
Hip pain is a common symptom that can significantly limit everyday activities such as walking, standing, or sitting. It can affect people of all ages, and the causes of hip pain often vary depending on age, gender, and lifestyle.
In many cases, hip pain is difficult to pinpoint. The discomfort may not be felt only in the hip joint itself but can also appear in the groin or thigh. Because of this, identifying the true source of hip pain can be challenging.
Understanding the most common causes of hip pain, recognizing early symptoms, and seeking timely medical advice are essential for maintaining joint function and overall quality of life.
This article explains the most common causes of hip pain, outlines how hip pain is diagnosed, and reviews available treatment options. Below, you will find a clear overview of the 10 most common conditions associated with hip pain.
- Hip pain may originate from the joint itself or from surrounding structures such as muscles, tendons, or the lumbar spine.
- Pain location is clinically important: anterior, lateral, and posterior hip pain are associated with different underlying conditions.
- Common causes include osteoarthritis, trochanteric pain syndrome, labral tears, and referred pain from the spine.
- Diagnosis is based on clinical examination supported by imaging such as X-ray or MRI.
- Conservative treatment is first-line and includes physiotherapy, medications, and lifestyle modification.
- Surgical intervention is reserved for severe or refractory cases.
- Early evaluation improves functional outcomes and helps prevent long-term joint degeneration.
Hip Anatomy and Function
To better understand hip pain, it is important to first look at the structure and function of the hip joint.
Structure of the Hip Joint
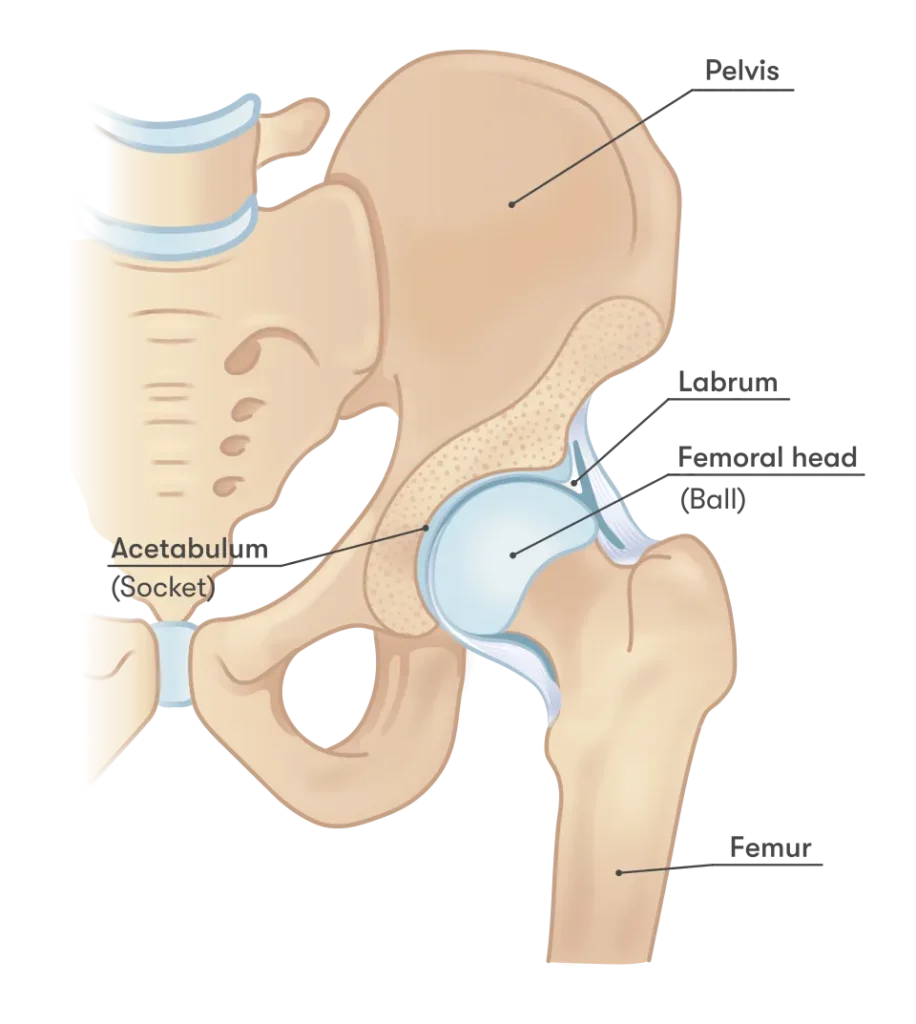
The hip joint is a synovial ball-and-socket joint. The head of the femur (thigh bone) forms the “ball,” while the socket is a cup-shaped part of the pelvis known as the acetabulum.
This structure gives the hip joint both strength and flexibility. It is surrounded by a strong joint capsule and reinforced by ligaments, which provide stability while still allowing movement in multiple directions.
One of the primary roles of the hip joint is to transfer body weight between the upper and lower body, making it essential for standing, walking, and overall mobility.
