
A supraspinatus tendon tear is a common type of rotator cuff injury affecting the tendon of the supraspinatus muscle. This condition can cause pain, weakness, and difficulty performing everyday activities such as lifting the arm or reaching overhead.
A supraspinatus tear can occur due to acute trauma, like a fall or sports injury, or from gradual degenerative changes in the tendon over time. Early recognition and proper diagnosis are essential to prevent further damage and restore shoulder function.
In this article, we will explore the causes, symptoms, diagnostic methods, and treatment options for supraspinatus tears, helping patients and healthcare providers understand this common shoulder injury.
Rotator Cuff Anatomy
The rotator cuff is a group of four muscles and their tendons that surround the shoulder joint and provide both movement and stability. These muscles originate from the scapula (shoulder blade) and attach to the head of the humerus, forming a functional “cuff” around the joint.
The rotator cuff consists of:
- Supraspinatus
- Infraspinatus
- Subscapularis
- Teres minor
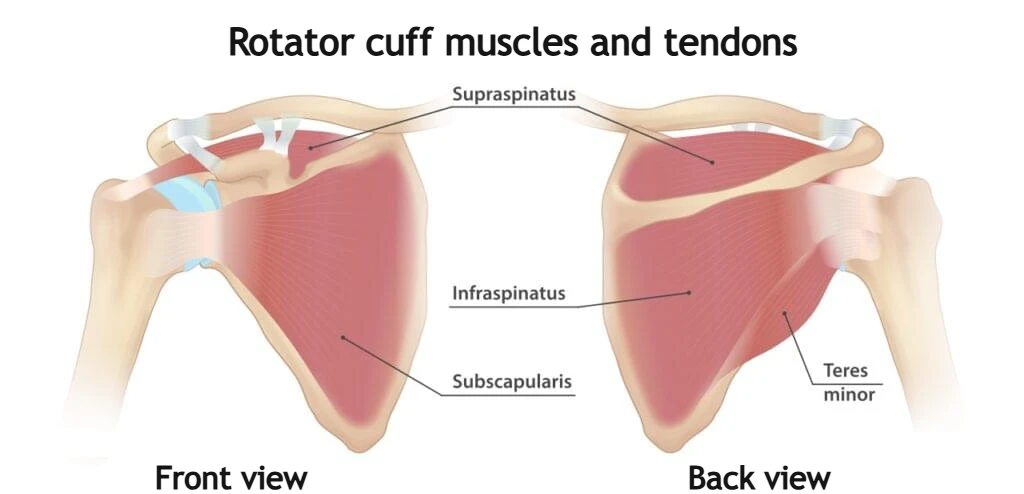
Together, these muscles stabilize the humeral head within the glenoid cavity during shoulder movement. While the shoulder is the most mobile joint in the human body, this mobility comes at the expense of stability. The rotator cuff plays a crucial role in keeping the humeral head centered, particularly during arm elevation and rotation.
In addition to enabling motion, the rotator cuff prevents excessive upward migration of the humeral head toward the acromion. When this stabilizing function is compromised, mechanical irritation, tendon overload, and eventually rotator cuff injury may occur.
Supraspinatus Muscle and Tendon
The supraspinatus muscle is one of the most important components of the rotator cuff and the tendon most commonly involved in a supraspinatus tear. It originates from the supraspinous fossa of the scapula and passes beneath the acromion before inserting onto the greater tuberosity of the humerus.
