

Hip pain is a common complaint that leads many patients to seek medical attention. Greater trochanteric pain syndrome (GTPS) is the most frequent cause of lateral hip pain, especially in individuals aged 40 to 60. The hallmark symptom is pain over the outer aspect of the hip, which often worsens during walking, stair climbing, or lying on the affected side. Pain may radiate down the lateral thigh toward the knee, sometimes leading to misdiagnosis as lumbar radiculopathy or sciatica.
Trochanteric bursitis and gluteal tendinopathy are not considered separate conditions but rather represent specific pathological components within the umbrella diagnosis of GTPS. Evidence indicates that lateral hip pain is more commonly related to gluteal tendon pathology than to isolated inflammation of the trochanteric bursa.
These conditions can develop due to mechanical overload, a sedentary lifestyle, excess body weight, or weakness of the hip abductor muscles. In the sections that follow, we will examine the anatomy, causes, symptoms, and evidence-based management strategies for GTPS, including trochanteric bursitis and gluteal tendinopathy.
What is Greater Trochanteric Pain Syndrome (GTPS)?
Definition:
Greater Trochanteric Pain Syndrome (GTPS) is a painful condition that causes discomfort on the outer side of the hip. It is usually caused by gluteal tendinopathy or trochanteric bursitis, which are considered components of this syndrome rather than separate diseases.
GTPS most commonly occurs in middle-aged women, and the main symptom is lateral hip pain that may radiate down the thigh toward the knee. The pain often worsens with walking, stair climbing, or lying on the affected side.
Hip Anatomy and Key Concepts
To better understand Greater Trochanteric Pain Syndrome (GTPS), it is important to clarify some basic anatomical concepts.
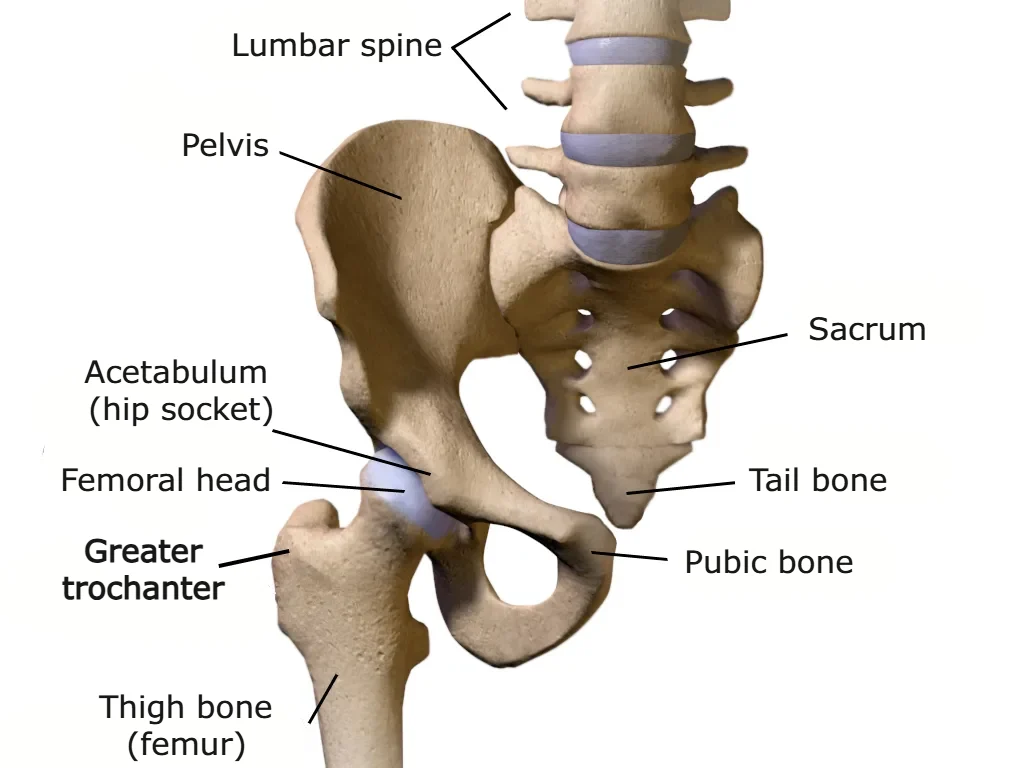
The hip joint is a synovial ball-and-socket joint, where the spherical head of the femur fits into a cup-shaped socket in the pelvic bone called the acetabulum. The joint is surrounded by a capsule and reinforced by strong ligaments that provide stability while still allowing movement in multiple directions. Its primary function is to transmit weight between the upper and lower body.