Cartilage and Joint Protection
The inner rim of the acetabulum is lined with a fibrocartilaginous structure called the labrum. The labrum deepens the socket and helps stabilize the hip joint while reducing friction during movement.
The surfaces of the bones within the hip joint are covered with smooth articular cartilage. This cartilage distributes load and allows bones to glide smoothly against each other.
Maintaining healthy cartilage is critical for preventing hip pain and preserving long-term joint function.
Muscles and Range of Motion
The hip joint works closely with surrounding muscles, which allow a wide range of motion. These movements include:
- Flexion and extension
- Abduction and adduction
- Internal and external rotation
Because of this, the hip is the second most mobile joint in the body, after the shoulder.
Hip Pain and Nerve Connection
The hip joint is closely connected to nerves from the lower spine (lumbosacral region). Because of this, hip pain is sometimes confused with pain originating from the lower back.
Understanding this connection is important when identifying the true cause of hip pain and choosing the right treatment approach.
Hip Pain Symptoms: What They Reveal About the Cause
Hip pain symptoms can vary widely, ranging from a dull, persistent ache to sudden, sharp pain that makes movement difficult. The way hip pain presents itself often provides important clues about the underlying cause.
Hip pain is not always felt directly in the hip joint. In many cases, it may appear in the groin, thigh, or even the buttocks. This can make it more difficult to identify the true source of hip pain.
Understanding hip pain symptoms — including the type of pain, its intensity, and its location — is essential for determining the cause and choosing the right treatment.
How Hip Pain Symptoms Help Identify the Cause
Different conditions that cause hip pain often produce specific and recognizable symptoms. Paying attention to these patterns can help narrow down the possible causes of hip pain.
Common Hip Pain Symptoms
- Pain location – hip pain may be felt directly in the hip joint, but also in the groin, buttocks, or lower back.
- Radiating pain – hip pain can spread down the thigh toward the knee, along the front or side of the leg (hip pain and leg pain / hip pain and groin pain). This pattern is commonly seen in hip osteoarthritis, hip impingement, or nerve compression in the lower spine.
- Specific pain points – some patients can point to precise areas such as the greater trochanter, which can help identify conditions like greater trochanteric pain syndrome.
- Type of pain – hip pain may be sharp, dull, or stabbing, depending on the underlying cause.
- Duration and triggers – hip pain may be constant or occur only during certain movements or activities.
- Activity-related pain – hip pain often worsens during walking, standing, or prolonged sitting.
- Night pain – hip pain at night or hip pain when sleeping may indicate conditions such as arthritis or inflammation.
- Limited range of motion – conditions like hip osteoarthritis can cause stiffness and difficulty with bending, rotating, or lifting the leg, making daily activities more challenging.
- Changes in walking pattern – people with hip pain may develop a limp to reduce discomfort; this may be due to pain (antalgic gait) or leg length differences.
How Is Hip Pain Diagnosed?
To successfully treat hip pain, it is essential to identify the underlying cause. An accurate diagnosis is the first step before starting any treatment plan.
If hip pain does not improve with short periods of rest, limits your daily activities, or affects your quality of life, you should consult a medical professional.
Medical History and Symptom Evaluation
Diagnosis of hip pain usually begins with a detailed conversation between the patient and the doctor.
Specialists such as physiatrists and orthopedic doctors will ask about:
- Hip pain symptoms
- Frequency and duration of hip pain
- Pain intensity and exact location
- Activities or movements that worsen or relieve hip pain
This information helps guide the diagnostic process and determine the next steps.
Physical Examination
After discussing symptoms, the doctor performs a physical examination.
This typically includes:
- Assessment of walking (gait analysis)
- Range of motion of the hip joint
- Muscle strength testing
- Specific clinical tests to reproduce hip pain
These findings help narrow down the possible causes of hip pain.
Imaging Tests for Hip Pain
If needed, additional diagnostic tests are used to confirm the cause of hip pain. Imaging methods allow detailed evaluation of the hip joint and surrounding tissues.
Common imaging tests include:
- X-ray
- Ultrasound
- CT scan
- MRI
X-ray of the Hip
An X-ray is usually the first imaging test for hip pain. It is widely available and provides a clear view of the bones in the hip and pelvis.
X-rays can help detect:
- Hip osteoarthritis (degenerative changes)
- Bone fractures
- Advanced avascular necrosis
- Femoroacetabular impingement (FAI)
Ultrasound of the Hip
Ultrasound is a quick, accessible, and cost-effective method. It is often used during a clinical examination.
While ultrasound cannot show the internal structure of the hip joint in detail, it is very useful for evaluating:
- Tendons
- Muscles
- Soft tissue structures around the hip
It is especially helpful in identifying problems in the outer hip (trochanteric region), a common source of hip pain.
CT Scan (Computed Tomography)
CT scans are less commonly used for hip pain diagnosis but can be very useful in specific cases.