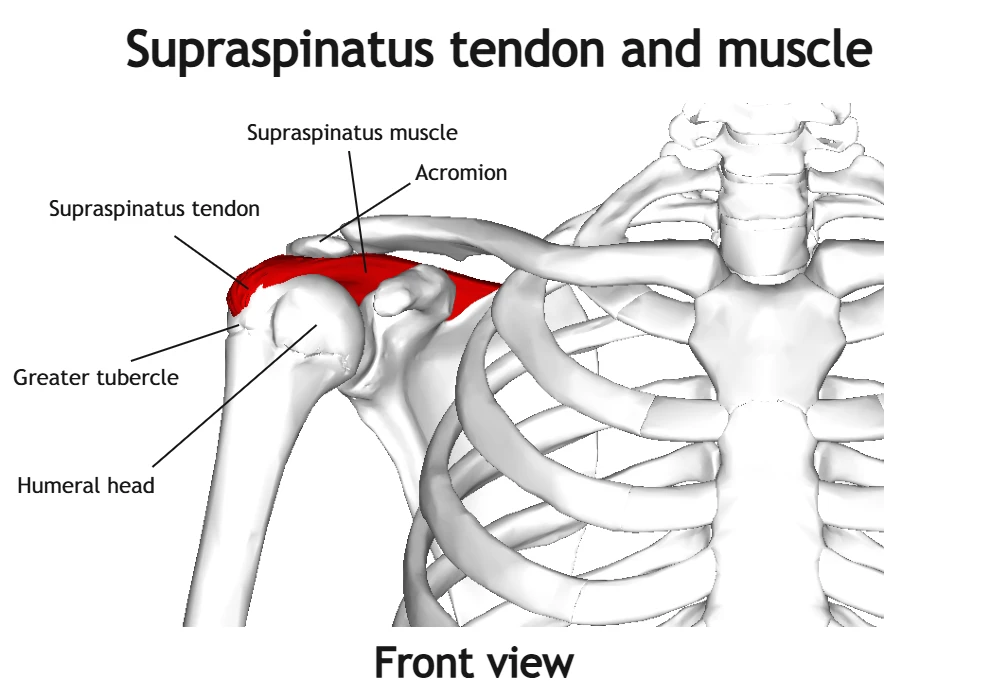
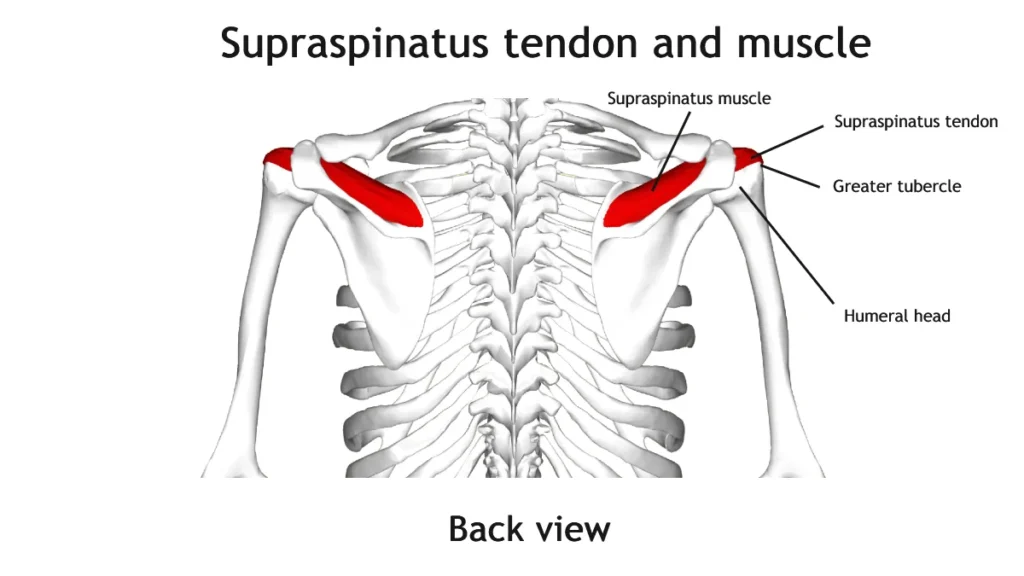
The primary function of the supraspinatus muscle is to initiate arm abduction (lifting the arm away from the body) during the first 15 degrees of movement. It also contributes significantly to shoulder joint stabilization by compressing the humeral head into the glenoid during motion.
The supraspinatus tendon has a region of relatively reduced blood supply known as the “critical zone,” located near its insertion on the humerus. This area is particularly vulnerable to degeneration and tearing. Over time, repetitive overhead activity, mechanical impingement under the acromion, and age-related tendon degeneration can weaken the tendon structure, increasing the risk of a supraspinatus tear.
Because of its anatomical position and biomechanical role, the supraspinatus tendon is involved in approximately 90% of rotator cuff tears, making it the most frequently injured shoulder tendon.
What Is a Supraspinatus Tear?
