact pain generator is often multifactorial. The underlying problem is increased mechanical stress on the patellofemoral joint combined with reduced resilience of the patellar hyaline cartilage.
One of the most common reasons is lower limb misalignment, where the leg isn’t positioned in an ideal way during movement. A higher Q‑angle, a patella that sits too high or too low, or foot problems like flat feet can all change how the kneecap tracks. When the patella drifts slightly to the side instead of gliding straight, pressure builds up on one part of the cartilage and wear‑and‑tear speeds up.
Muscle weakness—especially in the quadriceps and hip stabilizers—also plays a major role. If these muscles don’t guide the kneecap properly, it tends to shift laterally, increasing friction and stress inside the joint.
Another important group of causes includes patellar injuries and repetitive microtrauma. A direct hit to the kneecap, previous knee surgery, long periods of immobilization, or repetitive loading from sports can all disrupt normal patellar mechanics. Even small, repeated stresses add up over time and gradually damage the cartilage.
Certain iatrogenic factors, such as specific medications injected into the joint (like high‑dose corticosteroids or bupivacaine), can negatively affect cartilage health and make it more vulnerable to degeneration.
Finally, patellar subluxation—a partial, often subtle slipping of the kneecap—is a frequently overlooked cause. Even if the kneecap doesn’t fully dislocate, repeated episodes of slight shifting create abnormal shear forces that accelerate cartilage breakdown.
The most relevant contributing factors include:
| Cause | Mechanism | Key Details |
|---|---|---|
| Lower Limb Malalignment & Patellar Maltracking | Abnormal patellar glide increases focal cartilage pressure |
|
| Muscular Weakness | Reduced dynamic patellar stabilization |
|
| Patellar Lesions & Microtrauma | Repetitive overload or direct injury damages cartilage |
|
| Iatrogenic Factors | Chondrotoxic substances weaken cartilage |
|
| Patellar Subluxation | Recurrent shear forces damage cartilage |
|
Pathophysiology of Chondromalacia Patella
Hyaline cartilage is composed of chondrocytes embedded in an extracellular matrix of Hyaline cartilage is composed of chondrocytes embedded in an extracellular matrix of type II collagen, proteoglycans, and water. It is avascular, aneural, and alymphatic, relying on diffusion from synovial fluid for nutrition — which explains its poor healing capacity.
Cartilage degeneration occurs due to:
- Biochemical stress Chondrotoxic substances, inflammatory cytokines, proteolytic enzymes (e.g., after infection).
- Mechanical stress Repetitive compressive loading and microtrauma accelerate wear and tear.
- Aging Fewer chondrocytes → fewer proteoglycans → less water → reduced elasticity. The superficial zone degenerates first.
Pain usually originates from the anterior fat pad and joint capsule, not from the cartilage itself.
Pathologically, chondromalacia patella begins with softening, swelling, and edema of the articular cartilage — the earliest visible stage of degeneration.