They provide detailed cross-sectional images of the hip, which can be combined into a 3D view. CT is particularly helpful for detecting abnormal hip joint shape or structural changes.
MRI of the Hip
MRI (Magnetic Resonance Imaging) is one of the best methods for evaluating soft tissues.
MRI can detect:
- Tendon tears
- Labral injuries
- Joint effusion
- Inflammation of surrounding structures
It is also the most sensitive method for early detection of avascular necrosis of the femoral head.
| Diagnostic Method | Advantages | Limitations |
|---|---|---|
| X-ray (Radiography) | Widely available and quick; low cost; effective for detecting bone fractures and advanced hip osteoarthritis | Limited ability to detect early-stage conditions; does not show soft tissues such as cartilage or labrum |
| Ultrasound | Non-invasive, fast, and cost-effective; useful for evaluating tendons, muscles, and soft tissue around the hip | Cannot visualize internal structures of the hip joint; limited for deep joint pathology |
| CT (Computed Tomography) | Provides detailed 3D images of bone structures; useful for complex fractures and abnormal joint anatomy | Exposure to radiation; less effective for evaluating soft tissue injuries |
| MRI (Magnetic Resonance Imaging) | Best method for soft tissue evaluation; detects labral tears, tendon injuries, and early avascular necrosis | More expensive; longer examination time; less accessible in some settings |
| Combination of Methods | Provides the most accurate diagnosis; allows detailed assessment and monitoring of hip pain causes | May require multiple appointments; higher overall cost and time investment |
Hip Pain: 10 Most Common Diagnoses
In this section, we will present a structured overview of the 10 most common conditions that cause hip pain.
To make the information easier to understand, these conditions are grouped according to the area where hip pain is most commonly felt.
This approach helps identify patterns in hip pain symptoms and makes it easier to associate specific types of hip pain with their most likely causes.
Hip Pain: Classification by Location and Common Causes
Anterior Hip Pain (Front Hip Pain)
In most cases, anterior hip pain is caused by conditions affecting the hip joint itself. It can also result from overuse or strain of the hip flexor tendons.
In some cases, hip pain in the front of the hip or groin may be referred pain, meaning it originates from another area but is felt in the hip region.
Pain that is referred from the abdominal cavity may be related to conditions such as:
- appendicitis
- hernia
- bladder issues
- or gynecological conditions (most commonly ovarian cysts)
For more information about groin-related pain, you can read a separate article on groin pain and its most common causes.
Most Common Causes in Older Adults
In older individuals, the most frequent causes of anterior hip pain include:
- Hip osteoarthritis
- Hip fractures
- Avascular necrosis of the femoral head
Most Common Causes in Younger and Active Individuals
In younger, physically active individuals and athletes, anterior hip pain is most often caused by:
- Labral tears
- Femoroacetabular impingement (FAI)
- Femoral neck stress fractures
1. Hip Osteoarthritis (Hip Arthritis / Coxarthrosis)
Hip osteoarthritis is a degenerative joint disease characterized by the gradual breakdown of cartilage within the hip joint. It is most common in older adults and leads to pain, stiffness, and reduced mobility.
In older individuals, hip osteoarthritis is the most common cause of anterior hip pain. The condition can significantly reduce physical activity and negatively affect quality of life.
The onset of symptoms is usually gradual, although some patients may recall a previous injury or fall. Patients most commonly report pain during walking, and sometimes while sitting—especially in a low chair or car seat—as well as when rising from a seated position. As the condition progresses, limping may develop.
Diagnosis of Hip Osteoarthritis
Diagnosis involves a comprehensive evaluation, including:
- Clinical examination
Reduced range of motion in the hip and pain provoked by specific movements - Imaging studies
X-ray of the hips and pelvis typically shows joint space narrowing and the formation of osteophytes (bone spurs) - Diagnostic injections (in unclear cases)
Ultrasound-guided anesthetic injections may help differentiate hip joint pain from referred pain originating in the lumbar spine
Treatment of Hip Osteoarthritis
Treatment depends on the severity of the condition and may include:
- Lifestyle modifications
Weight reduction and activity adjustment as first-line management - Assistive devices
Walking aids such as canes or crutches help reduce joint load, decrease pain, and improve mobility - Medications
Pain relievers (analgesics) - Physical therapy
Strengthening exercises for the muscles around the hip and pelvis, as well as range-of-motion exercises - Surgical treatment
In advanced stages, hip replacement surgery (total hip arthroplasty) may be indicated to restore function and reduce symptoms
2. Hip Fracture (Hip Break)
Hip fractures most commonly occur in older adults, usually after a fall or trauma. They are often associated with osteoporosis, a condition that weakens the bones and increases the risk of fracture even after minor injuries.
Patients typically experience severe hip or groin pain and are unable to stand or walk on the affected leg. The leg may appear shortened, externally rotated, and positioned away from the body when lying down.
Hip fracture is a medical emergency and requires immediate hospital treatment. Most fractures are clearly visible on X-ray and require urgent surgical management, followed by rehabilitation.