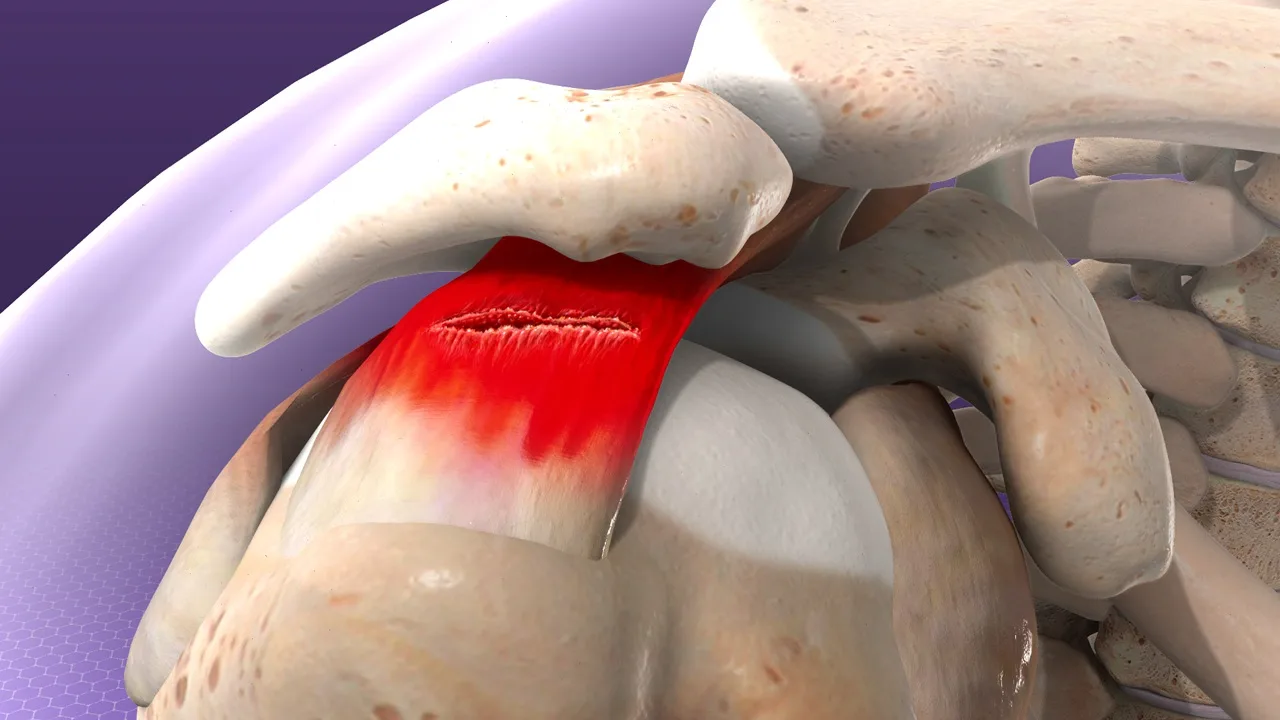
A supraspinatus tear is an injury in which the tendon of the supraspinatus muscle becomes partially or completely torn. Because the supraspinatus tendon is one of the key components of the rotator cuff, this condition is considered the most common type of rotator cuff injury.
A supraspinatus tendon tear can vary in severity, ranging from small partial tears of the tendon fibers to complete ruptures in which the tendon detaches from its attachment on the humerus. Such injuries can lead to shoulder pain, weakness, and difficulty lifting the arm or performing overhead activities.
Causes of Supraspinatus Tear
A supraspinatus tendon tear can develop gradually over time due to degenerative changes in the tendon or occur suddenly as a result of an acute injury. In clinical practice, most supraspinatus tears are related to chronic degeneration, while traumatic tears are less common and usually occur after a specific injury.
Degenerative Supraspinatus Tear
Degenerative changes are the most common cause of rotator cuff tear, particularly in middle-aged and older adults. Over time, the tendon undergoes gradual wear due to repetitive shoulder movements, reduced blood supply, and mechanical stress beneath the acromion.
Several factors contribute to degenerative tendon damage:
- Age-related tendon degeneration
- Repetitive overhead activities (sports or occupational movements)
- Subacromial impingement, where the tendon is compressed between the humeral head and the acromion
- Reduced blood supply to the critical zone of the supraspinatus tendon
- Chronic microtrauma from long-term mechanical stress
These processes can progressively weaken the tendon fibers, eventually leading to a supraspinatus tendon tear, which may initially present as a partial tear and later progress to a full thickness tear of the supraspinatus tendon.
Acute Supraspinatus Tear
An acute rotator cuff injury with supraspinatus tear occurs suddenly following a traumatic event that places excessive force on the shoulder. These injuries are more common in younger individuals or physically active patients.
Common mechanisms include:
- Fall onto an outstretched arm
- Sudden lifting of a heavy object
- Direct trauma to the shoulder
- Shoulder dislocation
- Sports injuries involving rapid arm movement
Acute trauma can cause an immediate full thickness tear of the supraspinatus tendon, particularly if the tendon has already been weakened by underlying degeneration.