The greater trochanter is a bony prominence on the femur that serves as the attachment point for tendons of the hip muscles. It can be palpated on the lateral side of the hip. While the hip contains many muscles, the gluteus medius and gluteus minimus are particularly important for GTPS. These muscles attach to the greater trochanter and play a key role in stabilizing the hip, especially during single-leg stance while walking. They prevent the pelvis from tilting to the opposite side when lifting the leg, ensuring proper gait mechanics.
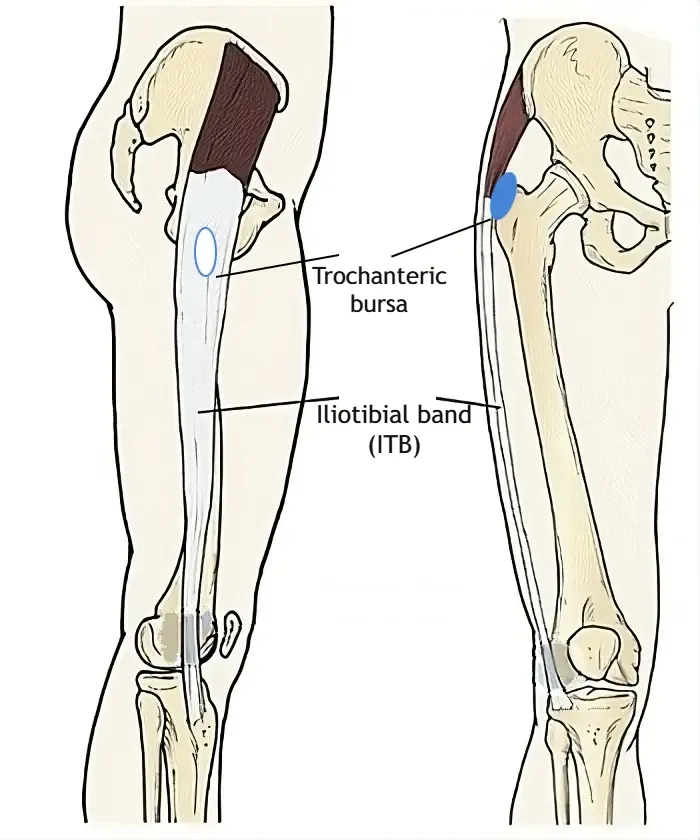
Bursae are small fluid-filled sacs located where tendons, muscles, or skin rub against bone. Their main function is to reduce friction and facilitate smooth movement of these structures. In the hip, several bursae exist, with the trochanteric bursa being the largest and most relevant to GTPS. Trochanteric bursitis refers to inflammation of this bursa.
The iliotibial band (ITB) is a thick, strong band of connective tissue that runs along the outer thigh from the hip to the knee, crossing over the greater trochanter along its path.
Trochanteric Pain Syndrome, Hip Tendinopathy, and Trochanteric Bursitis – What’s the Difference?
The terms Greater Trochanteric Pain Syndrome (GTPS), hip tendinopathy, and greater trochanteric bursitis are often used interchangeably, which can confuse patients and even some clinicians. It is important to clarify the meaning of each term and understand how these conditions are related.
Trochanteric bursitis or greater trochanteric bursitis refers specifically to inflammation of the bursa, a small fluid-filled sac located above the bony prominence of the greater trochanter. Historically, it was thought to be the main cause of lateral hip pain. However, current evidence shows that trochanteric bursitis is present in only about 10% of patients with lateral hip pain. Instead, degenerative changes in the gluteus medius and gluteus minimus tendons, known as gluteal tendinopathy (commonly called hip tendon inflammation), are considered the leading cause of symptoms and dysfunction.