3. Femoroacetabular Impingement (FAI)
Femoroacetabular impingement (FAI), also known as hip impingement, is one of the most common causes of hip pain in young adults. It occurs when there is abnormal contact between the femoral head and the acetabulum due to bone deformities.
The condition can be caused by a cam deformity (extra bone on the femoral head or neck) or a pincer deformity (excess coverage of the femoral head by the acetabulum).
Symptoms typically develop gradually without a specific injury. FAI is more common in athletes, especially those involved in sports that require deep hip flexion and a wide range of motion.
Patients often experience pain during movement, particularly with hip flexion, rotation, or prolonged activity. Clinical examination may reproduce pain with specific tests such as FADIR and FABER, which indicate hip joint pathology.
X-ray imaging can help identify cam and pincer deformities and confirm the diagnosis.
4. Labral Tear (Hip Labrum Injury)
The hip labrum is a ring of cartilage that surrounds the acetabulum (hip socket). It helps stabilize the joint, reduces friction, and distributes load across the hip. It also creates a suction effect that improves joint stability and helps prevent dislocation.
Labral tears are often associated with femoroacetabular impingement (FAI) and are common in athletes or individuals with a history of hip trauma.
Symptoms
- Pain in the front of the hip or groin
- Pain that may radiate toward the knee
- Gradual onset of symptoms
- Nocturnal hip pain (pain during sleep)
- Dull, constant pain with episodes of sharp pain during movement
- Pain worsened by activities such as walking, running, or prolonged sitting
- Clicking, catching, or locking sensations in the hip
Diagnosis
- X-ray
Does not show the labrum directly but may reveal associated FAI changes (cam and pincer deformities) - MRI
Best imaging method to visualize labral and cartilage injuries - MR arthrography
In some cases, contrast-enhanced MRI is needed for more accurate detection
Treatment
Treatment depends on severity and symptoms:
- Conservative treatment
Rest, pain medication, activity modification, physical therapy, and sometimes corticosteroid injections - Surgical treatment
Arthroscopic procedures to repair or reconstruct the labrum
Aims to preserve joint function and reduce the risk of early osteoarthritis
5. Femoral Neck Stress Fracture (Hip Stress Fracture)
A femoral neck stress fracture is caused by repetitive overload of the hip joint rather than a single traumatic event. It is relatively rare and most commonly seen in high-impact athletes, such as long-distance runners and military personnel.
The condition typically develops gradually without a clear injury. Pain improves with rest and worsens with weight-bearing activities. In some cases, the pain may radiate to the groin or down the leg, making diagnosis more challenging.
If left untreated, a stress fracture can progress to a complete fracture with serious complications.
Symptoms
- Gradual onset of hip or groin pain
- Pain that worsens with activity and improves with rest
- Pain that may radiate to the groin or leg
- Difficulty bearing weight on the affected side
- Increasing pain with continued activity
Diagnosis
- X-ray
Often normal in early stages and may not detect the fracture - MRI
The most reliable method for early detection of stress fractures
Treatment
- Conservative treatment
Rest, activity modification, and gradual return to activity after healing
Rehabilitation and physical therapy - Surgical treatment
In some cases, surgical fixation is required to prevent fracture progression
Complications (if untreated)
- Progression to a complete fracture
- Non-union (failure of bone to heal)
- Avascular necrosis (bone tissue death)
- Long-term disability
6. Avascular Necrosis of the Femoral Head (Hip Osteonecrosis)
Avascular necrosis (AVN) of the femoral head, also known as hip osteonecrosis, is a condition caused by reduced or interrupted blood supply to the femoral head. This leads to the death of bone cells and bone marrow, resulting in gradual collapse of the bone structure.
If left untreated, the condition can progress and lead to secondary hip osteoarthritis. Avascular necrosis is responsible for a significant percentage of hip replacement surgeries.
Several factors can contribute to the development of avascular necrosis:
Causes of Avascular Necrosis (AVN) of the Femoral Head
- Trauma – Fractures or dislocation of the femoral head are the most common cause of avascular necrosis of the hip.
- Corticosteroids – Long-term corticosteroid use is the second most common cause of AVN. Up to 80% of non-traumatic cases are associated with steroid use. Although the exact mechanism is not fully understood, there is a well-established link.
- Alcohol – Chronic alcohol consumption is also a significant risk factor, although the exact mechanism remains unclear.
- Sickle Cell Disease – A hereditary condition in which red blood cells become misshapen and rigid, impairing blood flow and leading to bone ischemia and infarction.
- Autoimmune Diseases – Chronic inflammatory and autoimmune conditions, such as systemic lupus erythematosus (SLE), are known risk factors for AVN of the hip.
- Vascular Diseases and Cytotoxic Drugs – Conditions such as diabetes-related vascular disease, as well as the use of cytotoxic medications in cancer treatment, can contribute to the development of osteonecrosis.
