A rotator cuff tear, also known as a shoulder tendon rupture, refers to damage of one or more tendons of the rotator cuff in the shoulder. A torn rotator cuff is a common cause of both acute and chronic shoulder pain. In addition to pain, this type of rotator cuff injury often leads to muscle weakness and functional impairment.
As a result, many everyday activities — such as combing hair, getting dressed, or reaching overhead — can become painful and difficult to perform.
A rotator cuff tear can occur in individuals of all age groups; however, its incidence increases with age and it is most commonly seen in older adults.
In this article, we will explain in detail what causes a rotator cuff injury, how to recognize the symptoms of a torn rotator cuff, which diagnostic methods are used, and what treatment options are available — from conservative management to surgical repair.
What Is the Rotator Cuff?
The rotator cuff is a group of four muscles whose tendons join together to form a “cuff” or covering over the head of the humerus (the upper part of the upper arm bone).
The rotator cuff is composed of the following muscles:
- Supraspinatus
- Subscapularis
- Infraspinatus
- Teres minor
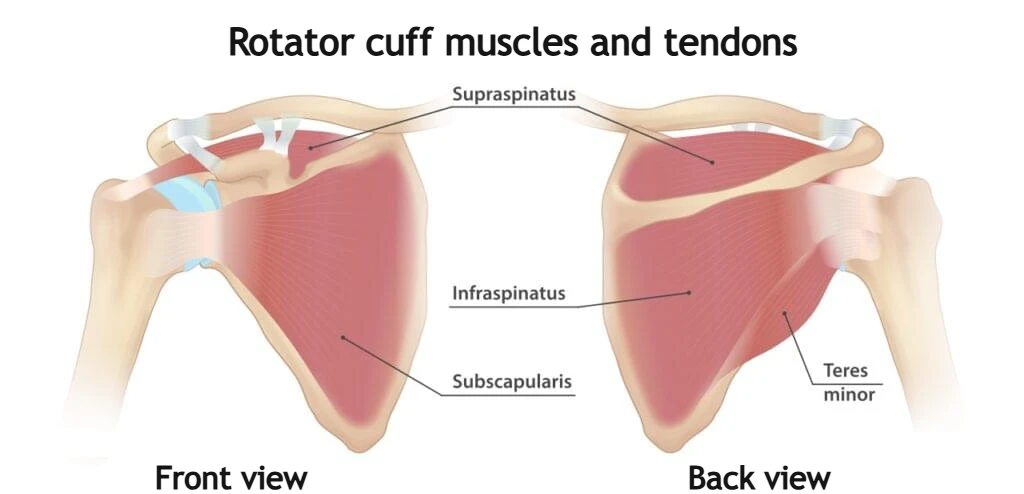
All of these muscles originate from the scapula (shoulder blade) and attach to the head of the humerus at bony prominences known as the greater and lesser tuberosities.
Thanks to its anatomical structure, the shoulder is the most mobile joint in the human body. However, this high level of mobility comes at a price. Due to its wide range of motion, the shoulder joint is more vulnerable to tendon and cartilage injuries during everyday activities.
For proper shoulder function, it is essential that the head of the humerus remains perfectly centered within the glenoid during movement. Shoulder stability is provided by strong ligaments, the joint capsule, and the rotator cuff muscles, which surround the humeral head from all sides.
In addition to enabling arm movement, the rotator cuff muscles have an even more important role — stabilizing the humeral head within the glenoid during motion. When stabilization is inadequate, the humeral head may shift upward toward the acromion during arm elevation. This can lead to irritation and injury of the shoulder tendons and bursae.
Why Does a Rotator Cuff Tear Occur?
There are two main causes of a rotator cuff tear:
- Injury – acute rotator cuff tear
- Degeneration – rotator cuff tear related to chronic tendon wear
Acute injuries usually occur as a result of a single traumatic incident. Degenerative tears, on the other hand, develop due to long-term tendon wear associated with aging or repetitive overload.