To reduce confusion, the term Greater Trochanteric Pain Syndrome (GTPS) was introduced. GTPS is a modern, umbrella term that describes pain in the lateral hip over the greater trochanter, which worsens with walking, stair climbing, or lying on the affected side. GTPS encompasses several conditions, including:
- Trochanteric bursitis (inflammation of the bursa)
- Gluteal tendinopathy (degeneration or inflammation of the gluteal tendons)
- External snapping hip
This syndrome can significantly interfere with daily activities, particularly walking, standing, or sleeping. It most commonly affects individuals aged 40 to 60 and is much more frequent in women than in men.
Hip Bursitis Symptoms
The main symptom of Greater Trochanteric Pain Syndrome (GTPS) is pain on the outer (lateral) side of the hip, around the greater trochanter. Pain may also be felt in the thigh, and less commonly in the groin or buttocks.
Patients with trochanteric bursitis or gluteal tendinopathy may experience all or only some of the following symptoms:
- Pain type: Can range from dull to sharp or stabbing. Initially, pain is often sharp and localized around the greater trochanter. Over time, it may become more diffuse, dull, and affect a larger area of the hip, thigh, or buttocks.
- Radiating pain: Pain may extend from the hip down the leg toward the knee, sometimes mimicking sciatica.
- Activity-related pain: Pain often increases during activities that load the hip, such as walking, running, climbing stairs, or ascending hills. Symptoms can appear immediately at the start of activity or gradually worsen over time.
- Pain when rising: Pain may be worse when standing up from a chair after prolonged sitting, lifting the leg onto a bed, or getting into a car.
- Night pain: Lying on the affected side during sleep can trigger discomfort, which often affects sleep quality.
- Tenderness: The greater trochanter may be painful to touch or pressure. Many patients report discomfort when pressing or massaging the area.
- Associated weakness: GTPS is often accompanied by weakness in the gluteal muscles and lateral hip stabilizers.
These symptoms can significantly interfere with daily activities, including walking, standing, and sleeping.
How GTPS Develops: Tendon Degeneration and the Role of the Bursa
Greater Trochanteric Pain Syndrome (GTPS) is primarily caused by degeneration of the gluteal tendons attached to the greater trochanter, along with changes in the associated bursae. During activities such as walking, running, or climbing stairs, the iliotibial band (ITB) repeatedly passes—or “snaps”—over the greater trochanter.
This repetitive friction between the ITB and the greater trochanter can cause microtrauma to the tendon insertion. The friction leads to local inflammation, affecting both the bursa (trochanteric bursitis) and the tendons (gluteal tendinopathy). Over time, these processes result in chronic changes in the gluteal tendons, known as gluteal tendinopathy.
As with most chronic tendinopathies, structural changes occur within the tendon itself, including collagen fiber disorganization, increased cellularity, excessive proteoglycan production, and neovascularization (the ingrowth of new blood vessels into the tendon). These changes weaken the tendon structure, making it more vulnerable to further damage. Current evidence suggests that symptoms are more related to myofascial pain than to true tendon inflammation.
Causes of Gluteal Tendinopathy and Trochanteric Bursitis
The causes of Greater Trochanteric Pain Syndrome (GTPS) are multifactorial and involve a combination of external factors and individual patient characteristics. Below are the main factors that contribute to the development of gluteal tendinopathy and trochanteric bursitis.
Common Symptoms of a Swollen Knee
- Swelling: One knee may appear larger due to excess fluid within the joint or bursae.
- Pain: Usually occurs with movement or weight-bearing, while resting often relieves discomfort.
- Stiffness: Bending or straightening the knee can be difficult, especially after periods of rest.
- Muscle Weakness: The quadriceps may lose strength and bulk, affecting walking and joint stability.
- Reduced Range of Motion: The knee may not fully bend or straighten due to pain or swelling.
- Warmth and Redness: More noticeable with inflammatory or infectious causes; skin may be red and warm to the touch.
