

Cervical spondylosis is a common age-related condition that refers to degenerative changes in the cervical spine (the neck), including disc degeneration, the formation of bone spurs (osteophytes), and reduced spinal mobility. It represents one of the most frequent forms of spinal degeneration, particularly in adults over the age of 50.
In many cases, cervical spondylosis does not cause noticeable symptoms. However, as these degenerative changes progress, they may begin to affect nearby nerves or even the spinal cord. This can lead to neurological complications such as cervical radiculopathy (nerve root compression) and cervical myelopathy (spinal cord compression).
In this article, we will explain what cervical spondylosis is, how it develops, and which symptoms it can cause. We will also explore the key differences between radiculopathy and myelopathy, including why some forms of the condition are more serious than others.
Key Clinical Points – Cervical Spondylosis
- Cervical spondylosis is a common degenerative condition of the cervical spine involving disc degeneration, osteophyte formation, and reduced spinal mobility.
- It most often affects the neck region due to its high mobility and mechanical load, making it particularly prone to age-related wear and tear.
- In many cases, cervical spondylosis is asymptomatic, but it can lead to pain and stiffness or neurological complications when nerve structures are involved.
- Cervical radiculopathy occurs when a nerve root is compressed, causing radiating arm pain, tingling, numbness, or weakness.
- Cervical myelopathy is a more serious condition caused by spinal cord compression, leading to gait instability, hand dysfunction, and progressive neurological deficits.
- Diagnosis is based on clinical examination and imaging, with MRI being the most important tool for assessing nerve and spinal cord involvement.
- Treatment is usually conservative, including medication, physical therapy, and exercise, while surgery is reserved for severe or progressive cases, especially in myelopathy.
What Is Cervical Spondylosis?
Cervical spondylosis refers to degenerative changes affecting the structures of the cervical spine (the neck), including the intervertebral discs, vertebral bodies, facet joints, and surrounding ligaments. These changes typically involve progressive disc degeneration, the formation of bone spurs (osteophytes), and a gradual reduction in spinal mobility.
The cervical spine is particularly susceptible to spondylotic changes due to its unique structure and function. Unlike other parts of the spine, it must support the weight of the head while allowing a high degree of movement, including rotation, flexion, and extension. This combination of mobility and mechanical load makes the cervical spine more vulnerable to wear and tear over time.
As degenerative changes progress, they may alter the normal alignment and stability of the spine. In some cases, this can lead to narrowing of the spaces where nerves exit the spine or even compression of the spinal cord, which explains why cervical spondylosis can sometimes be associated with neurological symptoms.
How Cervical Spondylosis Develops
Cervical spondylosis develops gradually over time as a result of age-related changes and mechanical stress in the cervical spine. The process typically begins with degeneration of the intervertebral discs, which lose water content, elasticity, and height.
As the discs deteriorate, their ability to absorb load decreases. This leads to increased mechanical stress on the adjacent vertebrae and facet joints. In response, the body forms bony outgrowths known as osteophytes, which may help stabilize the spine but can also contribute to structural changes.
At the same time, disc degeneration reduces segmental stability, placing additional strain on the facet joints and surrounding ligaments. This can lead to joint degeneration, ligament thickening, and further narrowing of the available space within the spine.
Over time, these combined changes—disc degeneration, osteophyte formation, and reduced stability—may result in narrowing of the spinal canal or the openings where nerve roots exit. When this occurs, nearby nerves or even the spinal cord can become compressed, which explains the development of neurological symptoms in more advanced stages of cervical spondylosis.
Symptoms of Cervical Spondylosis
Not all cases of cervical spondylosis cause symptoms. In fact, many people have degenerative changes visible on imaging without experiencing any pain or functional problems. When symptoms do occur, they typically develop gradually and may vary depending on whether only the local structures are affected or if there is compression of neural elements.
1. Neck Pain and Stiffness
The most common symptoms of cervical spondylosis are neck pain and stiffness. This discomfort is usually mechanical in nature and tends to worsen with prolonged sitting, poor posture, or repetitive neck movements.
Patients often describe a dull, aching pain in the neck, sometimes accompanied by reduced range of motion. The pain may radiate to the shoulders or upper back but typically does not extend into the arms unless nerve involvement is present. In many cases, symptoms improve with rest or changes in position.
These symptoms are primarily related to degenerative changes in the intervertebral discs, facet joints, and surrounding soft tissues, rather than direct nerve compression.