Legg-Calvé-Perthes Disease (Pediatric Hip Osteonecrosis)
Legg-Calvé-Perthes disease is a form of avascular necrosis of the femoral head that occurs in children. The exact cause is unknown. A reduced blood supply leads to necrosis of the femoral head, resulting in bone deformation and a significantly increased risk of developing hip osteoarthritis later in life.
Symptoms
In the early stages, patients may be asymptomatic. When symptoms do appear, they most commonly include:
- Pain in the front of the hip or groin
- Hip or leg pain that may radiate
- Pain that worsens with weight-bearing
- Pain that may persist even at rest
- Nocturnal hip pain (pain during sleep)
Diagnosis
Early diagnosis is essential to prevent collapse of the femoral head and long-term complications. Diagnosis is based on clinical evaluation and imaging studies:
- X-ray
Useful in advanced stages, when bone collapse and deformity of the femoral head are already present - MRI (Magnetic Resonance Imaging)
The gold standard for early detection of avascular necrosis
MRI can identify bone marrow changes, the size and location of necrosis, and involvement of the articular cartilage, all of which are important for prognosis and treatment planning
Treatment
Treatment of avascular necrosis can be conservative or surgical, depending on individual factors:
- Patient’s age
- Severity and intensity of pain
- Location and extent of necrosis
- Presence of other medical conditions (comorbidities)
- Whether femoral head collapse has occurred (the most important factor)
Treatment options may include conservative management or surgical procedures such as hip replacement in advanced cases.
Lateral Hip Pain (Outer Hip Pain)
The most common cause of pain on the outer side of the hip is greater trochanteric pain syndrome (GTPS).
7. Greater Trochanteric Pain Syndrome (Trochanteric Bursitis)
Greater trochanteric pain syndrome is the leading cause of lateral hip pain. It is a broad term that includes several related conditions:
- Trochanteric bursitis
- External snapping hip
- Gluteal tendinopathy
This condition typically presents as pain on the outer side of the hip, which worsens with walking, physical activity, prolonged sitting, or lying on the affected side. Tenderness over the lateral hip is commonly present when pressure is applied.
Symptoms usually develop gradually and are not associated with a specific injury. It most commonly affects women between the ages of 40 and 60.
Causes of Greater Trochanteric Pain Syndrome
- Tendon degeneration and inflammation – Most commonly involves degeneration of the gluteal tendons attaching to the greater trochanter, along with associated bursae (bursitis).
- Iliotibial band friction – Friction over the greater trochanter and external snapping hip can contribute to symptom development.
- Repetitive activities – Prolonged walking, running, or repetitive movements can irritate tissues on the outer side of the hip.
- Mechanical overload – Intense training or long-distance running can increase stress on the lateral hip structures.
- Sedentary lifestyle – Reduced muscle strength and hip stability may increase the risk of developing pain.
- Excess body weight – Increases load on the hip joint and surrounding tendons.
- Leg length discrepancy – Unequal leg length or conditions such as scoliosis can lead to abnormal loading of the hip and tendon irritation.
Greater trochanteric pain syndrome is often associated with bursitis; however, current evidence suggests that gluteal tendinopathy and partial or complete tears of the gluteus medius tendon are the primary underlying causes.
Diagnosis
The diagnosis of greater trochanteric pain syndrome is primarily clinical. A detailed patient history combined with a targeted physical examination is usually sufficient to establish the diagnosis.
During evaluation, it is essential to rule out other common causes of hip pain, particularly hip osteoarthritis and femoroacetabular impingement (FAI), which may present with similar symptoms.
- X-ray imaging
Typically used to exclude other conditions rather than confirm the diagnosis, as it does not clearly show soft tissue pathology - Ultrasound (US)
A useful and accessible diagnostic tool that can demonstrate thickening and structural changes of the gluteal tendons, as well as inflammation of the trochanteric bursa - MRI (Magnetic Resonance Imaging)
Usually not required, but indicated when a tendon tear is suspected or when the diagnosis remains unclear
Treatment
In the vast majority of cases, treatment is conservative and focuses on reducing pain and improving hip function.
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
Help reduce pain and inflammation - Physical therapy
Focused on strengthening the hip abductors and improving pelvic stability - Activity modification
Avoiding activities that aggravate symptoms, such as prolonged standing, running, or lying on the affected side - Corticosteroid injections
May be considered in selected cases to reduce inflammation and pain
Surgical treatment is rarely required and is reserved for patients with persistent symptoms or confirmed tendon tears that do not respond to conservative management.
Learn More
For a more detailed explanation, read our full article on Trochanteric Bursitis and Greater Trochanteric Pain Syndrome (GTPS) .
Posterior Hip Pain (Back of the Hip)
Pain in the back of the hip can be challenging to diagnose, as it may originate from multiple sources. The range of possible causes includes musculoskeletal conditions, as well as referred pain from the pelvis or internal organs.
Patients with referred pain may report a history of recurrent symptoms related to the menstrual cycle, or symptoms involving the urinary or digestive system. This highlights the importance of a thorough clinical evaluation when assessing posterior hip pain.