1. Acute Rotator Cuff Tear (Injury)
A rotator cuff injury can occur as a result of traumatic events such as a fall onto an outstretched arm, a fall from a bicycle or motorcycle onto the shoulder, a sports-related fall directly onto the shoulder, or a direct blow to the shoulder.
In younger individuals, even a healthy tendon can rupture due to significant trauma. In older adults, a degeneratively weakened tendon may tear more easily under stress. These injuries are often associated with high-force mechanisms, and other shoulder injuries may be present at the same time, such as:
- Shoulder dislocation
- Clavicle fracture
- Wrist fracture
In a certain number of younger patients, surgical treatment involving tendon repair (reconstruction and reattachment of the tendon) may be necessary.
2. Degenerative Rotator Cuff Tear
A rotator cuff tear caused by tendon degeneration develops gradually over a longer period of time as a result of chronic “wear and tear.” This type of tear is much more common than acute traumatic rupture and primarily affects older individuals.
With aging, degenerative changes naturally occur in joints and tendons. During tendon degeneration, structural changes develop within the tendon tissue — the tendon fibers become less organized and the overall strength of the tendon decreases. Chronic degenerative changes of the tendon are referred to as tendinopathy.
Long-term tendon overload, combined with aging, further contributes to tendon degeneration and gradual deterioration. A degeneratively altered tendon is weaker than a healthy tendon and therefore more prone to tearing.
A degenerative torn rotator cuff most often develops spontaneously during normal daily activities. Many patients are unable to identify the exact moment when the rupture occurred.
The strong association between age and rotator cuff injury is reflected in epidemiological data: at the age of 60, approximately 30% of individuals have a rotator cuff tear, while this percentage rises to about 60% among people aged 80.
Factors Contributing to Degenerative Rotator Cuff Tears
Several factors contribute to chronic or degenerative rotator cuff tears:
Repetitive stress on the tendon
Repeating the same shoulder movements over and over can overload the rotator cuff muscles and tendons. Sports such as baseball, tennis, rowing, and weightlifting are examples of activities that may increase the risk of overuse-related tearing. Many occupations and routine daily tasks can also lead to overuse injuries.
Reduced blood supply
As we age, blood supply to the rotator cuff tendons decreases. Without adequate blood flow, the body loses its natural ability to repair tendon damage, which can eventually result in a tear.
Bone spurs (osteophytes)
Bone spurs, particularly those located on the underside of the acromion, can contribute to the development of shoulder impingement syndrome. During arm elevation, the tendon may rub against the bone. If this impingement becomes chronic, it leads to increased tendon wear and may ultimately result in a rotator cuff tear.
Rotator Cuff Tear Risk Factors
The most significant risk factors for degenerative rotator cuff tears include:
- Age
As we grow older, degeneration of our tendons naturally progresses. After the age of 40, the risk of developing a rotator cuff tear increases significantly. - Smoking
Smoking negatively affects cardiovascular health and impairs blood supply to the tendons. It also causes oxidative stress, which adversely impacts tendon health and healing capacity. - Family predisposition
If close relatives have experienced shoulder tendon problems — especially before the age of 40 — your likelihood of developing similar issues is higher. - Poor posture
Poor posture is another important risk factor for rotator cuff tears. Studies have shown that tears are present in approximately 50% of individuals with poor posture, compared to only about 3% of those with good posture. - Occupation or sports activities
People who regularly lift heavy loads or perform overhead activities are at increased risk of rotator cuff injury. Certain athletes are particularly vulnerable due to repetitive overuse, especially tennis players, baseball players, rowers, and wrestlers. Painters, carpenters, electricians, and others whose work involves frequent overhead activity also have a higher likelihood of developing a rotator cuff tear.
What Types of Rotator Cuff Tears Exist?
A rotator cuff tear means that the tendon is partially or completely detached from its insertion on the head of the humerus. Most tears occur in the supraspinatus tendon (approximately 90% of cases), although other rotator cuff tendons may also be involved.
