Shoulder pain is one of the most common musculoskeletal complaints, affecting a large portion of the adult population and often interfering with daily activities and sleep. Despite its prevalence, accurate diagnosis can be challenging—especially when evaluating rotator cuff injuries.
In clinical practice, individual rotator cuff muscles are not always assessed precisely. The infraspinatus, a key muscle responsible for external rotation and shoulder stability, is frequently overlooked.
The infraspinatus test is a simple and effective clinical tool used to assess its function. In this article, you will learn how to perform the test, interpret the results, and apply it in everyday clinical practice.
Key Clinical Points – Infraspinatus Test
- The infraspinatus test is a clinical examination maneuver used to assess external rotation strength and posterior rotator cuff function.
- It primarily evaluates the infraspinatus muscle, a key stabilizer of the shoulder responsible for external rotation and dynamic joint control.
- A positive test may indicate infraspinatus tendinopathy, partial tear, full-thickness rupture, or suprascapular nerve involvement.
- The test is most useful in patients presenting with posterior shoulder pain, weakness in external rotation, or suspected rotator cuff injury.
- It should always be interpreted together with patient history, physical examination, and other shoulder special tests to improve diagnostic accuracy.
- Cluster testing significantly increases reliability, as no single shoulder test is sufficient to confirm or exclude pathology.
What Is the Infraspinatus Test?
The infraspinatus test is a clinical examination maneuver used to assess the function and integrity of the infraspinatus muscle, one of the four muscles that make up the rotator cuff. It is primarily performed as part of a focused shoulder examination when rotator cuff pathology is suspected.
This test specifically evaluates external rotation strength of the shoulder, which is the main function of the infraspinatus muscle. By applying resistance during external rotation, the clinician can determine whether the muscle and its tendon are functioning properly or if there is weakness, pain, or dysfunction.
Its relevance lies in the fact that deficits in external rotation are often associated with infraspinatus tendinopathy, partial tears, or more significant rotator cuff injuries. Because these conditions can present with overlapping symptoms, isolating the infraspinatus during physical examination is clinically valuable.
In practice, the infraspinatus test is not used in isolation but as part of a broader shoulder assessment that includes patient history, range of motion testing, and other special tests to improve diagnostic accuracy.
Anatomy and Function of the Infraspinatus
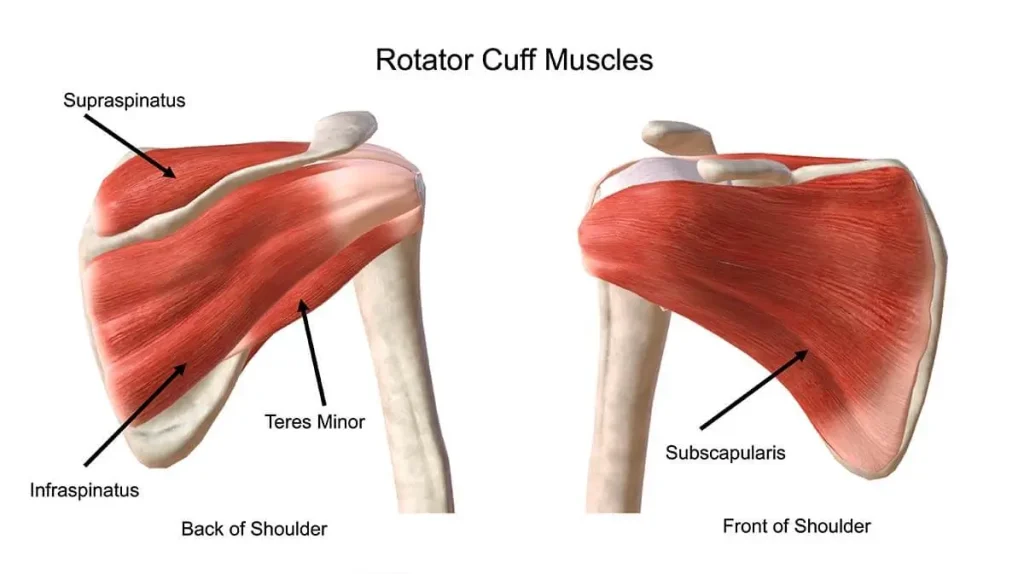
The infraspinatus is one of the four muscles of the rotator cuff and plays a central role in shoulder biomechanics. It originates from the infraspinous fossa of the scapula, occupying most of the posterior surface of the scapula below the scapular spine. From there, its fibers converge laterally and insert onto the middle facet of the greater tubercle of the humerus. The muscle is innervated by the suprascapular nerve (C5–C6), which also supplies the supraspinatus.