In many patients, a combination of degenerative changes and acute trauma ultimately leads to a clinically significant supraspinatus tendon tear.
Types of Supraspinatus Tears
A supraspinatus tendon tear can be classified according to the extent of tendon damage. In many patients, a degenerative tendon tear begins as a small area of tendon degeneration that gradually progresses over time. Depending on how much of the tendon is affected, supraspinatus tears are generally divided into partial-thickness tears and full-thickness tears.
Partial-Thickness Supraspinatus Tear
In a partial supraspinatus tendon tear, the damage affects only a portion of the tendon and does not extend through its entire thickness. The tendon remains attached to the humerus, but its structure becomes weakened and thinner.
Based on the location of the injury within the tendon, partial supraspinatus tears are further classified into:
- Intrasubstance tear – the rupture occurs within the substance of the tendon fibers without reaching the surface of the tendon.
- Articular-sided tear – the tear affects the lower surface of the tendon facing the shoulder joint and the humeral head.
- Bursal-sided tear – the damage occurs on the upper surface of the tendon, adjacent to the subacromial bursa.
A partial supraspinatus tear may remain stable for some time, but in many cases the tear gradually enlarges and can eventually progress to a full thickness tear of the supraspinatus tendon.
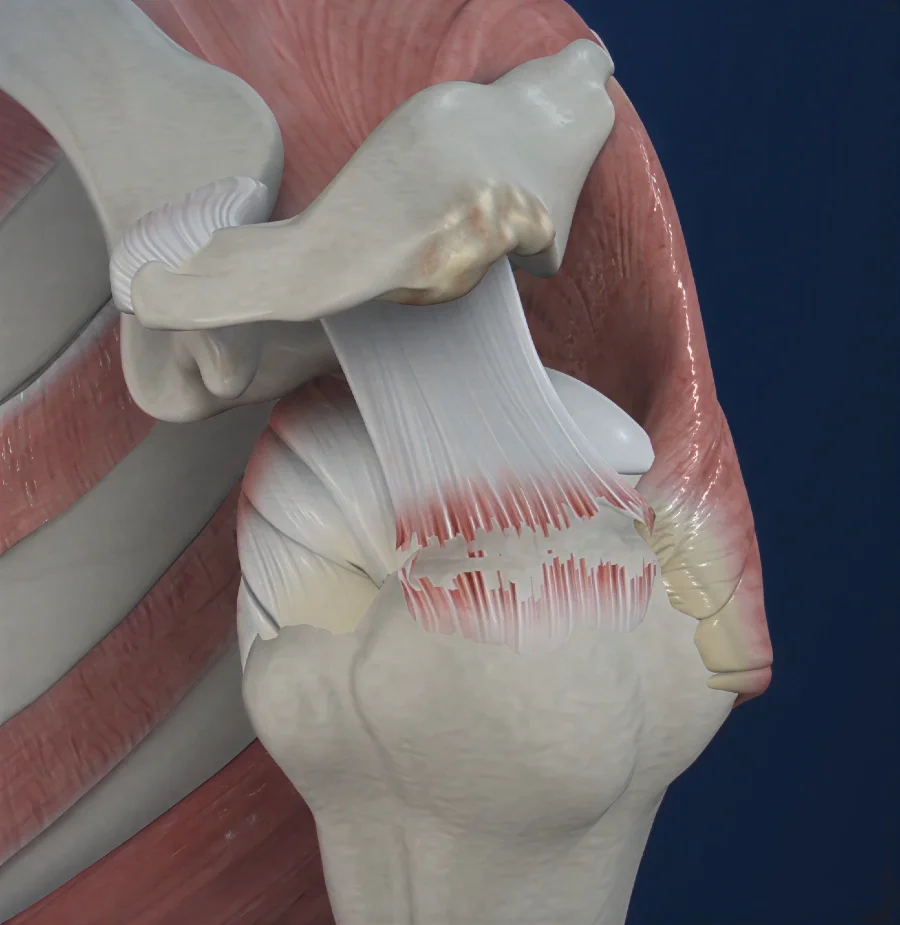
Full-Thickness Supraspinatus Tear
A full thickness tear of the supraspinatus tendon occurs when the rupture extends through the entire thickness of the tendon, creating a communication between the shoulder joint and the subacromial space.
These injuries are considered an advanced form of supraspinatus tendon tear and may vary in severity. They are often divided into:
- Incomplete full-thickness tear, where only a small part of the tendon is detached from the bone.