Common Musculoskeletal Causes
The most frequent musculoskeletal causes of posterior hip pain include:
- Deep gluteal pain syndrome
- Piriformis syndrome
- Referred pain from the lumbar spine
- Sacroiliac (SI) joint dysfunction
- Hamstring-related pain or injuries
8. Piriformis Syndrome and Deep Gluteal Syndrome
Piriformis syndrome is caused by compression of the sciatic nerve by the piriformis muscle in the posterior hip region. This nerve compression leads to pain in the hip and buttock, often accompanied by sciatica-like symptoms, such as burning pain radiating down the leg.
Piriformis syndrome is considered a subset of deep gluteal syndrome, a broader condition that involves compression of the sciatic and/or pudendal nerve by surrounding muscles, including:
- Piriformis
- Gemelli muscles
- Obturator internus
- Proximal hamstring muscles
Symptoms
Patients with deep gluteal syndrome typically experience:
- Deep, persistent pain in the buttock
- Pain that worsens with prolonged sitting
- Radiating pain down the leg (sciatica-like symptoms)
Stretching the piriformis muscle in a seated position may reproduce the pain and support the diagnosis.
Diagnosis
Diagnosis is primarily clinical, based on patient history and physical examination.
In cases where the diagnosis is unclear, additional tests may be required:
- MRI (Magnetic Resonance Imaging)
Helps identify the site of nerve compression - EMG (Electromyoneurography)
Used to assess nerve function and detect nerve compression or damage
Treatment
Treatment is usually conservative and focuses on relieving nerve compression and improving muscle function:
- Physical therapy and stretching exercises
- Activity modification (avoiding prolonged sitting)
- Pain management
In rare cases, more advanced interventions may be required.
9. Referred Pain from the Lumbar Spine and Sacroiliac Joint
Conditions affecting the lumbar spine can often present as pain in the posterior hip. Patients typically report lower back pain (low back pain) along with discomfort in the buttock or back of the hip. In many cases, a history of chronic or recurrent lower back pain is already present.
Pain may also extend into the pelvic region, making it more difficult to identify the true source.
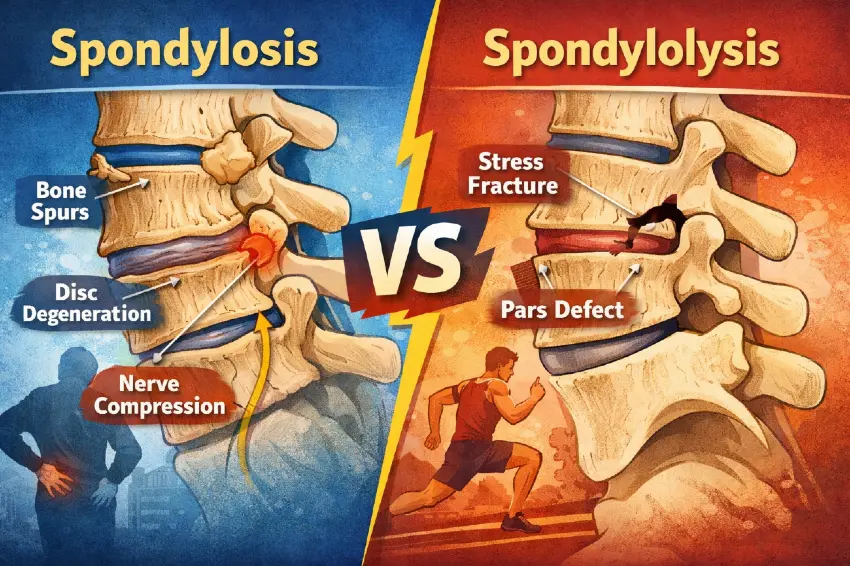
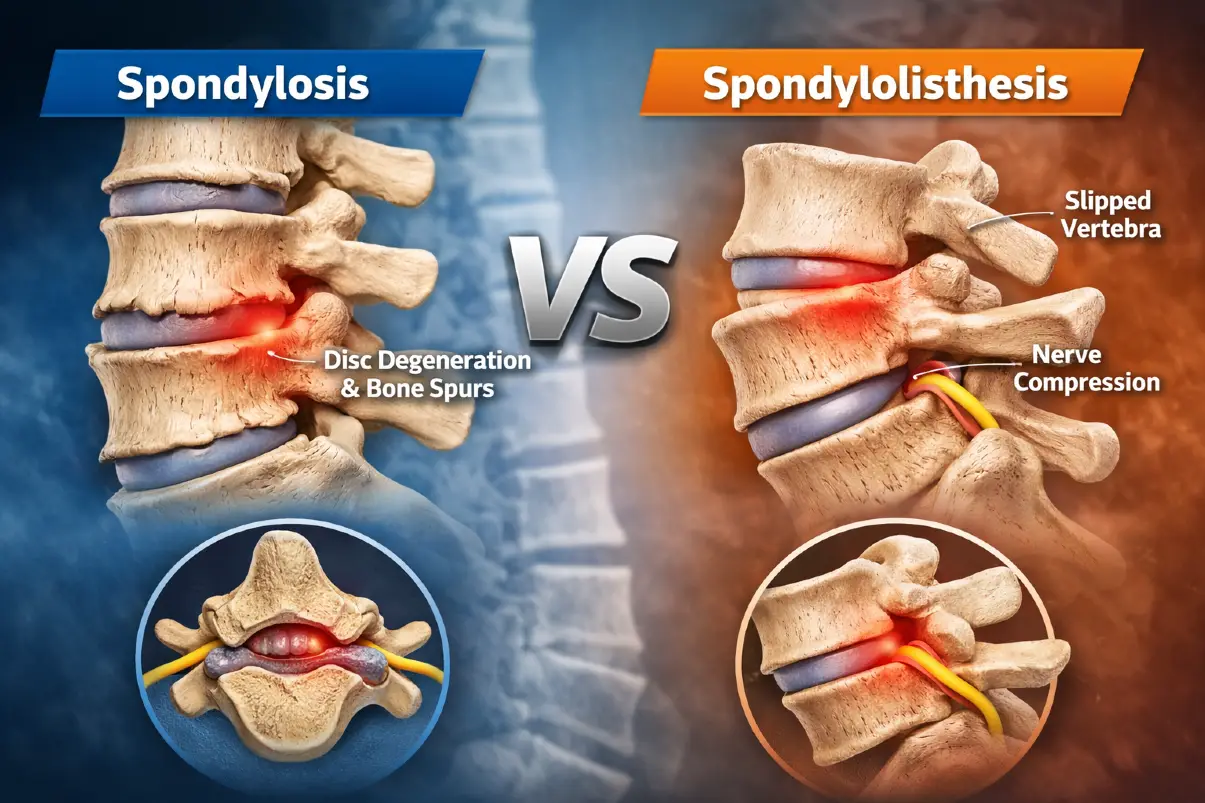
- X-ray of the lumbar spine
Often shows degenerative changes such as spondylosis, but provides limited information about the exact cause of pain - MRI (Magnetic Resonance Imaging)
More useful for identifying conditions such as disc herniation, nerve compression, spinal stenosis, or facet joint osteoarthritis
These conditions can cause pain that radiates into the gluteal region and posterior hip
Sacroiliac (SI) Joint Dysfunction
Dysfunction or arthritis of the sacroiliac joint is another common cause of posterior hip pain.