In terms of frequency, supraspinatus tears are followed by infraspinatus tears and then subscapularis tears.
In many cases of degenerative rotator cuff tears, a small initial injury develops first and gradually enlarges over time. As the damage progresses, the tendon may eventually rupture completely, either spontaneously during everyday activities or while lifting a heavy object.
In acute, traumatic rotator cuff injury, the site of injury is often located at the musculotendinous junction (where the tendon meets the muscle) or within the so-called critical zone, which lies slightly proximal to the tendon’s insertion on the bone.
Classification of Tears by Extent of Tendon Damage
Based on the severity or extent of damage, rotator cuff tears are divided into:
- Partial-thickness tears
- Full-thickness tears
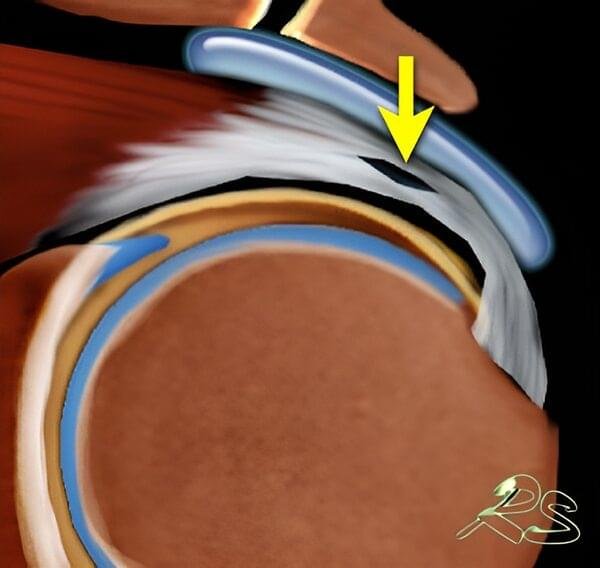
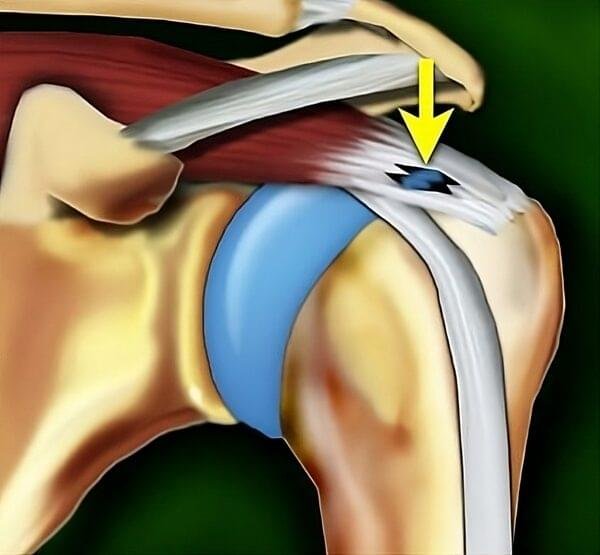
Partial Rotator Cuff Tear
In this type of tear, the tendon damage involves only part of the tendon and does not extend through its entire thickness — this is referred to as a partial-thickness rotator cuff tear. The tendon remains attached to its insertion on the humerus but is thinned and structurally weakened.
According to the location of the damage, partial tears can be classified as:
- Intrasubstance tear
Tendon fibers rupture within the substance of the tendon, creating a cavity. However, the damage does not extend to the surface of the tendon and is not visible externally. - Bursal-sided tear
The damage occurs on the upper (bursal) side of the tendon, which is in contact with the subacromial bursa. These tears are less common than intrasubstance tears and articular-sided tears. They are often associated with shoulder impingement, where the tendon rubs against the undersurface of the acromion during shoulder movement. The presence of bone spurs (osteophytes) on the inferior surface of the acromion is considered a risk factor, as they may mechanically irritate the tendon. - Articular-sided tear
The damage occurs on the lower (articular) side of the tendon, facing the shoulder joint and the humeral head. Certain athletes, such as baseball pitchers and tennis players, are at increased risk of developing this type of tear.