2. Neurological Symptoms
As cervical spondylosis progresses, degenerative changes may begin to affect nearby nerves or the spinal cord. When this happens, neurological symptoms can develop, representing more advanced forms of the condition.
The two main neurological complications are:
- Cervical radiculopathy, which occurs when a nerve root is compressed or irritated
- Cervical myelopathy, which results from compression of the spinal cord
These conditions can lead to symptoms such as pain radiating into the arms, tingling, numbness, weakness, or problems with coordination and balance. Because they involve neural structures, they are generally more clinically significant than isolated neck pain and may require further evaluation and treatment.
Clinical Insight
If symptoms are limited to neck pain and stiffness without radiation into the arms or neurological deficits, cervical spondylosis is most likely presenting as a mechanical condition. However, the presence of arm pain, tingling, weakness, or coordination problems suggests nerve root or spinal cord involvement, such as cervical radiculopathy or myelopathy.
In the following sections, we will examine cervical spondylosis with radiculopathy and myelopathy in more detail.
Cervical Spondylosis with Radiculopathy
Cervical radiculopathy occurs when degenerative changes in the cervical spine lead to compression or irritation of a nerve root as it exits the spinal canal. In cervical spondylosis, this most commonly results from age-related structural changes such as disc degeneration and the formation of osteophytes, which can narrow the intervertebral foramina where the nerve roots pass.
Symptoms
The hallmark of cervical radiculopathy is radiating pain from the neck into the upper limb. This pain typically follows a specific nerve distribution and may extend into the shoulder, arm, or hand.
Common symptoms include:
- Pain radiating from the neck into the arm
- Tingling or “pins and needles” sensations in the upper limb
- Numbness in specific dermatomal patterns
- Muscle weakness in the affected arm or hand
Symptoms may worsen with certain neck movements, such as extension or rotation, which can further narrow the foraminal space and increase nerve irritation.
Causes
In cervical spondylosis, radiculopathy most commonly develops due to:
- Herniated intervertebral disc – more frequent in younger patients, where disc material protrudes and compresses the nerve root
- Osteophyte formation (bone spurs) – more common in older individuals, where degenerative changes lead to gradual narrowing of the nerve exit pathways
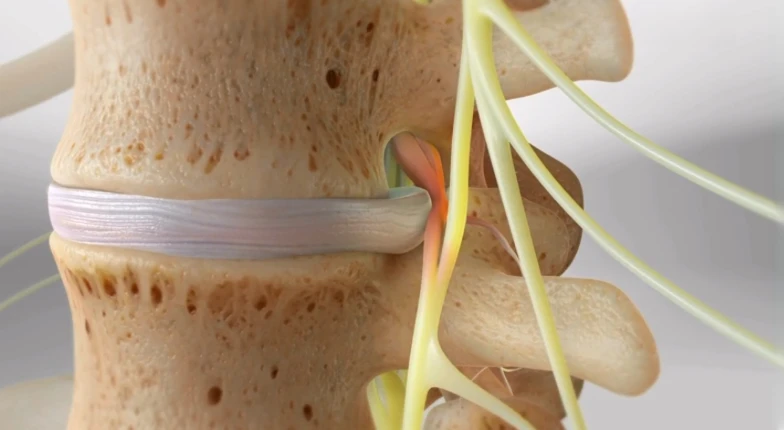
In many cases, both disc degeneration and osteophytes contribute to nerve root compression, resulting in a combination of mechanical and degenerative factors.
Cervical Spondylosis with Myelopathy
Cervical myelopathy is a condition that occurs when degenerative changes in the cervical spine lead to compression of the spinal cord. In the context of cervical spondylosis, this compression is typically caused by a combination of disc degeneration, osteophyte formation, ligament thickening, and reduced space within the spinal canal.
Unlike radiculopathy, which affects individual nerve roots, myelopathy involves the spinal cord itself, which is responsible for transmitting signals between the brain and the rest of the body. For this reason, it is considered a more serious and potentially progressive form of cervical spondylosis.
Symptoms
Cervical myelopathy usually develops gradually and may initially present with subtle neurological changes. Common symptoms include:
- Difficulty with fine motor skills (e.g., buttoning clothes, writing, or handling small objects)
- Gait instability or unsteady walking
- Weakness in the arms and/or legs
- Clumsiness or reduced hand coordination
In more advanced cases, patients may also experience sensory disturbances and increased tendency to fall. Neck pain may be absent or only mild, which can sometimes delay recognition of the condition.