Typical findings include:
- Localized tenderness over the SI joint
- Positive provocation tests during physical examination
A key clinical point is that SI joint pain usually does not occur above the level of L5, which helps differentiate it from lumbar spine-related pain.
- X-ray may reveal signs of SI joint arthritis
- MRI can detect inflammation or early joint changes when the diagnosis is uncertain
10. Hamstring Injuries (Posterior Thigh Muscles)
Pain in the lower buttock, especially around the ischial tuberosity (sitting bone), may indicate a hamstring injury. This can include:
- Muscle strain
- Partial tear
- Complete tendon avulsion from its attachment
Hamstring injuries are often associated with:
- Sports-related trauma
- Sudden movements (e.g., sprinting)
- Overuse
A complete tear or avulsion typically presents with bruising on the back of the thigh and significant functional impairment.
In contrast, tendinopathy or partial tears usually cause:
- Pain during resisted hamstring contraction
- No visible bruising or deformity
Patients with suspected acute tears should be referred to an orthopedic specialist.
- MRI or ultrasound can be helpful when the diagnosis is unclear and to assess the extent of injury
How Is Hip Pain Treated?
If you are experiencing hip pain, it is important to consult a specialist—such as a physiatrist or orthopedic surgeon—to determine the exact cause. Once the diagnosis is established, treatment can be tailored to each patient.
In general, hip pain treatment can be divided into:
- Conservative (non-surgical) treatment
- Surgical treatment
Conservative Treatment (Non-Surgical)
In most cases, conservative treatment is the first-line approach. The goal is to reduce pain, maintain mobility, and prevent further joint damage.
Physical therapy plays a key role and may include:
- Targeted hip strengthening and mobility exercises
- Stretching and biomechanical correction
- Modalities such as ultrasound therapy, TENS, or shockwave therapy (for chronic tendinopathies)
Lifestyle modifications are also important:
- Reducing activities that aggravate pain
- Weight management to decrease joint load
- Choosing low-impact activities such as swimming or cycling
Medications may be used for symptom control:
- NSAIDs (e.g., Ibuprofen, Naproxen)
- Stronger pain relievers when necessary, under medical supervision
Injections may be considered when symptoms persist:
- Corticosteroid injections for inflammation
- Hyaluronic acid injections (viscosupplementation) in osteoarthritis
Regenerative therapies (in selected cases):
- PRP (platelet-rich plasma)
- Stem cell therapy
Assistive devices:
- Canes or crutches to reduce load on the hip
- Orthotic insoles for biomechanical correction
Surgical Treatment
Surgery is considered when conservative measures fail and symptoms significantly affect quality of life.