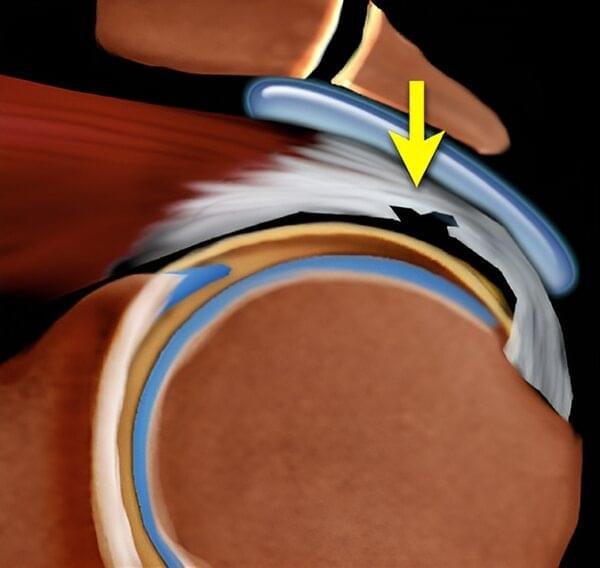

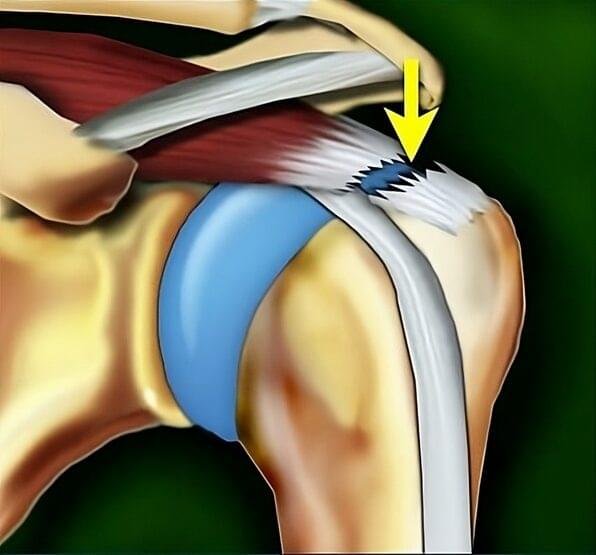
Full-Thickness Rotator Cuff Tear
In this type of tear, the tendon damage extends through the entire thickness of the tendon — a full-thickness rotator cuff tear. Essentially, a hole is created in the tendon.
In degenerative tears, the rupture site is usually located at the tendon’s insertion on the bone, resulting in partial or complete detachment of the tendon from the humerus.
- Incomplete full-thickness tear
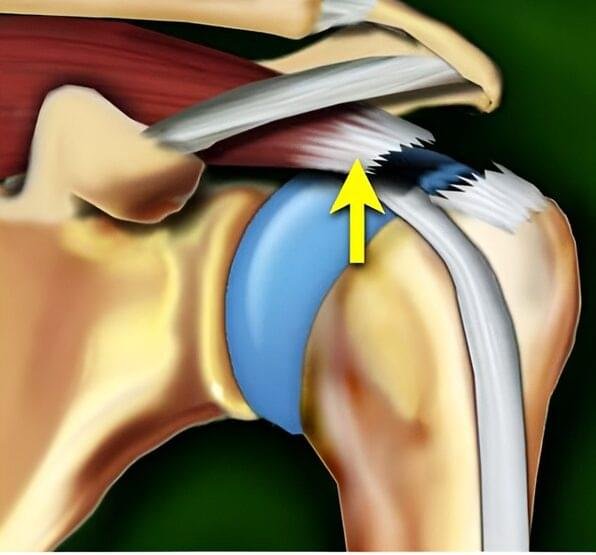
Only a small portion of the tendon is detached from the bone. The tendon largely retains its function. - Complete full-thickness tear
The tendon is completely detached from the bone. When a complete full-thickness tear is present, nothing connects the muscle to the bone, and the muscle becomes functionally inactive.
