

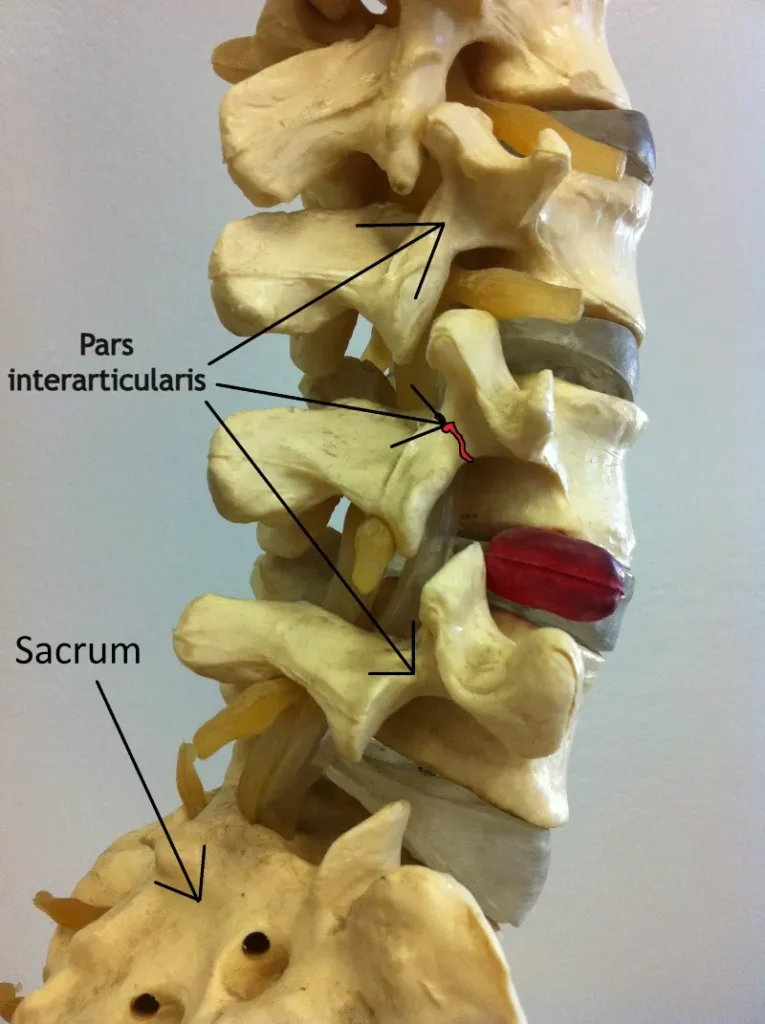
Spondylolysis is a stress fracture or pars defect of the vertebra known as the pars interarticularis. It most commonly occurs in the lower lumbar spine (L5) of children and adolescents who are active in sports. If left untreated, it may lead to vertebral slippage, a condition called spondylolisthesis.
- Spondylolysis is a stress fracture of the pars interarticularis of a vertebra.
- It most commonly occurs in children and adolescents who participate in sports.
- The most common symptom is lower back pain that worsens with spinal extension.
- Diagnosis is confirmed using imaging methods such as MRI or CT scans.
- In most cases, treatment is conservative.
Introduction
Spondylolysis is a relatively common cause of lower back pain in children and adolescents, particularly among young athletes exposed to repetitive spinal stress. Although it often goes unnoticed because it can be asymptomatic, early detection is crucial to prevent complications, such as spondylolisthesis – a condition in which the affected vertebra slips forward relative to the adjacent vertebra.
Most cases occur in the lumbar spine, especially at the fourth and fifth lumbar vertebrae (L4 and L5). High-risk sports include gymnastics, rowing, tennis, soccer, and athletics. The prevalence of spondylolysis is roughly equal in boys and girls, while it is less common in adults and usually does not cause significant pain.
Timely recognition and appropriate treatment, most often conservative, allow a successful return to daily activities and sports and significantly reduce the risk of developing spondylolisthesis and chronic lower back pain.
Spondylolysis Definition?
Spondylolysis is a condition in which a crack or bone defect develops in a part of the vertebra called the pars interarticularis. The term comes from the Greek words spondylos (vertebra) and lysis (break or separation). The pars interarticularis is a narrow segment of bone connecting the upper and lower articular processes of a vertebra, contributing to the stability of the posterior part of the spine. A defect in this area can compromise the stability of the posterior spinal segment and, in some cases, lead to spondylolisthesis, where the vertebra slips forward, backward, or sideways relative to the adjacent vertebra.