Functionally, the infraspinatus is the primary external rotator of the glenohumeral joint, especially when the arm is in a neutral position. In addition to producing external rotation, it contributes significantly to dynamic stabilization of the shoulder by centering the humeral head within the glenoid fossa during movement.
From a biomechanical perspective, the infraspinatus works as part of a force couple with the subscapularis muscle. While the subscapularis generates internal rotation and anterior stabilization, the infraspinatus provides opposing posterior force and external rotation. This balance is essential for maintaining joint congruency and preventing excessive translation of the humeral head.
When the infraspinatus is injured—whether through tendinopathy, partial tear, or full-thickness rupture—this balance is disrupted. Patients typically develop weakness in external rotation, reduced shoulder stability, and posterior or lateral shoulder pain. In more severe cases, compensatory muscle activation may mask early deficits, delaying diagnosis and contributing to chronic dysfunction.
When to Use the Infraspinatus Test
The infraspinatus test is indicated when rotator cuff pathology is suspected, particularly involving the posterior cuff. In clinical practice, it is most useful in patients presenting with shoulder pain that is mechanical in nature and worsens with movement, especially during activities involving external rotation or overhead positioning.
Patients typically describe posterior or lateral shoulder pain, often accompanied by weakness when rotating the arm outward or performing pushing and lifting movements away from the body. Night pain is also common, particularly when lying on the affected shoulder, which can significantly affect sleep quality.
The test is especially relevant in two main groups. The first includes athletes exposed to repetitive overhead loading, such as swimmers, tennis players, and baseball athletes, where chronic microtrauma can lead to tendinopathy or partial tearing. The second group includes older patients, in whom degenerative rotator cuff changes are far more common and may present with gradual onset weakness and pain.
There are also important limitations to consider. The infraspinatus test should always be interpreted within a broader clinical context, as isolated weakness or pain is not specific and may overlap with other conditions such as cervical radiculopathy, subacromial impingement, or pathology of adjacent rotator cuff structures. In acute trauma settings, or when fracture or dislocation is suspected, the test should be avoided until more serious injury has been excluded.
Clinical Insight
The infraspinatus test is most valuable when integrated into a full shoulder examination rather than used in isolation. While a positive finding may suggest rotator cuff pathology, it is not specific and must be interpreted alongside patient history and other clinical tests.
Weakness in external rotation is generally more clinically significant than pain alone, particularly in differentiating true tendon dysfunction from nonspecific shoulder pain.
Careful patient selection is essential, as acute trauma or neurological conditions may mimic infraspinatus dysfunction and require alternative diagnostic pathways.
How to Perform the Infraspinatus Test
The infraspinatus test is a straightforward clinical maneuver, but its diagnostic value depends on correct technique, proper stabilization, and careful observation of subtle findings.
The patient should be positioned either seated or standing in a relaxed posture with the arms resting at the sides of the body. The elbows are flexed to 90 degrees, and the shoulders are kept in a neutral position without abduction or flexion. This positioning helps isolate the external rotators of the shoulder and reduces compensatory movements.
The examiner stands facing the patient to ensure symmetry and direct comparison between both sides. Hands are placed on the distal forearms or wrists, allowing controlled application of resistance during the movement.
The patient is then instructed to externally rotate both shoulders against resistance. The movement should be slow and controlled, with gradual increase in resistance applied by the examiner. It is important to maintain consistency between sides to allow accurate comparison.
Stabilization is a key component of the test. The examiner should keep the patient’s elbows close to the torso throughout the maneuver to prevent substitution from larger muscle groups such as the deltoid or trapezius. Without proper stabilization, the test may lose specificity and lead to false interpretation.
During the test, the clinician should observe several key elements, including:
- Strength of external rotation compared to the contralateral side
- Presence of pain during resisted movement
- Quality of movement and any compensatory patterns
- Ability to maintain resistance without early fatigue or collapse
Clinical Insight
A positive infraspinatus test is typically characterized by weakness, pain, or both during resisted external rotation. However, these findings should never be interpreted in isolation and must always be correlated with a full clinical shoulder examination, including history, functional assessment, and additional special tests.
Interpretation of the Infraspinatus Test
Correct interpretation of the infraspinatus test is essential, as clinical meaning depends not only on whether the test is positive or negative, but also on the quality of the findings—particularly the distinction between pain and true weakness.