- Complete full-thickness tear, in which the tendon is fully detached from its insertion on the humerus.
In more advanced cases, the torn tendon may retract away from the bone. Long-standing full thickness tears of the supraspinatus tendon can also lead to fatty degeneration and atrophy of the supraspinatus muscle.
Because the supraspinatus tendon is particularly vulnerable to degeneration and mechanical impingement beneath the acromion, supraspinatus tendon tear is the most common rotator cuff tendon injury.
Symptoms of Supraspinatus Tear
The symptoms of a supraspinatus tendon tear can vary depending on the size of the tear and whether the injury developed gradually or occurred suddenly. Some patients experience mild discomfort for a long period, while others develop significant pain and weakness in the shoulder.
One of the most common symptoms is pain on the outer side of the shoulder, which may radiate down the upper arm. The pain is often worse during activities that involve lifting the arm, especially overhead movements. Many patients also report increased discomfort at night, particularly when lying on the affected shoulder.
Another important symptom of a supraspinatus tendon tear is weakness when lifting the arm away from the body (shoulder abduction). This weakness becomes more noticeable in cases of a full thickness tear of the supraspinatus tendon, where the tendon is no longer able to effectively transmit muscle force to the bone.
Other common symptoms include:
- Pain when lifting the arm or reaching overhead
- Difficulty performing daily activities such as dressing or combing hair
- Shoulder stiffness and reduced range of motion
- A feeling of weakness or loss of strength in the shoulder
- Clicking or catching sensations during shoulder movement
Because these symptoms can overlap with other shoulder conditions, proper clinical evaluation and imaging are necessary to confirm the presence of a supraspinatus tendon tear.
Diagnosis of Rotator Cuff Tear
The diagnosis of a supraspinatus tendon tear is based on a combination of clinical examination and imaging studies. Patients typically present with shoulder pain, weakness, and difficulty performing overhead movements. Pain is often located on the outer side of the shoulder and may worsen when lifting the arm or lying on the affected side.
During the physical examination, the physician evaluates shoulder mobility, strength, and specific clinical tests that assess the function of the supraspinatus muscle. Weakness during arm abduction and pain during certain shoulder movements may suggest a supraspinatus tendon tear or even a full thickness tear of the supraspinatus tendon.
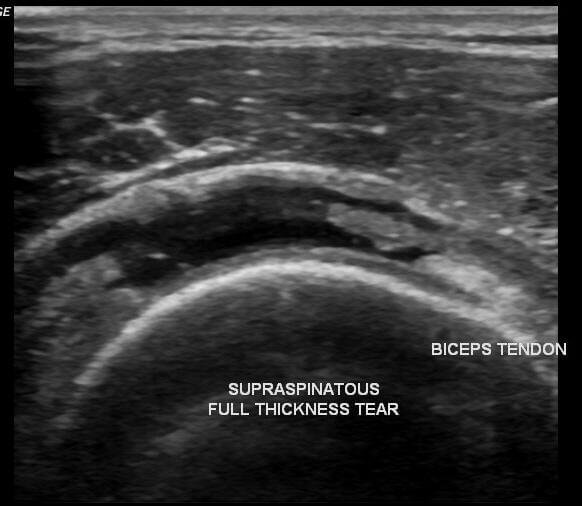
Imaging plays an essential role in confirming the diagnosis and determining the extent of tendon damage:
- Ultrasound is commonly used as an initial imaging method because it allows dynamic assessment of the rotator cuff tendons and can reliably detect partial and full-thickness tears.
- Magnetic resonance imaging (MRI) provides detailed visualization of the rotator cuff, helping evaluate the size of the tear, tendon retraction, and possible muscle degeneration.
- X-ray does not directly show the tendon but may reveal indirect signs, such as upward migration of the humeral head in cases of a large supraspinatus tendon tear.

Accurate diagnosis is important because the treatment approach often depends on the size of the tear and whether the injury represents a partial tear or a full thickness tear of the supraspinatus tendon.
Supraspinatus Tendon Tear Treatment
Supraspinatus tendon tear treatment depends on several factors, including the size of the tear, symptom severity, patient age, and activity level. Treatment can be either conservative (non-surgical) or surgical, and the choice is usually based on the extent of tendon damage and the patient’s functional limitations.
Conservative Treatment
In many cases, especially with partial tears or smaller injuries, supraspinatus tendon tear treatment begins with non-surgical methods. The main goal is to reduce pain, restore shoulder mobility, and strengthen the surrounding muscles that support the rotator cuff.