Spondylolysis most commonly occurs in the lower lumbar spine, particularly at the fourth and fifth lumbar vertebrae (L4 and L5). It is believed to develop gradually due to repetitive stress and microtrauma, especially during activities that involve frequent backward bending and trunk rotation. This is why spondylolysis is relatively common in children and adolescents who are actively involved in sports.
In many cases, spondylolysis is asymptomatic and is discovered incidentally during imaging studies. However, some patients may experience lower back pain, particularly during sports activities or movements that put stress on the spine.
Did You Know?
Spondylolysis is one of the most common causes of chronic lower back pain in young athletes. It develops due to repetitive stress and microfractures in a part of the vertebra called the pars interarticularis.
If the bone defect is not detected and treated in time, it can sometimes lead to vertebral slippage – a condition known as spondylolisthesis.
Who Is Most Affected by Spondylolysis?
Spondylolysis most commonly occurs in children and adolescents, especially before the age of 18, with young athletes being particularly at risk. Studies show that spondylolysis is the leading cause of lower back pain in adolescent athletes, accounting for nearly 47% of cases in this population. However, spondylolysis is not exclusive to young athletes. It is also present in 6–12% of adults, usually without causing significant lower back pain.
The risk is particularly high in sports that involve frequent spinal extension and rotation, such as gymnastics, rowing, swimming, soccer, tennis, and athletics. Repetitive stress on the lumbar spine during training and competition increases the likelihood of microtraumas and the development of spondylolysis.
Although spondylolysis can also occur in non-athletic children, it is much less common. Historically, it was believed to occur two to three times more often in males, but with the rise of female participation in competitive sports—especially gymnastics—the prevalence in girls has now increased fourfold.
Key Facts About Spondylolysis
- Most commonly affects children and adolescents – especially those actively involved in sports.
- Frequent cause of lower back pain in young athletes – responsible for nearly half of lumbar pain cases in adolescent athletes.
- Higher risk in certain sports – activities involving repeated backward bending and trunk rotation, such as gymnastics, rowing, tennis, soccer, and athletics, increase spinal stress.
- Similar prevalence in boys and girls – spondylolysis occurs roughly equally in both sexes.
Why Spondylolysis Occurs (Mechanism)
The exact cause of spondylolysis is not fully understood, but it is generally considered a result of repeated mechanical stress on the spine, sometimes combined with a genetic predisposition. In most cases, it develops as a stress fracture that forms gradually over time.
About 95% of spondylolysis cases occur at the level of the fifth lumbar vertebra (L5). Repeated extension, rotation, and bending movements create shear forces on the pars interarticularis. During these movements, the inferior articular process of L4 and the superior articular process of S1 place additional load on the L5 pars interarticularis. Over time, this repeated stress can cause microfractures, which may eventually develop into a full bony defect.
Other risk factors can contribute to spondylolysis, including anatomical or developmental changes in the spine and genetic susceptibility. For example, a higher incidence is seen in individuals with spinal deformities such as Scheuermann’s disease or spina bifida occulta. These factors can alter the distribution of stress in the spine, increasing the load on the pars interarticularis.
Main factors contributing to spondylolysis:
- Repeated spinal extension and rotation
- Intensive sports training during growth periods
- Recurrent microtraumas to the lumbar spine
- Genetic predisposition
- Developmental or anatomical spinal changes (e.g., Scheuermann’s disease, spina bifida occulta)
Symptoms of Spondylolysis
Most cases of spondylolysis are asymptomatic – it is estimated that around 87% of patients experience no symptoms, especially adults. However, spondylolysis remains the most common cause of lower back pain in children and adolescents, particularly in young athletes. Symptoms often develop gradually, although some patients may recall an episode of acute trauma after which the first signs appeared.
When symptoms do occur, they are usually mild and related to activity or stress:
- Lower back pain that appears during activity and eases with rest.
- Pain may initially occur only during intense physical activities but can gradually worsen and interfere with daily life.
- Pain often increases with excessive extension or rotation of the spine, as well as lifting from a bent position, especially against resistance.
- Tenderness in the lumbosacral region and buttocks, sometimes accompanied by reduced spinal mobility.