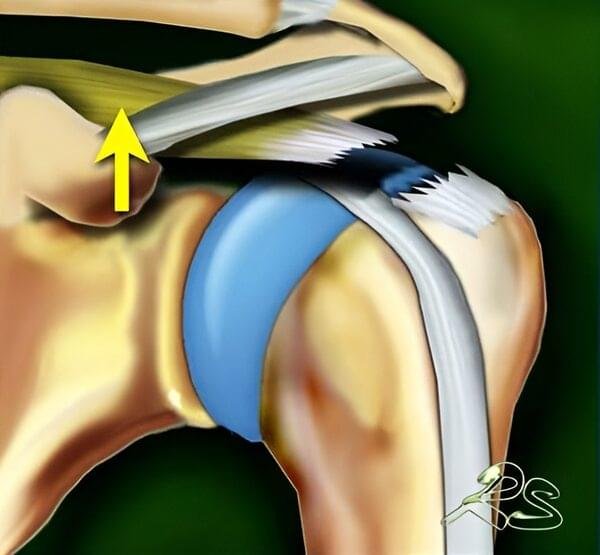
Massive Rotator Cuff Tear
A massive rotator cuff tear refers to a full-thickness rupture involving multiple rotator cuff tendons. This condition leads to significant shoulder instability and disruption of normal shoulder joint biomechanics.
Rotator Cuff Tear Symptoms
The main reason patients seek medical attention is shoulder pain. Interestingly, about 50% of individuals with a rotator cuff tear may not experience significant pain. However, when symptoms are present, they can considerably affect daily function and quality of life.
Common rotator cuff tear symptoms include:
- Shoulder pain, which is typically more pronounced during active movement, especially when lifting the arm above shoulder level. Everyday activities such as reaching for a shelf, hanging laundry, combing or drying hair, or fastening a seatbelt can become extremely painful. As the condition progresses, pain may also occur at rest.
- Night pain, particularly when lying on the affected shoulder.
- Pain radiating from the shoulder into the upper arm, often extending toward the elbow.
- Weakness when lifting or rotating the arm, a common sign of a more advanced torn rotator cuff.
- A grinding, clicking, or catching sensation during shoulder movement. This symptom can occasionally occur even in a healthy shoulder, but it is frequently reported in cases of rotator cuff injury.
Pain may appear suddenly after a traumatic event, such as a fall, and is usually intense in acute cases of a torn rotator cuff. In contrast, pain related to a degenerative rotator cuff injury typically develops gradually. It is often mild at first but progressively worsens over time. Active individuals often seek medical evaluation when they are no longer able to participate in sports or perform work-related activities.
Recent studies suggest that shoulder pain is not strongly correlated with the size or type of rotator cuff tear. Even large tears may sometimes cause minimal discomfort, while smaller tears can be very painful.
Many patients initially attempt to adapt by modifying their activities and shoulder movements. They may change the way they lift their arm, adjust how they carry heavy objects, or avoid certain positions altogether. Depending on when medical attention is sought, different stages of tendon damage may be present — ranging from tendinopathy, to a partial tear, and eventually to a complete torn rotator cuff.
How to Tell If You Tore Your Rotator Cuff
After reviewing the common rotator cuff tear symptoms, many patients ask a practical question: How can I tell if I tore my rotator cuff?
While a definitive diagnosis requires medical evaluation and imaging, certain signs strongly suggest a torn rotator cuff, especially when they appear after an injury or progressively worsen over time.