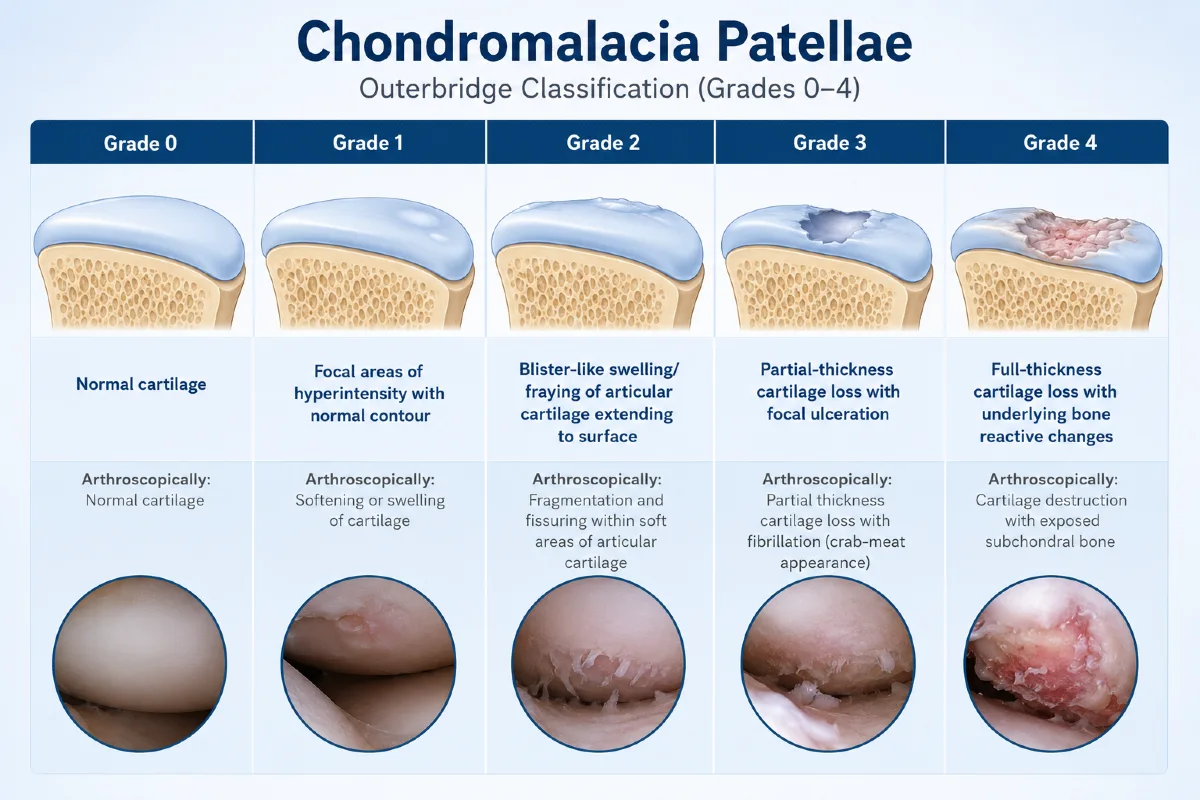
Chondromalacia Patella Grading According to the Outerbridge Classification (Grades 0–4)
The Outerbridge classification is the most widely used system for grading the severity of patellar cartilage damage. Although originally developed for arthroscopic assessment, modern clinical practice most commonly applies this grading system using MRI, which reliably visualizes cartilage softening, fissuring, and full‑thickness defects.
| Grade | Description | Arthroscopic Appearance |
|---|---|---|
| Grade 0 | Normal cartilage | Smooth, intact bluish-white hyaline cartilage |
| Grade 1 | Cartilage softening with preserved surface contour | Softening or swelling of the cartilage surface |
| Grade 2 | Superficial fissures, fragmentation, or blister-like swelling | Fragmentation and fissuring within softened cartilage |
| Grade 3 | Partial-thickness cartilage loss with deep fissuring | Fibrillation with “crab-meat” appearance |
| Grade 4 | Full-thickness cartilage loss with exposed subchondral bone | Complete cartilage destruction with exposed bone and reactive changes |
Symptoms of Chondromalacia Patella
Anterior knee pain is the most common and most characteristic symptom of chondromalacia patella. Patients typically describe a vaguely diffuse, retropatellar or prepatellar ache with a gradual, insidious onset rather than a sharp or localized pain. The discomfort is strongly activity‑dependent and correlates with situations that increase patellofemoral joint stress such as stair climbing, squatting, running, or prolonged sitting.
These symptoms closely overlap with those seen in patellofemoral pain syndrome (PFPS), a broader clinical entity characterized by pain originating from structures around the patellofemoral joint rather than the cartilage itself. While PFPS does not require structural cartilage damage, chondromalacia patella represents one of its potential underlying causes.