- Inability to Bear Weight: Large effusions or acute injuries make standing and walking difficult.
- Clicking or Locking: Can occur with meniscus damage or hemarthrosis, limiting normal movement.
Common Causes of GTPS
- Mechanical overload:
Repetitive activities such as prolonged walking or running increase friction between the greater trochanter and the iliotibial band (ITB). This continuous stress can lead to microtrauma and local inflammation. Symptoms often develop after a sudden increase in training intensity, distance, or frequency. - Training and movement errors:
High-intensity training or long-distance running without adequate preparation may place excessive stress on the hip joint. Poor load management and lack of gradual progression increase the risk of GTPS. - Muscle weakness and reduced flexibility:
Weakness of the hip abductor muscles and reduced flexibility of the hip musculature are significant risk factors for developing lateral hip pain. - Sedentary lifestyle and excess body weight:
Prolonged sitting contributes to muscle weakness and reduced hip flexibility. Excess body weight increases mechanical load on the hip joint and tendon insertions, including the greater trochanter. - Prolonged pressure on the lateral hip:
Long periods of sitting or standing in one position, habitual weight-bearing on one leg, or sleeping on the affected side can increase pressure on the lateral hip structures. - Trauma:
Direct injury, such as a fall onto the side of the hip, can trigger the onset of symptoms. - Hormonal factors:
Hormonal changes may play a role, with women in the perimenopausal and postmenopausal periods being at increased risk of developing gluteal tendinopathy. - Associated conditions:
GTPS may be associated with hip osteoarthritis and chronic low back pain, which can alter biomechanics and load distribution. - Spinal and limb alignment issues:
Anatomical variations such as scoliosis or leg length discrepancy can create uneven loading of the hips, placing additional stress on the greater trochanter.
Diagnosis of Greater Trochanteric Pain Syndrome (GTPS)
If Greater Trochanteric Pain Syndrome (GTPS) is suspected, patients should seek evaluation by a physical medicine specialist or musculoskeletal clinician. A thorough medical history, focused clinical examination, and targeted diagnostic testing are essential for establishing an accurate diagnosis and initiating appropriate treatment.
In most cases, the diagnosis of GTPS is based on typical symptoms and clinical findings. The diagnostic process begins with a detailed patient history, including the presence or absence of trauma, the mechanism of symptom onset, pain characteristics, duration of symptoms, and factors that aggravate or relieve pain.
This is followed by a targeted physical examination, during which the clinician assesses gait patterns, hip range of motion, and performs specific provocation tests to reproduce lateral hip pain. These findings help confirm the diagnosis and differentiate GTPS from other causes of hip pain.
It is important to exclude other common conditions that may cause hip pain, such as hip osteoarthritis and femoroacetabular impingement (FAI).
Plain X-rays are not routinely required but may be used to rule out bony pathology, including fractures or advanced degenerative joint changes.
If diagnostic uncertainty remains, musculoskeletal ultrasound can be useful to detect thickening and structural changes of the gluteal tendons and to identify inflammation of the trochanteric bursa. Magnetic resonance imaging (MRI) is rarely necessary and is typically reserved for cases where a gluteal tendon tear is suspected or when symptoms do not respond to appropriate conservative treatment.
How to Tell If Your Hip Pain Is Bursitis
Hip bursitis, most commonly involving the trochanteric bursa, is a frequent cause of pain on the outer side of the hip. However, not all lateral hip pain is caused by bursitis, as conditions such as gluteal tendinopathy and greater trochanteric pain syndrome can produce very similar symptoms. Recognizing key features can help determine whether bursitis is the likely source of pain.