You may have a rotator cuff tear if you experience:
- Sudden shoulder pain after a fall or trauma, followed by immediate weakness
- Inability to lift your arm, particularly above shoulder level
- Significant weakness when trying to rotate the arm outward or lift it sideways
- A noticeable loss of strength, even when pain is not severe
- Persistent night pain, especially when lying on the affected side
- A clicking or catching sensation combined with weakness
One of the most telling signs of a more serious rotator cuff injury is weakness that does not improve with rest. Many people with simple tendon inflammation (tendinopathy) can still lift their arm despite pain. However, in cases of a larger or complete rotator cuff tear, the arm may feel heavy, unstable, or difficult to control.
In acute cases, such as after a fall on an outstretched arm, patients often describe a sharp tearing sensation followed by immediate difficulty raising the arm. In degenerative cases, symptoms may begin gradually with mild discomfort and slowly progress to weakness and limited function.
It is important to note that some individuals with a torn rotator cuff may have surprisingly mild pain, which is why persistent weakness should never be ignored.
If you suspect a rotator cuff tear — especially if you cannot lift your arm, have ongoing night pain, or notice progressive weakness — a medical evaluation is recommended. Early diagnosis of a rotator cuff injury improves treatment outcomes and may prevent further tendon damage.
How Is a Rotator Cuff Injury Diagnosed?
The diagnosis of a rotator cuff tear is based on a detailed medical history (anamnesis), physical examination, and imaging studies.
Medical History
A thorough conversation between the physician and the patient regarding shoulder pain is essential for diagnosing a rotator cuff injury. Important details include:
- The nature of the shoulder pain — when it started, its characteristics, and factors that worsen or relieve it
- Any previous treatments undertaken and their outcomes
- A history of prior injuries to the affected shoulder or upper limb
This information often helps differentiate between an acute torn rotator cuff and a degenerative condition.
Physical Examination
After obtaining a detailed history, the physician (often a specialist in physical and rehabilitation medicine) will examine the shoulder, assessing:
- Deformity or asymmetry of the shoulder. In cases of massive rotator cuff tear, a visible depression may be present due to muscle atrophy.
- Tenderness to palpation, especially at the tendon insertion on the humerus, which is common in both tendinopathy and rotator cuff tear.
- Range of motion in all directions. In general, and particularly in massive tears, patients may be unable to fully raise the arm due to weakness and pain.
- Muscle strength of the rotator cuff. Strength is often reduced in complete tears.
- Other shoulder joint conditions, such as arthritis (especially in individuals over 75), which may also cause pain and restricted movement.
- Cervical spine issues, including nerve root compression, which can cause pain radiating to the shoulder and arm.
- Scapular dyskinesis, a disturbance in the normal movement of the shoulder blade, often present in chronic shoulder pain. This term refers to abnormal motion or partial detachment of the scapula from the chest wall during shoulder movement.
The physician will also perform several specific shoulder tests to further evaluate the integrity of the rotator cuff and identify signs of a torn rotator cuff.
While medical history and physical examination strongly suggest the diagnosis, imaging studies are required to confirm a rotator cuff tear.
Imaging Studies for Rotator Cuff Injury
The most commonly used imaging methods include X-ray, ultrasound, and magnetic resonance imaging (MRI).
X-ray
X-ray is usually the first imaging test performed in patients with shoulder pain. Because X-rays do not show soft tissues such as the rotator cuff, findings are often normal in cases of rotator cuff injury.
The main purpose of X-ray imaging is to rule out other causes of shoulder pain, such as arthritis. In massive rotator cuff tears, the humeral head may lose stability and migrate upward toward the acromion (cranial migration), which can be clearly seen on X-ray images.