Typical symptom pattern
- Anterior knee pain — hallmark symptom
- Pain during stair use (especially descending)
- Pain with squatting or kneeling
- Theatre sign — pain after prolonged sitting
- Pain during running or jumping
- Retropatellar crepitus — grinding sensation behind the patella
- Quadriceps wasting — secondary to pain‑inhibited activation
- Occasional effusion — mild swelling, not always present
Asymptomatic cases are common.
A key clinical point is that chondromalacia patella is frequently detected as an incidental MRI finding and does not necessarily cause symptoms. Large imaging studies have shown that structural cartilage changes may be present even in individuals without knee pain 1.
Pain does not originate from cartilage.
Hyaline cartilage is aneural, meaning it cannot generate pain. Therefore, symptoms attributed to chondromalacia patella usually arise from surrounding pain‑sensitive structures rather than the cartilage itself. The most common sources of anterior knee pain include:
- Infrapatellar (anterior) fat pad
- Synovium
- Joint capsule
Because the cartilage itself cannot produce nociceptive signals, diagnosis of chondromalacia patellae requires careful exclusion of other causes of anterior knee pain, such as patellofemoral pain syndrome, synovial plica syndrome, tendinopathies, and infrapatellar fat pad impingement.
Chondromalacia Patella vs. Patellofemoral Pain Syndrome (PFPS)
Chondromalacia patella and patellofemoral pain syndrome (PFPS) are closely related conditions, but they are not the same thing. Chondromalacia patella refers to structural changes of the patellar cartilage—such as softening, swelling, fissuring, or early degeneration. PFPS, on the other hand, is a clinical pain syndrome characterized by anterior knee pain that arises from the patellofemoral joint and surrounding soft tissues, even when the cartilage is completely normal.
Because both conditions overload the same joint, their symptoms often overlap. Patients with either condition typically report diffuse, retropatellar discomfort that worsens with activities that increase patellofemoral stress, such as stair climbing, squatting, running, or prolonged sitting. However, while PFPS can occur without any cartilage damage, symptomatic chondromalacia patella usually presents with a similar pain pattern that tends to intensify as cartilage degeneration progresses.
In practice, PFPS is considered the broader umbrella term, and chondromalacia patella represents one of its potential structural causes. Distinguishing between the two is important for prognosis, but initial management—focused on biomechanics, muscle balance, and load reduction—is largely similar.
Evaluation of Chondromalacia Patella
Imaging plays an important role in the assessment of chondromalacia patella, especially when symptoms persist or when a structural cause is suspected. Different imaging methods provide different levels of detail, from basic bone evaluation to advanced cartilage visualization.
Each modality has its own strengths and limitations, so understanding what each test can and cannot show is important for correct diagnosis and clinical decision-making.
| Imaging Method | Advantages | Limitations |
|---|---|---|
| X-ray (Radiographs) | First-line and widely available imaging test; useful for detecting advanced cartilage loss, early arthritis, and anatomical abnormalities such as patella alta/baja or patellar tilt. | Cannot visualize early cartilage damage or softening; limited value in early-stage chondromalacia patella. |
| CT Scan | Excellent visualization of patellar alignment and trochlear anatomy; accurately measures TT–TG distance and other alignment abnormalities. | Less sensitive for early cartilage degeneration; involves radiation exposure. |
| MRI Scan | Best and most accurate imaging method for chondromalacia patella; detects cartilage softening, fissures, swelling, bone marrow changes, patellar tracking abnormalities, and trochlear groove morphology. | More expensive and less available than X-rays; examination takes longer. |
| Arthroscopy | Most precise method for directly visualizing cartilage damage and determining its exact severity and location. | Invasive surgical procedure; usually reserved for unclear cases or when surgery is planned. |
| CT Arthrography / Arthrography | Can reveal cartilage defects and joint surface irregularities in more advanced disease stages. | Requires contrast injection and radiation exposure; rarely used today because MRI provides superior information noninvasively. |
Summary
MRI is the most useful imaging modality for suspected chondromalacia patella, as it provides detailed visualization of early cartilage changes and patellar tracking abnormalities.