Common signs that suggest hip bursitis include:
- Pain localized over the outer aspect of the hip, often directly over the greater trochanter
- Tenderness to touch over the lateral hip
- Pain that worsens when lying on the affected side
- Discomfort during prolonged walking, stair climbing, or standing
- Pain that may develop gradually or after increased activity, repetitive movements, or prolonged pressure
Features that may suggest another cause rather than bursitis:
- Pain deep in the groin or radiating below the knee
- Significant hip stiffness or reduced range of motion
- Neurological symptoms such as numbness, tingling, or weakness
- Persistent pain despite rest and initial conservative measures
Sciatica vs Gluteal Tendinopathy and GTPS
Diagnosing Greater Trochanteric Pain Syndrome (GTPS) can sometimes be challenging and may therefore be delayed. The symptoms of GTPS can mimic disorders of the lumbar spine, particularly low back pain, sciatica, lumbar spinal stenosis, and lumbar radiculopathy caused by nerve root compression, most commonly involving the L2–L4 nerve roots.
Both GTPS and lumbar spine conditions can cause pain in the hip and leg, which often leads to diagnostic confusion. However, there are important clinical differences. In gluteal tendinopathy and trochanteric bursitis, pain is typically localized to the lateral aspect of the hip and only rarely radiates below the knee. In contrast, sciatica and lumbar radiculopathy more commonly produce pain that radiates down the leg, often extending past the knee and into the lower leg or foot.
A detailed patient history and a targeted physical examination are usually sufficient to distinguish GTPS from lumbar spine–related conditions. Identifying the correct source of pain is essential, as treatment strategies differ significantly between spinal pathology and lateral hip disorders such as GTPS.
| Feature | GTPS / Gluteal Tendinopathy | Sciatica / Lumbar Radiculopathy |
|---|---|---|
| Main pain location | Outer (lateral) side of the hip | Lower back, buttock, and leg |
| Pain radiation | May radiate to thigh, rarely below knee | Commonly radiates below knee to calf or foot |
| Pain with lying on side | Common and often severe | Less common |
| Tenderness over hip | Marked tenderness over greater trochanter | Usually absent |
| Pain with walking or stairs | Frequently worsens | Variable |
| Neurological symptoms | Absent | May include numbness, tingling, weakness |
| Primary cause | Tendon degeneration / bursa involvement | Nerve root compression |
Treatment of Greater Trochanteric Pain Syndrome (GTPS)
Conservative management is the first-line treatment for greater trochanteric pain syndrome, and the majority of patients achieve satisfactory outcomes. The following treatment options are available:
Treatment options for Greater Trochanteric Pain Syndrome:
Some of these methods can be applied at home, while others require evaluation and treatment by a medical specialist. Management should always begin with activity modification and physical therapy, with exercise forming the cornerstone of treatment due to its long-term benefits.
Other modalities—such as shockwave therapy, corticosteroid injections, dry needling, and PRP—are considered only if initial conservative measures fail. Surgical treatment is rarely required and is reserved for refractory cases.
1. Activity Modification and Self-Management
Patient education regarding activity modification and postural control aimed at reducing load and compressive forces on the lateral hip is essential for both prevention and treatment. Patients should adopt strategies to minimize prolonged single-leg loading during daily activities. For example, sitting rather than standing while dressing (e.g., putting on trousers) reduces stress on the gluteal muscles.
When standing for prolonged periods, symmetrical weight-bearing on both legs is recommended instead of leaning on one leg. To limit excessive compression over the lateral hip and prevent symptom exacerbation, sitting with crossed legs should be avoided. When sleeping in a side-lying position—particularly in women with wider pelvises—placing a pillow between the knees is advised.
If symptoms are caused by excessive loading during sports or training, training intensity should be reduced. Any technical errors that increase compression and load on the lateral hip should be identified and corrected.
2. Physical Therapy and Gluteal Tendinopathy Exercises
Physical therapy combined with activity modification has proven to be the most effective treatment for GTPS. When designing an individualized rehabilitation program, key contributing factors should be considered, particularly:
- Weakness of the gluteal muscles (gluteus medius and gluteus minimus)
- Increased tightness or thickening of the iliotibial band
These factors increase compressive forces on the trochanteric bursa and gluteal tendons at the greater trochanter.
The fundamental principles of exercise therapy in gluteal tendinopathy focuses on strengthening the hip abductors, especially the gluteus medius and minimus.