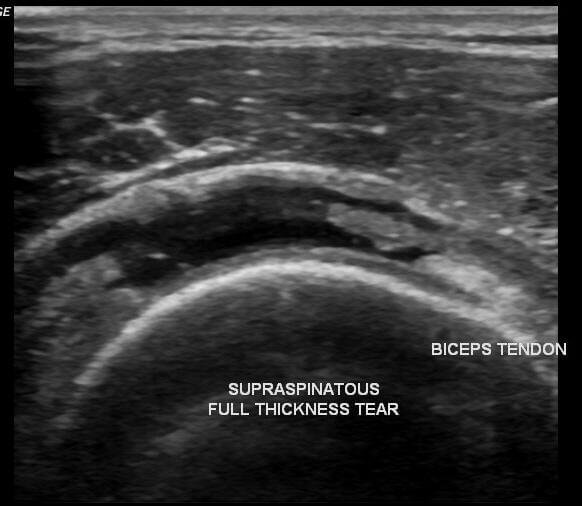
Ultrasound
Ultrasound is a fast, safe, accessible, and cost-effective diagnostic method that allows excellent visualization of soft tissues, including rotator cuff tendons. It is often considered an “extension” of the clinical examination and can be performed during an outpatient visit.
Ultrasound can accurately detect both partial and complete rotator cuff tears, with diagnostic accuracy comparable to MRI. However, in some cases, it may be difficult to distinguish between tendinopathy and a chronic tear.

Magnetic Resonance Imaging (MRI)
MRI is an excellent, non-invasive imaging method for evaluating shoulder soft tissues. It provides detailed information about:
- The size and location of the rotator cuff tear
- Tendon retraction
- Muscle atrophy
- Chronic degenerative changes in the tendon and muscle
- Associated shoulder pathologies
Assessment of muscle atrophy is particularly important when considering surgical repair of a torn rotator cuff. For this reason, MRI is commonly used when planning operative treatment.
Torn Rotator Cuff Treatment
When deciding on the most appropriate torn rotator cuff treatment, several important factors must be considered:
- Patient age
- Level of physical activity
- Overall health status
- Type and size of the tear
- Whether the tear is acute (traumatic) or chronic (degenerative)
For complete tears in patients younger than 40 years of age, surgical repair is generally the recommended treatment, followed by structured rehabilitation. These injuries are typically traumatic and tend to respond well to surgical management.
The primary goal of any torn rotator cuff treatment is to relieve pain and restore shoulder function.
When treatment is initiated early, further symptom progression can often be prevented and recovery may be faster. Chronic tears, especially in older patients, are most commonly treated conservatively. This includes activity modification, pain medication, physical therapy, shoulder exercises, and occasionally corticosteroid injections.
There is no strong evidence that surgical outcomes are significantly better if surgery is performed within six months of the tear compared with delayed surgery.
Conservative Treatment
Conservative management is recommended as the first-line approach for most patients. Approximately 80–85% of patients experience pain relief and improved shoulder function with non-surgical treatment. In many cases, outcomes of conservative care can be comparable to surgery, even in larger tears.
Available treatment options include:
Conservative torn rotator cuff treatment options:
Rest and Activity Modification
Temporary rest from activities — whether sports or occupational — that aggravate symptoms may be necessary. Avoid movements and positions that provoke shoulder pain, especially repetitive overhead activities.
Pain Medication
Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, ketoprofen, naproxen, and diclofenac, are commonly prescribed. These medications reduce both pain and inflammation.
If NSAIDs are not tolerated or cause side effects, a physician may prescribe alternative analgesics, such as tramadol, either alone or in combination with paracetamol.
Physical Therapy and Rotator Cuff Exercises
Physical therapy plays a central role in torn rotator cuff treatment. Carefully designed rotator cuff exercises aim to:
- Strengthen the shoulder muscles
- Improve range of motion
- Correct posture
- Restore muscular balance in the upper limb
Exercises should focus on strengthening the rotator cuff muscles — particularly the supraspinatus and infraspinatus — as well as the trapezius and serratus anterior, which are key stabilizers of the scapula.
Additional physical therapy modalities such as therapeutic ultrasound, heat therapy, TENS, laser therapy, or diathermy may also be used to reduce pain.
Corticosteroid Injection
If rest, medication, and physical therapy do not adequately relieve pain, an injection of a local anesthetic combined with a corticosteroid may be considered. Corticosteroids are powerful anti-inflammatory agents, although they are not effective in all patients.