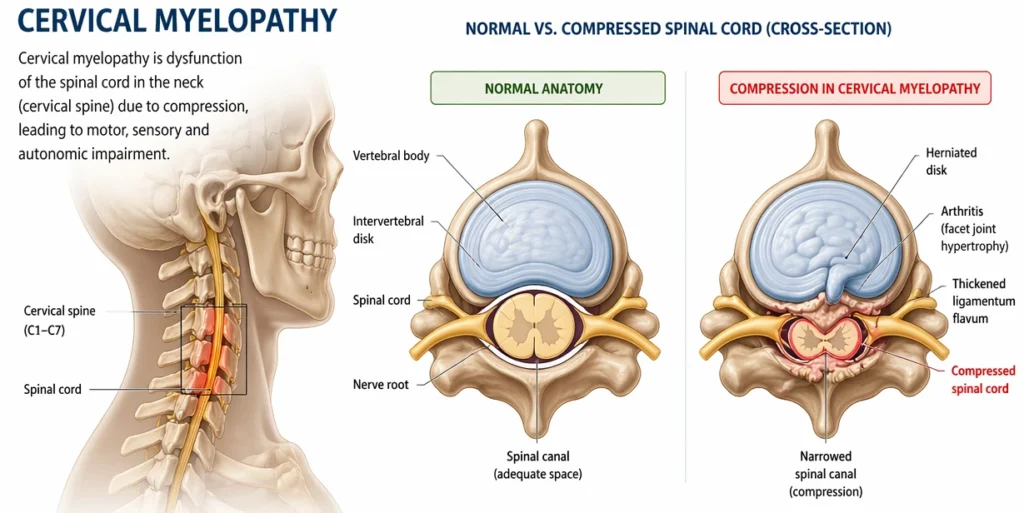
This image may be freely used for educational or editorial purposes, provided proper attribution is given to the original source (jointhealthguide.com)
Progression and Clinical Significance
Cervical myelopathy is typically a progressive condition. Without appropriate diagnosis and management, symptoms may worsen over time as spinal cord compression increases. This can lead to more pronounced functional impairment, including significant gait disturbance and loss of hand dexterity.
Because the spinal cord is involved, cervical myelopathy is generally considered more clinically significant than cervical radiculopathy. Early recognition is important, as prolonged compression may result in irreversible neurological deficits.
For this reason, patients with suspected myelopathy often require further imaging, typically MRI, and specialist evaluation to determine the extent of spinal cord involvement and the need for more advanced treatment options (surgery).
Cervical Radiculopathy vs Myelopathy
Cervical radiculopathy and cervical myelopathy differ primarily in the anatomical structure affected and the resulting clinical presentation.
Radiculopathy involves compression of a nerve root, typically causing unilateral symptoms such as neck pain radiating into one arm, along with tingling, numbness, or localized weakness.
Myelopathy, on the other hand, results from compression of the spinal cord, leading to more widespread neurological dysfunction, including gait instability, hand clumsiness, and difficulty with fine motor tasks.
In general, radiculopathy is less severe and often responsive to conservative treatment, while myelopathy is a more serious and potentially progressive condition that may require closer monitoring and specialist evaluation.
| Condition | Affected Structure | Typical Symptoms | Severity |
|---|---|---|---|
| Cervical Radiculopathy | Nerve root (peripheral nerve exit) | Neck pain radiating into one arm, tingling, numbness, localized weakness | Mild to moderate; often manageable with conservative treatment |
| Cervical Myelopathy | Spinal cord (central nervous system) | Gait instability, hand clumsiness, fine motor difficulty, limb weakness | Moderate to severe; potentially progressive and functionally limiting |
Diagnosis
Cervical spondylosis is diagnosed through a combination of clinical evaluation and imaging studies. Because degenerative changes are common even in asymptomatic individuals, diagnosis is based on correlating symptoms with objective findings.
A clinical examination is the first step and includes assessment of neck mobility, neurological function, muscle strength, reflexes, and signs of nerve root or spinal cord involvement.
Imaging plays a key role in confirming the diagnosis and identifying the extent of structural changes:
- MRI (Magnetic Resonance Imaging) is the most important method for evaluating soft tissues, including intervertebral discs, nerve roots, and the spinal cord. It is especially useful for detecting nerve or spinal cord compression in cases of radiculopathy or myelopathy.