- Muscle spasms in the paravertebral muscles and tight hamstrings.
Neurological symptoms are rare, but progression of spondylolysis to spondylolisthesis can lead to nerve root compression, radiculopathy, neurogenic symptoms such as claudication, bowel or bladder dysfunction, and very rarely cauda equina syndrome.
Pain while sitting, worsening pain at rest, or persistent nighttime pain is not typical of spondylolysis and may indicate sacroiliac joint injury, sacroiliitis, or, less commonly, more serious conditions such as tumors.
Diagnosis of Spondylolysis
The diagnosis of spondylolysis begins with a detailed medical history, including questions about previous sports activities and possible congenital spinal abnormalities, such as spina bifida.
A clinical examination includes visual assessment of the spine and posture, evaluation of lumbar lordosis, kyphosis, and gait, palpation of the paravertebral muscles, and assessment of local tenderness and pain. In spondylolysis, pain is often reproduced by spinal extension.
Clinical tests can be helpful but do not confirm the diagnosis. The most well-known is the Stork test, where the patient stands on one leg while the other leg is pulled backward, inducing lumbar hyperextension and pain in the lumbosacral region. Progression to spondylolisthesis may be detected by the presence of a “step-off” deformity on palpation of the spine.
Imaging studies are required to confirm a definitive diagnosis of spondylolysis.
- X-ray (lumbosacral radiograph) is usually the first imaging method and can reveal a pars interarticularis defect, especially if a complete fracture is present. However, X-rays are not sensitive enough for early cases or stress fractures, where the fracture line may not yet be clearly visible.
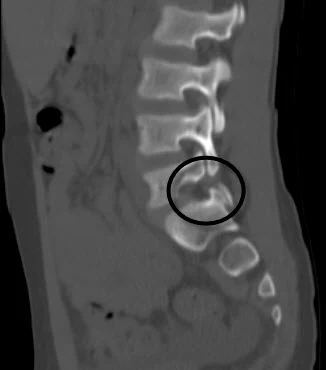
- CT scan (computed tomography) provides a more detailed view of bony structures and is considered the gold standard for visualizing pars interarticularis fractures. CT also has limitations: it is less suitable for early stress fractures that have not yet formed a complete crack, and radiation exposure is much higher than with standard X-rays, which is important to consider, especially in children.
- MRI (magnetic resonance imaging) is particularly useful for early detection of spondylolysis, as it can reveal inflammatory changes and edema in the pars interarticularis before a fracture develops. MRI also allows assessment of morphological changes and neurological complications, such as nerve root compression.

| Method | Advantages | Limitations |
|---|---|---|
| X-ray (Radiograph) | Fast and inexpensive; low radiation exposure; good for fully developed fractures | Does not detect early stress fractures; less sensitive for initial microfractures |
| CT (Computed Tomography) | Detailed view of bone structures; gold standard for visualizing fractures | High radiation exposure; limited for early stress fractures |
| MRI (Magnetic Resonance Imaging) | Best for early detection of inflammation and edema; can assess neurological complications and morphological changes | Less detailed for bone compared to CT; more expensive and longer exam |
| Combination of methods | Allows precise confirmation of diagnosis and monitoring of progression or treatment | Requires coordination; may involve higher costs and longer exam times |
Treatment of Spondylolysis
In most cases, spondylolysis is treated conservatively without surgery, especially in children and adolescents. The goal of treatment is to reduce pain, promote healing of the stress fracture, and gradually return the patient to daily activities and sports. Timely recognition and appropriate management generally lead to an excellent prognosis.
Conservative Treatment
Conservative treatment is the foundation of therapy and focuses on reducing pain, promoting healing of the stress fracture, and preventing disease progression. Typically, this involves temporarily reducing or stopping sports activities that place stress on the spine, particularly movements involving extension and rotation.
In young athletes, a lumbar brace may sometimes be used for approximately 6–12 weeks to reduce stress on the affected spinal segment and allow proper healing.
Physical therapy and targeted exercises play a crucial role, especially programs aimed at strengthening the core muscles, improving flexibility, and gradually returning to functional activities. Studies show that strengthening trunk stabilizers can significantly reduce lower back pain. Once symptoms have resolved and imaging confirms healing, young athletes can gradually resume sports activities.
Surgical Treatment
Surgery is considered when conservative therapy fails to produce improvement. It is estimated that about 9–15% of patients with spondylolysis may not respond to non-surgical treatment and may require an operation.