Exercises should be performed daily. Patients are advised to complete 3–4 different exercises per day, with each exercise performed in 2–3 sets of 10–12 repetitions. The exercise program should be followed consistently for 8–12 weeks.
Progressive loading is crucial for improving muscle strength and endurance. During the initial days of exercise, a temporary increase in symptoms may occur; however, this should not persist beyond the third week. Pain reduction may be noticed early in the program. With adherence, the benefits of exercise can persist for several months to up to one year after completion.
An individualized exercise approach allows adaptation of the program to the patient’s specific needs and functional capacity. Education on proper exercise technique and understanding its role in rehabilitation are critical for recovery and long-term symptom control.
3. Extracorporeal Shockwave Therapy (ESWT)

Shockwave therapy is a non-invasive medical treatment that uses acoustic waves to stimulate tissue healing and reduce pain in musculoskeletal conditions. In greater trochanteric pain syndrome with gluteal tendinopathy , shockwaves are applied to the painful area over the greater trochanter.
Treatment is typically performed once weekly for a total of three to five sessions. Clinical improvement is usually observed after the second or third session and may last longer than six months. Shockwave therapy is considered safe, although pain may be experienced during and shortly after treatment.
4. Corticosteroid Injections for Trochanteric Bursitis
Corticosteroid injections into the trochanteric region are commonly used to treat hip bursitis and gluteal tendinopathy. Pain relief usually occurs within 3–5 days after injection. The average duration of effect is 3–5 months, meaning corticosteroids do not provide long-term benefit compared to exercise therapy.
Corticosteroid injections should be limited to a maximum of three times per year. Repeated steroid use may lead to further tendon degeneration and increase the risk of tendon rupture. Additionally, studies have shown that corticosteroids negatively affect tendon healing and slow tissue repair.
5. Dry Needling Therapy
Dry needling is a therapeutic technique used to treat pain and movement dysfunction by inserting a thin, sterile needle—most commonly an acupuncture needle—through the skin to stimulate specific tissues, including trigger points, connective tissue, and muscles.
In the treatment of gluteal tendinopathy and GTPS, dry needling targets specific points around the greater trochanter as well as muscles such as the gluteus medius and minimus. This technique may reduce muscle tension, improve circulation, and modulate neuromuscular activity, leading to pain relief and improved function.
Typically, three treatment sessions are performed at intervals of 7–10 days. Studies have demonstrated effectiveness comparable to local corticosteroid injections, but without significant adverse effects.
6. Platelet-Rich Plasma (PRP) Therapy – A Novel Treatment Option
Platelet-rich plasma (PRP) therapy is a newer treatment option for greater trochanteric pain syndrome (GTPS). It involves injecting a concentrated solution of the patient’s own platelets into the affected tendon, bursa, or joint. Growth factors released from PRP have the potential to stimulate natural healing processes by promoting tissue repair, reducing inflammation, and improving overall function.
Although research is ongoing, some studies have shown outcomes comparable to corticosteroid injections, with sustained benefits lasting up to two years. PRP is derived exclusively from the patient’s own tissue and is associated with minimal known side effects.
7. Surgical Treatment
Surgical intervention for trochanteric pain syndrome is considered only in patients with persistent symptoms lasting at least 6–12 months despite comprehensive conservative treatment. Prior to surgery, magnetic resonance imaging (MRI) is recommended to identify the specific pain source.
Depending on the underlying pathology, surgical options may include:
- Open or endoscopic bursectomy (removal of the bursa), with or without release of the iliotibial band
- Procedures similar to those used for external snapping hip syndrome
- Open or endoscopic repair of partial or complete gluteal tendon tears
- Tendon lengthening using grafts or muscle transfer procedures in cases of significant tendon retraction or severe muscle atrophy
Greater Trochanteric Bursitis, Gluteal Tendinopathy and Greater Trochanteric Pain Syndrome – 10 Key Facts
- Greater trochanteric pain syndrome (GTPS) is a common cause of lateral hip pain and occurs more frequently in women, particularly between the fourth and sixth decades of life.
- GTPS is an umbrella term that includes several related conditions, such as external snapping hip, trochanteric bursitis, and tendinopathy of the gluteus medius and minimus.