- CT (Computed Tomography) provides detailed visualization of bony structures and is useful for assessing osteophytes and foraminal narrowing.
- X-rays can show general degenerative changes such as disc space narrowing and bone spur formation but offer limited information about soft tissue involvement.
In most cases, MRI is preferred when neurological symptoms are present, while X-rays may be sufficient for initial evaluation of mild or non-specific neck pain.
Treatment of Cervical Spondylosis
Treatment of cervical spondylosis depends on the severity of symptoms and whether neurological structures such as nerve roots or the spinal cord are involved. In most cases, management is conservative, with surgery reserved for more advanced or progressive conditions.
Conservative Treatment
The majority of patients with cervical spondylosis are treated non-surgically, especially when symptoms are mild and there is no significant neurological impairment.
Common conservative approaches include:
- Medications – such as analgesics and non-steroidal anti-inflammatory drugs (NSAIDs) to reduce pain and inflammation
- Physical therapy – aimed at improving neck mobility, reducing muscle tension, and supporting spinal function
- Exercise therapy – including targeted neck and postural exercises to strengthen supporting muscles and improve stability
These methods are often effective in controlling symptoms such as neck pain and stiffness, particularly when no nerve compression is present.
When Surgery Is Needed?
Surgical treatment is considered when conservative therapy fails or when there is evidence of significant neurological involvement.
It is particularly important in cases of cervical myelopathy, where spinal cord compression can lead to progressive neurological deficits. Surgery may also be indicated in severe or persistent radiculopathy that does not respond to non-surgical treatment.
Clinical Insight
The main goal of surgery in cervical spondylosis is to decompress the affected neural structures, particularly the spinal cord or nerve roots, in order to prevent further neurological deterioration and preserve long-term function.
When to See a Doctor
Most cases of cervical spondylosis can be managed conservatively, especially when symptoms are mild and limited to neck pain or stiffness. However, medical evaluation is important when symptoms suggest nerve root or spinal cord involvement.
You should seek medical attention if you experience:
- Progressive weakness in the arms or hands
- Difficulty with walking or loss of balance
- Problems with fine motor skills, such as buttoning clothes or writing
- Persistent or worsening neurological symptoms
These signs may indicate cervical radiculopathy or cervical myelopathy and require further assessment, typically with MRI, to determine the extent of nerve or spinal cord compression.
FAQ
Is cervical spondylosis serious?
In most cases, cervical spondylosis is not serious and represents a normal part of aging. However, it can become clinically significant if it leads to nerve root or spinal cord compression, resulting in radiculopathy or myelopathy.
What is the difference between radiculopathy and myelopathy?
Cervical radiculopathy involves compression of a nerve root, causing symptoms such as pain, tingling, or weakness in one arm. Cervical myelopathy involves compression of the spinal cord and typically causes more widespread symptoms, including gait instability, coordination problems, and hand dysfunction.
Can cervical spondylosis cause arm pain?
Yes. Cervical spondylosis can cause arm pain when degenerative changes lead to compression or irritation of a nerve root. This condition is known as cervical radiculopathy.
Does cervical spondylosis always require surgery?
No. Most cases are managed without surgery using conservative treatments such as medication, physical therapy, and exercise. Surgery is typically reserved for severe or progressive cases, especially when cervical myelopathy is present or when symptoms do not improve with non-surgical treatment.
Kuo DT, Tadi P. Cervical Spondylosis. StatPearls [Internet]. NCBI Bookshelf: Cervical spondylosis clinical overview and pathophysiology
Margetis K, Donnally III CJ. Cervical Myelopathy. StatPearls [Internet]. NCBI Bookshelf: Cervical myelopathy diagnosis, symptoms, and management
BMJ. Degenerative cervical myelopathy. BMJ 2018;360:k186. BMJ clinical review: Degenerative cervical myelopathy overview and evidence
Margetis K, Magnus W, Mesfin FB. Cervical Radiculopathy. StatPearls [Internet]. NCBI Bookshelf: Cervical radiculopathy causes, symptoms, and treatment
Kang KC, Lee HS, Lee JH. Cervical Radiculopathy: Focus on Characteristics and Differential Diagnosis. Asian Spine J. Asian Spine Journal: Clinical features and differential diagnosis of cervical radiculopathy
BMJ Best Practice. Cervical radiculopathy. BMJ clinical decision guide: Cervical radiculopathy assessment and management

