X-ray and CT are primarily used to assess underlying bony alignment and structural contributors, while arthroscopy remains the definitive method for direct cartilage assessment but is reserved for selected cases.
Treatment of Chondromalacia Patella
Chondromalacia patella does not behave the same way in every patient. Some people show clear cartilage changes on MRI yet remain completely symptom‑free, while others develop noticeable anterior knee pain that tends to worsen as the degree of cartilage softening, fissuring, or fragmentation increases. Although early‑stage chondromalacia may be partially reversible, advanced cartilage damage has very limited self‑repair capacity, which makes early diagnosis and timely intervention especially important.
Because of this variability, there is no single universally accepted treatment. Management must be individualized, but most patients improve with a structured, long‑term conservative program.
1. First‑Line: Long‑Term Conservative Management
A minimum of one year of conservative treatment is recommended before considering surgical options. This approach is supported by clinical evidence showing that early CMP responds well to nonoperative care.
Conservative management includes:
- Activity modification — reducing deep squats, stairs, kneeling, and high‑impact activities that overload the patellofemoral joint.
- NSAIDs as needed — proven to be more effective than steroid injections for symptom relief.
- Physiotherapy focused on:
- closed‑chain, short‑arc quadriceps exercises
- targeted strengthening of the vastus medialis obliquus (VMO)
- hip external rotator and core strengthening
- neuromuscular training to improve patellar tracking
- Quadriceps strengthening — shown to significantly reduce anterior knee pain in early CMP.
- Patellar‑stabilizing braces for patients with maltracking.
- Foot orthotics to reduce excessive pronation and valgus stress.
This combination improves biomechanics, reduces patellofemoral stress, and often prevents progression.
2. Adjunct Therapies
Some clinicians use biologic or injection‑based treatments, but evidence remains inconsistent:
- Platelet‑rich plasma (PRP) — occasionally recommended, but not proven to consistently improve outcomes.
- Prolotherapy — also lacks consistent evidence and is not considered standard care.
These options may be discussed with patients, but expectations must be realistic.
3. Surgical Treatment
Surgery is considered only when symptoms persist despite at least 12 months of optimized conservative management.
Surgical options include:
- Arthroscopic debridement — smoothing fibrillated cartilage; used in a small minority of patients.
- Lateral release with medial realignment — reduces lateral patellar tension and improves tracking.
- Tibial tubercle osteotomy (TTO) — repositions the patellar tendon to improve biomechanics; may accelerate PFJ degeneration in some cases.
- Partial patellectomy — rarely used; total patellectomy is avoided due to major complications.
- Cartilage procedures such as microfracture, drilling, or excision — limited indications and variable outcomes.
Surgery does not “cure” cartilage degeneration but may reduce pain and improve function in carefully selected patients.
4. Regenerative Medicine (Emerging Options)
Traditional surgeries do not regenerate cartilage, which is why research has shifted toward cell‑based therapies.
Autologous Chondrocyte Implantation (ACI / MACI)
Studies show that chondrocyte implantation can improve symptoms in CMP, with MACI demonstrating better outcomes and easier surgical technique compared to classic ACI.
Mesenchymal Stem Cell (MSC) Therapy
MSCs may help by:
- reducing inflammation
- stimulating cartilage matrix production
- supporting regeneration through paracrine signaling
Early studies show promising improvements in pain, function, and MRI appearance, but long‑term evidence is still evolving and results are not yet consistent across trials.
Summary
Chondromalacia patella is a condition with highly variable presentation. Some patients remain asymptomatic, while others develop significant anterior knee pain that correlates with the severity of cartilage damage. Because advanced cartilage has minimal ability to repair itself, early diagnosis and long‑term conservative management remain the foundation of treatment. Most patients improve without surgery, while regenerative therapies offer promising—but still developing—future options.