Positive Test
A positive infraspinatus test is typically defined by the presence of weakness during resisted external rotation, pain, or both. However, in clinical practice, the distinction between pain and true weakness is crucial. Pain alone may indicate tendinopathy or local inflammation, while true strength deficit is more suggestive of structural tendon damage.
From a diagnostic perspective, a positive test may indicate several underlying conditions. A rotator cuff tear of the infraspinatus is one of the most significant causes, particularly when there is clear side-to-side weakness. Tendinopathy can also produce pain with preserved or mildly reduced strength. In some cases, suprascapular nerve involvement may lead to isolated weakness due to impaired muscle activation.
Negative Test
A negative infraspinatus test indicates preserved strength and absence of pain during resisted external rotation. In a typical clinical context, this makes significant infraspinatus dysfunction less likely.
However, a negative result does not completely exclude pathology. Small partial-thickness tears, early degenerative changes, or compensated movement patterns may still produce false-negative findings. Additionally, other shoulder structures may be responsible for symptoms even when infraspinatus function appears normal.
For this reason, the infraspinatus test should always be interpreted as part of a broader clinical assessment rather than a standalone diagnostic tool.
Clinical Accuracy and Limitations
The infraspinatus test has moderate clinical accuracy, with sensitivity and specificity estimated in the range of approximately 70–80%, depending on patient population and examiner technique. While useful, it is not sufficiently accurate to confirm or exclude pathology on its own.
A key limitation is that shoulder pain is often multifactorial, meaning a positive test may reflect not only infraspinatus pathology but also conditions such as subacromial impingement, cervical radiculopathy, or dysfunction of adjacent rotator cuff muscles. This overlap reduces diagnostic specificity in isolation.
Another issue is compensatory muscle activation, which can mask true weakness in partial tears or early degenerative changes, leading to false-negative findings. Patient pain tolerance and examiner variability further influence reliability.
For this reason, the infraspinatus test should always be interpreted within a cluster of clinical findings, rather than as a standalone diagnostic tool. Combining it with history, range of motion assessment, and additional rotator cuff tests significantly improves diagnostic accuracy and clinical decision-making.
Differential Diagnosis
A positive or painful infraspinatus test is not specific to isolated infraspinatus pathology. Several other shoulder and cervical conditions can present with similar clinical findings, making differential diagnosis essential.
Common conditions to consider include:
- Supraspinatus tendinopathy or tear – often presents with pain during abduction rather than isolated external rotation weakness
- Subacromial impingement syndrome – typically causes pain with overhead activity and positive impingement signs
- Teres minor involvement – may mimic infraspinatus weakness but is less commonly isolated
- Cervical radiculopathy (C5–C6) – may present with radiating pain and neurological symptoms such as numbness or reflex changes
- Adhesive capsulitis – global restriction of both active and passive range of motion
Distinguishing these conditions relies on a combination of clinical findings. Isolated external rotation weakness is more suggestive of infraspinatus involvement, while global pain and stiffness point toward adhesive capsulitis. Neurological signs favor a cervical origin, whereas impingement typically produces pain in specific arc movements rather than true strength deficits.
Accurate diagnosis therefore depends on integrating the infraspinatus test within a full shoulder and neurological examination.
Role in Clinical Practice
In clinical practice, the infraspinatus test is best viewed as a targeted screening tool within a structured shoulder examination, rather than a standalone diagnostic method. It is typically used early in the physical assessment to help narrow the differential diagnosis when rotator cuff pathology is suspected.
In a practical workflow, the evaluation begins with a detailed patient history, followed by inspection, range of motion testing, and basic strength assessment. The infraspinatus test is then used as part of a focused set of special tests to identify posterior cuff involvement. In this context, it functions primarily as a screening test, helping to raise or lower clinical suspicion rather than definitively confirming disease.
From a clinical decision-making perspective, a clearly positive test—especially when associated with objective weakness and functional impairment—may increase the likelihood of significant rotator cuff pathology. In such cases, further imaging, most commonly MRI or high-resolution ultrasound, is often indicated to confirm the extent of tendon involvement and guide treatment planning.
However, a negative test does not eliminate the need for further evaluation if clinical suspicion remains high. As with most musculoskeletal examinations, the greatest value of the infraspinatus test lies in its integration within a broader diagnostic framework rather than isolated interpretation.