Surgery is usually considered for patients who, after more than six months of conservative therapy, continue to experience persistent pain, associated symptoms, and signs of a chronic pars interarticularis defect on imaging. A diagnostic anesthetic block of the pars defect may sometimes be performed to confirm that the segment is indeed the source of pain before making a final surgical decision.
There are generally two main types of surgical treatment:
- Direct repair of the pars interarticularis
This procedure aims to close the defect while preserving spinal mobility. It is most commonly recommended for younger patients and athletes with low-grade lesions. Various direct stabilization techniques have been developed, usually involving screws or pedicle fixation. - Spinal fusion
Spinal fusion is typically used in more severe cases or in patients with advanced instability, such as in spondylolisthesis. This procedure stabilizes the affected spinal segment and can significantly reduce pain but also decreases mobility of that part of the spine. Therefore, it is more often used in older patients, while for younger and physically active individuals, techniques that preserve spinal mobility are preferred whenever possible.
Conclusion
Although spondylolysis rarely causes symptoms in adults, it is a relatively common cause of lower back pain in children and adolescents, especially in young athletes who are exposed to repetitive spinal stress. Therefore, whenever a young athlete presents with lower back pain, this diagnosis should always be considered.
Diagnosis is made through a combination of clinical examination and imaging studies, with MRI playing a key role in the early detection of stress fractures. In most cases, treatment is conservative and includes temporary reduction of spinal load, physical therapy, and targeted core stabilization exercises. Surgery is required only in a small number of patients whose symptoms persist despite prolonged conservative therapy.
With timely diagnosis and appropriate rehabilitation, the prognosis of spondylolysis is generally very good, and most patients can successfully return to daily activities and sports.
Frequently Asked Questions
1. Can spondylolysis heal on its own?
Spondylolysis, especially in the case of an early stress fracture of the pars interarticularis, can often heal with appropriate conservative management. This usually involves temporarily reducing sports activities, targeted physical therapy, and gradual reloading of the spine. Healing is more likely in children and adolescents because their bones are still growing. Chronic or long-standing defects may remain as a stable bone gap, which often causes no symptoms.
2. What is the difference between spondylolysis and spondylolisthesis?
Spondylolysis refers to a bone defect or crack in the pars interarticularis of a vertebra. If this defect leads to forward slippage of one vertebra over another, it is called spondylolisthesis. In other words, spondylolysis can be a cause of spondylolisthesis (isthmic spondylolisthesis), but not all patients with spondylolysis develop vertebral slippage.
3. How long does recovery from spondylolysis take?
Recovery time depends on the patient’s age, the severity of the bone defect, and how early the diagnosis is made. In most cases, conservative treatment lasts several months. Young athletes can often return to full sports activities within 3 to 6 months, once pain subsides and imaging shows stabilization or healing of the defect.
4. Can athletes continue to play sports with spondylolysis?
During the acute phase, it is generally recommended to temporarily stop activities that stress the spine, especially movements involving extension and rotation. After pain decreases and rehabilitation is complete, most athletes can gradually return to training. Strengthening the core and spinal stabilizers is important to reduce the risk of reinjury and potential development of spondylolisthesis.
Li N, Amarasinghe S, Boudreaux K, Fakhre W, Sherman W, Kaye AD. Spondylolysis. Orthop Rev (Pavia). 2022 Aug 30;14(3):37470. doi: 10.52965/001c.37470. PMID: 36045696; PMCID: PMC9425520.
Lemoine T, Fournier J, Odent T, Sembély-Taveau C, Merenda P, Sirinelli D, Morel B. The prevalence of lumbar spondylolysis in young children: a retrospective analysis using CT. Eur Spine J. 2018 May;27(5):1067-1072. doi: 10.1007/s00586-017-5339-5. Epub 2017 Oct 13. PMID: 29030702.
Kalichman L, Kim DH, Li L, Guermazi A, Berkin V, Hunter DJ. Spondylolysis and spondylolisthesis: prevalence and association with low back pain in the adult community-based population. Spine (Phila Pa 1976). 2009 Jan 15;34(2):199-205. doi: 10.1097/BRS.0b013e31818edcfd. PMID: 19139672; PMCID: PMC3793342.











{kind=link}
{kind=link}