Prognosis
The prognosis of chondromalacia patella is generally favorable, but it varies widely from person to person. Chondromalacia patellae may be reversible, or it could progress to the development of patellofemoral osteoarthritis, depending on the severity of cartilage changes and the patient’s biomechanics. Many individuals—especially those with mild or early‑stage disease—experience significant improvement with proper rehabilitation, and patients with knee pain resulting from chondromalacia patella often achieve full recovery.
Recovery timelines differ. Some patients improve within a few weeks, while others require many months of consistent rehabilitation. Teenagers and young adults often have the best long‑term outlook because their musculoskeletal system is still developing, and symptoms frequently diminish as they reach adulthood.
Therapeutic exercises rarely worsen symptoms when performed correctly. If a particular activity aggravates pain, the patient and clinician should work together to adjust the frequency, duration, or intensity—or temporarily avoid the activity until symptoms settle. Long‑term success depends on maintaining good lower‑limb strength, avoiding overload, and recognizing early warning signs before symptoms escalate.
Overall, most patients improve without surgery, and only a small minority progress to persistent pain or patellofemoral osteoarthritis. Early diagnosis, load management, and targeted strengthening remain the key predictors of a positive outcome.
Living With Chondromalacia Patella
Living with chondromalacia patella requires a balance between staying active and avoiding movements that overload the patellofemoral joint. Most patients can maintain a normal lifestyle by understanding their triggers and adapting daily habits to reduce stress on the kneecap.
Activities that involve deep knee flexion—such as squatting, kneeling, or descending stairs—often increase patellofemoral pressure and may provoke symptoms. Adjusting technique, reducing repetition, or temporarily limiting these movements can significantly reduce discomfort. Prolonged sitting with bent knees can also cause stiffness or aching; taking brief standing or stretching breaks helps prevent the “theatre sign.”
Strengthening the quadriceps, hips, and core remains essential for long‑term control of symptoms. These exercises improve patellar tracking and reduce joint stress during everyday tasks. Supportive footwear or orthotics can help individuals with excessive pronation, while patellar‑stabilizing braces may benefit those with maltracking.
Most importantly, patients should learn to recognize early signs of overload—such as increased stiffness, swelling, or a dull ache after activity—and adjust their routine before symptoms escalate. With consistent rehabilitation and mindful activity modification, the majority of individuals can remain active, participate in sports, and maintain a high quality of life despite having chondromalacia patella.
Habusta SF, Coffey R, Ponnarasu S, et al. Chondromalacia Patella. StatPearls [Internet]. Updated 2023 Apr 22. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. StatPearls: Evidence-based overview of chondromalacia patella
Zheng W, Li H, Hu K, et al. Chondromalacia patellae: current options and emerging cell therapies. Stem Cell Research & Therapy. 2021;12:412. Review: Pathophysiology and emerging regenerative treatments
Radiopaedia. Chondromalacia patellae. Imaging guide: MRI appearance and grading of cartilage damage
Cole BJ, Malek MM. Articular Cartilage Lesions. Springer, 2004. ISBN: 9780387955407. Textbook: Knee articular cartilage pathology and classification systems
Jungius K, Schmid MR, Zanetti M, et al. Cartilaginous Defects of the Femorotibial Joint: MR Imaging Accuracy. Radiology. 2006;240(2):482–488. Study: MRI accuracy in detecting cartilage defects of the knee
Aysin IK, Askin A, Mete BD, et al. Relationship between anterior knee pain and chondromalacia patellae. Eurasian Journal of Medicine. 2018;50(1):28–33. Clinical study: Patellofemoral malalignment and cartilage changes
Elson DW, Jones S, Caplan N, et al. Association between anterior knee pain and patellofemoral lesions. The Knee. 2013;20(6):471–475. Study: Incidental patellofemoral cartilage lesions in knee pain patients
Jensen DB, Albrektsen SB. The natural history of chondromalacia patellae: a 12-year follow-up. Acta Orthopaedica Belgica. 1990;56(2):503–506. Long-term study: Natural progression of chondromalacia patella

