- The primary symptom is pain on the outer side of the hip, which typically worsens during activities such as walking, climbing stairs, standing on one leg, or lying on the affected side.
- Although GTPS was historically attributed mainly to trochanteric bursitis, current evidence highlights gluteal tendinopathy as a major source of pain and functional impairment.
- Because symptoms may overlap with other hip and lumbar spine disorders, establishing an accurate diagnosis can sometimes be delayed.
- Conservative treatment—including patient education, activity modification, physical therapy, analgesic medication (NSAIDs), and corticosteroid injections—results in satisfactory outcomes in more than 90% of patients.
- Physical therapy is the cornerstone of treatment, with a primary focus on strengthening the hip abductors and other muscles of the pelvic girdle.
- Education on activity modification and posture is essential to reduce mechanical load and compressive forces on the lateral aspect of the hip.
- It is important to note that clinical improvement is often gradual, typically occurring over 2–3 months; in some patients, symptoms may persist for several months or even years.
- Surgical intervention is rarely required and is reserved for refractory cases that fail to respond to comprehensive conservative management.
Pumarejo Gomez L, Li DD, Childress JM. Greater Trochanteric Pain Syndrome (Greater Trochanteric Bursitis) [Updated 2024 Feb 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557433/
Speers CJ, Bhogal GS. Greater trochanteric pain syndrome: a review of diagnosis and management in general practice. Br J Gen Pract. 2017 Oct;67(663):479-480. doi: 10.3399/bjgp17X693041. PMID: 28963433; PMCID: PMC5604828.
Kjeldsen T, Hvidt KJ, Bohn MB, Mygind-Klavsen B, Lind M, Semciw AI, Mechlenburg I. Exercise compared to a control condition or other conservative treatment options in patients with Greater Trochanteric Pain Syndrome: a systematic review and meta-analysis of randomized controlled trials. Physiotherapy. 2024 Jun;123:69-80. doi: 10.1016/j.physio.2024.01.001. Epub 2024 Jan 5. PMID: 38295551.
Wang Y, Wang K, Qin Y, Wang S, Tan B, Jia L, Jia G, Niu L. The effect of corticosteroid injection in the treatment of greater trochanter pain syndrome: a systematic review and meta-analysis of randomized controlled trials. J Orthop Surg Res. 2022 May 21;17(1):283. doi: 10.1186/s13018-022-03175-5. PMID: 35598025; PMCID: PMC9123821.
Nissen MJ, Brulhart L, Faundez A, Finckh A, Courvoisier DS, Genevay S. Glucocorticoid injections for greater trochanteric pain syndrome: a randomised double-blind placebo-controlled (GLUTEAL) trial. Clin Rheumatol. 2019 Mar;38(3):647-655. doi: 10.1007/s10067-018-4309-6. Epub 2018 Sep 28. PMID: 30267357.
Migliorini F, Kader N, Eschweiler J, Tingart M, Maffulli N. Platelet-rich plasma versus steroids injections for greater trochanter pain syndrome: a systematic review and meta-analysis. British Medical Bulletin, Volume 139, Issue 1, September 2021, Pages 86–99. doi: 10.1093/bmb/ldab018
Notarnicola A, Ladisa I, Lanzilotta P, Bizzoca D, Covelli I, Bianchi FP, Maccagnano G, Farì G, Moretti B. Shock Waves and Therapeutic Exercise in Greater Trochanteric Pain Syndrome: A Prospective Randomized Clinical Trial with Cross-Over. J Pers Med. 2023 Jun 10;13(6):976. doi: 10.3390/jpm13060976. PMID: 37373965; PMCID: PMC10301141.
Rompe JD, Segal NA, Cacchio A, Furia JP, Morral A, Maffulli N. Home training, local corticosteroid injection, or radial shock wave therapy for greater trochanter pain syndrome. Am J Sports Med. 2009 Oct;37(10):1981-90. doi: 10.1177/0363546509334374. Epub 2009 May 13. PMID: 19439758.