Practical Clinical Tips
In daily clinical practice, the accuracy of the infraspinatus test depends more on technique and interpretation than on complexity.
- First, always stabilize the elbow against the torso to prevent compensatory movements from the deltoid or trapezius, as this is the most common source of false results.
- Second, compare both sides systematically—side-to-side asymmetry is often more clinically meaningful than absolute strength.
- Third, distinguish carefully between pain and true weakness; pain alone is more suggestive of tendinopathy, while consistent strength loss raises concern for structural tear.
- Fourth, apply resistance gradually rather than abruptly, as sudden force can provoke guarding and reduce test reliability.
- Finally, integrate the test into a broader shoulder assessment rather than interpreting it in isolation, since diagnostic accuracy significantly improves when combined with history and additional special tests.
These small technical refinements can substantially increase the clinical value of the examination and reduce
FAQ
What does a positive infraspinatus test mean?
A positive infraspinatus test indicates weakness, pain, or both during resisted external rotation of the shoulder. Clinically, this may suggest infraspinatus tendinopathy, partial or full-thickness rotator cuff tear, or in some cases suprascapular nerve involvement. The most clinically significant finding is true weakness compared to the contralateral side, which increases suspicion of structural tendon pathology.
How accurate is the infraspinatus test?
The infraspinatus test has moderate diagnostic accuracy, with reported sensitivity and specificity generally around 70–80%, depending on technique and patient population. It is not sufficiently accurate to confirm or exclude rotator cuff pathology on its own. Its diagnostic value increases significantly when used as part of a cluster of shoulder examination tests combined with patient history and imaging when necessary.
What muscles does the test evaluate?
The infraspinatus test primarily evaluates the infraspinatus muscle, which is part of the rotator cuff and responsible for external rotation of the shoulder. It may also indirectly assess the teres minor muscle, which assists in external rotation. The test helps determine the functional integrity of the posterior rotator cuff complex and its ability to stabilize the glenohumeral joint.
Is it painful?
The infraspinatus test may or may not be painful depending on the underlying condition. Pain during the test often suggests tendinopathy or inflammation of the rotator cuff, while painless weakness is more concerning for structural damage such as a tendon tear or neurological involvement. However, pain alone is not specific and must be interpreted alongside strength testing and other clinical findings.
Conclusion
The infraspinatus test is a simple yet clinically valuable component of the shoulder examination, providing important information about the integrity and function of the posterior rotator cuff. When performed correctly, it helps identify potential infraspinatus dysfunction and contributes to a more focused and efficient diagnostic process.
However, its true value lies in correct interpretation rather than execution alone. Differentiating between pain and true weakness, and understanding the limitations of the test, is essential to avoid misdiagnosis and overinterpretation of isolated findings.
When integrated into a comprehensive clinical assessment, the infraspinatus test supports earlier recognition of rotator cuff pathology, more accurate clinical decision-making, and more appropriate referral for imaging or specialist care when needed. For patients, this translates into faster diagnosis, more targeted treatment, and improved functional outcomes.
Park HB et al. Diagnostic accuracy of clinical tests for the infraspinatus tendon. Journal of Bone and Joint Surgery (Am). PubMed: Infraspinatus clinical test diagnostic accuracy study
Physiopedia. Infraspinatus Test (External Rotation Strength Test). Clinical guide: How to perform the Infraspinatus Test step-by-step
AAOS (American Academy of Orthopaedic Surgeons). Rotator Cuff Tears Overview and Physical Examination. AAOS guideline: Rotator cuff injury diagnosis and shoulder examination
Magee DJ. Orthopedic Physical Assessment. Elsevier. Clinical textbook: Orthopedic shoulder examination techniques (Magee)
StatPearls. Rotator Cuff Injury. NCBI Bookshelf. Evidence-based review: Rotator cuff injury diagnosis and management
BMJ Best Practice. Shoulder impingement syndrome and rotator cuff pathology. BMJ clinical decision guide: Shoulder impingement and rotator cuff pathology
Kuhn JE. Exercise in the treatment of rotator cuff impingement. J Shoulder Elbow Surg. Systematic review: Rotator cuff rehabilitation and clinical outcomes
Clinical Orthopaedics and Related Research. Physical examination of shoulder disorders. Clinical orthopedics reference: Shoulder physical examination findings
TeachMeAnatomy. Rotator Cuff Muscles and Clinical Testing. Educational guide: Rotator cuff anatomy and clinical function