- Hip arthroscopy – minimally invasive procedure used to treat labral tears, impingement, and other intra-articular conditions
- Total hip replacement (THR) – indicated in advanced joint damage (e.g., severe osteoarthritis), providing pain relief and improved function
Prevention and Self-Care Tips
Maintaining hip health can significantly reduce the risk of pain:
Prevention and Self-Care for Hip Pain
- Maintain a healthy body weight – Reduces stress on the hip joint and lowers the risk of degeneration and pain.
- Stay physically active – Regular movement helps preserve joint mobility and overall hip function.
- Choose low-impact activities – Swimming and cycling strengthen muscles without excessive joint loading.
- Strengthen and stretch regularly – Focus on hip, gluteal, and core muscles to improve stability and flexibility.
- Improve posture and ergonomics – Proper sitting, standing, and lifting techniques reduce strain on the hip.
- Avoid prolonged sitting – Take regular breaks to move and prevent stiffness.
- Follow a balanced diet – Nutrient-rich foods support joint health and reduce inflammation risk.
Frequently Asked Questions (FAQ)
When should I see a doctor for hip pain?
Seek medical attention if:
- Pain lasts more than a few days despite rest
- Pain worsens with walking or disrupts sleep
- You experience stiffness or limited mobility
- There is swelling, redness, or inability to bear weight
Why does hip pain occur at night?
Night hip pain is commonly caused by:
- Trochanteric bursitis
- Hip osteoarthritis
- Piriformis syndrome
- Tendon inflammation
It may also be influenced by sleeping position or mattress quality. Using a pillow between the legs or changing sleep position may help reduce symptoms.
What causes a clicking or snapping sensation in the hip?
Clicking or snapping in the hip is usually caused by tendons moving over bony structures, such as:
- The iliotibial band over the greater trochanter
- The iliopsoas tendon over the pelvis
These sounds are often harmless if not associated with pain. However, in some cases, they may indicate labral or cartilage injury.
Wilson JJ, Furukawa M. Evaluation of the Patient with Hip Pain. Am Fam Physician. 2014 Jan 1;89(1):27-34. PMID: 24444505. https://www.aafp.org/pubs/afp/issues/2014/0101/p27.html
Reiman MP, Goode AP, Cook CE, Holmich P, Thorborg K, Martin HD. Diagnostic accuracy of clinical tests for the diagnosis of hip femoroacetabular impingement/labral tear: a systematic review. Br J Sports Med. 2015;49(12):811. doi: 10.1136/bjsports-2014-094302.
Nepple JJ, Prather H, Trousdale RT, Clohisy JC. Clinical diagnosis of femoroacetabular impingement. J Am Acad Orthop Surg. 2013;21 Suppl 1:S16–S19. doi: 10.5435/JAAOS-21-07-S16.
Lewis CL, Sahrmann SA. Acetabular labral tears. Phys Ther. 2006 Jan;86(1):110-21. doi: 10.1093/ptj/86.1.110.
Bali K, Sudesh P, Patel S, Kumar V, Saini U, Dhillon MS. Avascular necrosis of the femoral head: Etiology, pathogenesis, classification, and current treatment guidelines. Indian J Orthop. 2013;47(1):52–58. doi: 10.4103/0019-5413.106898. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3613526/
Mont MA, Cherian JJ, Sierra RJ, Jones LC, Lieberman JR. Nontraumatic Osteonecrosis of the Femoral Head: Where Do We Stand Today? J Bone Joint Surg Am. 2015;97(19):1604-1627. doi: 10.2106/JBJS.O.00071.
Bunker TD, Esler CNA, Leach WJ. Rotator-cuff tear of the hip. J Bone Joint Surg Br. 1997;79(4):618–620. doi: 10.1302/0301-620X.79B4.0790618.
Segal NA, Felson DT, Torner JC, et al. Greater trochanteric pain syndrome: epidemiology and associated factors. Arch Phys Med Rehabil. 2007 Aug;88(8):988-92. doi: 10.1016/j.apmr.2007.04.014.
Hopayian K, Song F, Riera R, Sambandan S. The clinical features of the piriformis syndrome: a systematic review. Eur Spine J. 2010 Dec;19(12):2095-109. doi: 10.1007/s00586-010-1504-9.
Vleeming A, Schuenke MD, Masi AT, Carreiro JE, Danneels L, Willard FH. The sacroiliac joint: an overview of its anatomy, function and potential clinical implications. J Anat. 2012;221(6):537-567. doi: 10.1111/j.1469-7580.2012.01564.x.
Brukner P, Khan K. Clinical Sports Medicine. 5th ed. McGraw-Hill Education; 2017.
American Academy of Orthopaedic Surgeons (AAOS) – Hip Conditions and Treatments









{kind=link}