Conservative treatment options typically include:
- Activity modification, avoiding movements that worsen shoulder pain
- Physical therapy, focused on strengthening the rotator cuff and scapular stabilizing muscles
- Nonsteroidal anti-inflammatory medications (NSAIDs) to reduce pain and inflammation
- Corticosteroid injections into the subacromial space in selected cases
Many patients experience significant improvement with these approaches, even when a structural supraspinatus tendon tear remains present.
Surgical Treatment
Surgical supraspinatus tendon tear treatment may be recommended when symptoms persist despite adequate conservative therapy or when imaging shows a large full thickness tear of the supraspinatus tendon. The goal of surgery is to reattach the torn tendon to the humerus and restore normal shoulder mechanics.
Today, most repairs are performed using arthroscopic techniques, which are minimally invasive and allow faster recovery compared with traditional open surgery.
Surgery is more often considered in the following situations:
- Large or progressive tears
- Acute traumatic tears in active individuals
- Persistent pain and weakness despite rehabilitation
- Confirmed full thickness tear of the supraspinatus tendon
After surgical repair, rehabilitation plays a crucial role in recovery. A structured physiotherapy program gradually restores shoulder mobility, strength, and function following supraspinatus tendon tear treatment.
To learn more about rotator cuff tear treatment, including conservative therapy and surgical repair, visit the following guide:
https://jointhealthguide.com/rotator-cuff-tear/#Torn_Rotator_Cuff_Treatment
Does a Full-Thickness Tear of the Supraspinatus Tendon Need Surgery?
Not every full-thickness tear of the supraspinatus tendon requires surgical repair. In many cases, conservative management is the first-line approach and can provide excellent outcomes. Studies show that approximately 80–85% of patients experience significant pain relief and improved shoulder function with non-surgical treatment, even in some larger tears. Conservative care typically includes activity modification, physical therapy, anti-inflammatory medications, and sometimes corticosteroid injections.
Surgery is usually considered only when non-surgical treatment fails to provide adequate improvement. Indications for surgical repair of a full-thickness tear of the supraspinatus tendon include:
- Acute traumatic tears in younger patients, particularly under 40 years of age
- Persistent pain or functional limitation despite 6–12 months of conservative management
- Large tears greater than 3 cm
- Good quality of surrounding tendon tissue with minimal muscle atrophy
- Patients who wish to return to overhead sports or physically demanding activities
- Significant weakness or loss of shoulder function
Conversely, surgery may not be recommended in certain situations:
- Patients older than 65 years
- Significant fatty degeneration or muscle atrophy
- Advanced shoulder arthropathy or chronic degenerative joint changes
- Individuals with a tear but no pain or functional limitation
Ultimately, the decision for surgical repair depends on the patient’s symptoms, functional needs, tear size, and overall shoulder health. Many patients with a full-thickness tear of the supraspinatus tendon can achieve good shoulder function through conservative treatment alone.
FAQ – Supraspinatus Tear Recovery & Related Questions
1. How long does it take to recover from supraspinatus tendon surgery?
After surgical repair, tendon healing typically takes 6–8 weeks. Full recovery depends on tear size:
- Small tears: ~4 months
- Large tears: ~6 months
- Massive tears: 6–12 months
Most patients return to daily activities around 12 weeks, while high-intensity or overhead sports may require 4–6 months.
2. Do supraspinatus tears worsen over time?
Yes. Many tears tend to progress, especially full-thickness tears or when the dominant shoulder is affected. About half of patients may see tear enlargement within three years.
3. Can a supraspinatus tear heal without surgery?
No, the tendon does not spontaneously reattach. However, many patients achieve good shoulder function through conservative care (physical therapy, activity modification, medications), even with full-thickness tears.
4. What happens if a supraspinatus tear is not operated on?
Untreated tears can lead to:
- Fatty degeneration and atrophy of the supraspinatus muscle
- Cuff arthropathy (degenerative changes in the shoulder joint)
Significant joint destruction is rare and occurs only in a smaller proportion of patients.
5. What conditions can mimic a supraspinatus tear?
Symptoms of pain, weakness, or limited motion can also appear in:
- Rotator cuff tendinitis or tendinopathy
- Shoulder impingement syndrome
- Shoulder bursitis
- Frozen shoulder (adhesive capsulitis)
- Calcific tendinitis
Proper clinical evaluation and imaging are essential to confirm a supraspinatus tendon tear.