Whenever possible, corticosteroid injections should be performed under ultrasound guidance to ensure accurate placement. The duration of pain relief varies — it may last weeks, months, years, or in some cases provide long-term relief. Approximately two-thirds of patients experience meaningful pain reduction for at least three months.
It is important to note that conservative treatment may not produce immediate improvement. Meaningful results are generally expected within 6–12 weeks, so treatment should not be discontinued prematurely if early improvement is limited.
Surgical Treatment
Surgical treatment involves reattaching the torn tendon to its insertion on the humerus. Surgery is generally recommended for patients who do not achieve satisfactory improvement after adequate conservative torn rotator cuff treatment.
It may also be advised in cases of:
- Acute traumatic tears in patients younger than 40
- Individuals wishing to continue overhead sports or physically demanding activities
Other circumstances in which surgery should be considered include:
- Symptoms lasting 6–12 months despite conservative treatment
- A large tear (greater than 3 cm)
- Good quality of surrounding tissue (minimal muscle atrophy)
- Significant weakness and functional loss despite non-surgical care
When Is Surgery Not Recommended?
Surgical repair may not be advised in the following situations:
- Patients older than 65 years
- Significant fatty muscle atrophy
- Advanced shoulder arthropathy (inflammatory or secondary to massive rotator cuff tears)
- Individuals who have a tear but do not experience pain or functional limitation
Recovery After Rotator Cuff Surgery
After surgical repair of a torn rotator cuff, it typically takes six to eight weeks for the tendon to biologically heal back to the bone.
Full recovery time depends on the size of the tear:
- Small tears: approximately 4 months
- Large tears: around 6 months
- Massive tears: 6 to 12 months
Most patients can return to many daily activities approximately 12 weeks after surgery. However, participation in high-intensity or overhead sports may be restricted for four to six months.
The ultimate goal of rehabilitation is to restore full range of motion and complete shoulder muscle strength.
Frequently Asked Questions About Rotator Cuff Tear
Does a Rotator Cuff Tear Worsen Over Time?
Research shows that most rotator cuff tears tend to progress over time. More specifically, about half of patients can expect an increase in tear size within a three-year period.
The risk of progression increases with the initial size of the tear. Full-thickness tears are more likely to enlarge compared to partial tears. Tear progression is also more common when the affected shoulder is the dominant arm.
There is limited evidence suggesting that smaller tears may occasionally heal or stabilize; however, the general trend indicates that most tears gradually increase in size.
Can a Torn Rotator Cuff Heal Without Surgery?
In short, no — a torn rotator cuff does not spontaneously reattach to the bone.
However, despite the tendon not biologically healing, many patients can achieve good shoulder function without surgery, regardless of tear size. The primary goal of torn rotator cuff treatment is to reduce pain and improve shoulder function rather than to anatomically close the tear in every case.
What Happens If the Tear Is Not Operated On?
Most degenerative rotator cuff tears are treated conservatively, and outcomes of non-surgical torn rotator cuff treatment are often comparable to surgical results, even in larger tears.
However, in some cases — particularly with larger tears — failure to repair the tendon may lead to:
- Fatty degeneration and atrophy of the rotator cuff muscles
- Development of so-called cuff arthropathy
Cuff arthropathy is a condition that develops after chronic rotator cuff damage and results in degenerative changes of the shoulder joint, including cartilage and bone damage.
Importantly, significant joint destruction is not the rule and occurs only in a smaller proportion of patients.
What Other Conditions Can Mimic a Rotator Cuff Tear?
The main symptom of a rotator cuff tear is shoulder pain, often accompanied by weakness, night pain, clicking sensations, or limited range of motion.
Other common conditions that may present with similar symptoms include:
- Rotator cuff tendinitis or tendinopathy
- Shoulder impingement syndrome
- Shoulder bursitis
- Frozen shoulder (adhesive capsulitis)
- Calcific tendinitis
A proper clinical examination and imaging are essential to distinguish between these conditions and confirm a rotator cuff injury.