

Spondylosis is a broad medical term used to describe degenerative changes of the spine. These changes include the gradual wear and tear of the intervertebral discs, the formation of bony growths (osteophytes), and a reduction in spinal mobility.
Spondylosis can affect any part of the spine—the cervical (neck), thoracic (mid-back), or lumbar (lower back) regions. While many people experience no significant symptoms, in some cases spondylosis can lead to back pain and stiffness. Tingling sensations or weakness in the arms or legs may occur if nerve compression develops, particularly in more advanced forms of the condition.
In this article, I will explain in more detail what spondylosis is, why it develops, whether it can be dangerous, and which symptoms it may cause.
What Is Spondylosis (Spondylosis Definition)
Spondylosis definition:
Spondylosis (from Greek spondylos – vertebra, and -osis – degenerative condition) is a broad term referring to degenerative changes affecting all structures of the spine, including the vertebrae, intervertebral discs, facet joints, and ligaments.
Most commonly, the term spondylosis is used to describe spinal osteoarthritis, but it is often applied more generally to any form of degenerative change of the spine.
Other Terms Used for Spondylosis
Medical terms that are commonly used as synonyms or closely related to spondylosis include:
- Degenerative spinal disease
- Degenerative changes of the spine
- Spinal osteoarthritis
- Spinal osteochondrosis
- Spinal arthrosis
- Spondyloarthrosis
- Degenerative spondylopathy
- Vertebral arthrosis
Spondylosis is considered a natural aging process and occurs in the majority of people after the age of 50. Due to the structure and mechanical demands of the spine, degenerative changes most commonly affect the lumbar spine (lumbar spondylosis) and the cervical spine (cervical spondylosis).
How Do Degenerative Changes of the Spine Manifest?
As mentioned earlier, degenerative changes associated with spondylosis can involve any spinal structure.
Below is an overview of the main pathological processes that occur in different parts of the spine in spondylosis, along with definitions of key related terms.
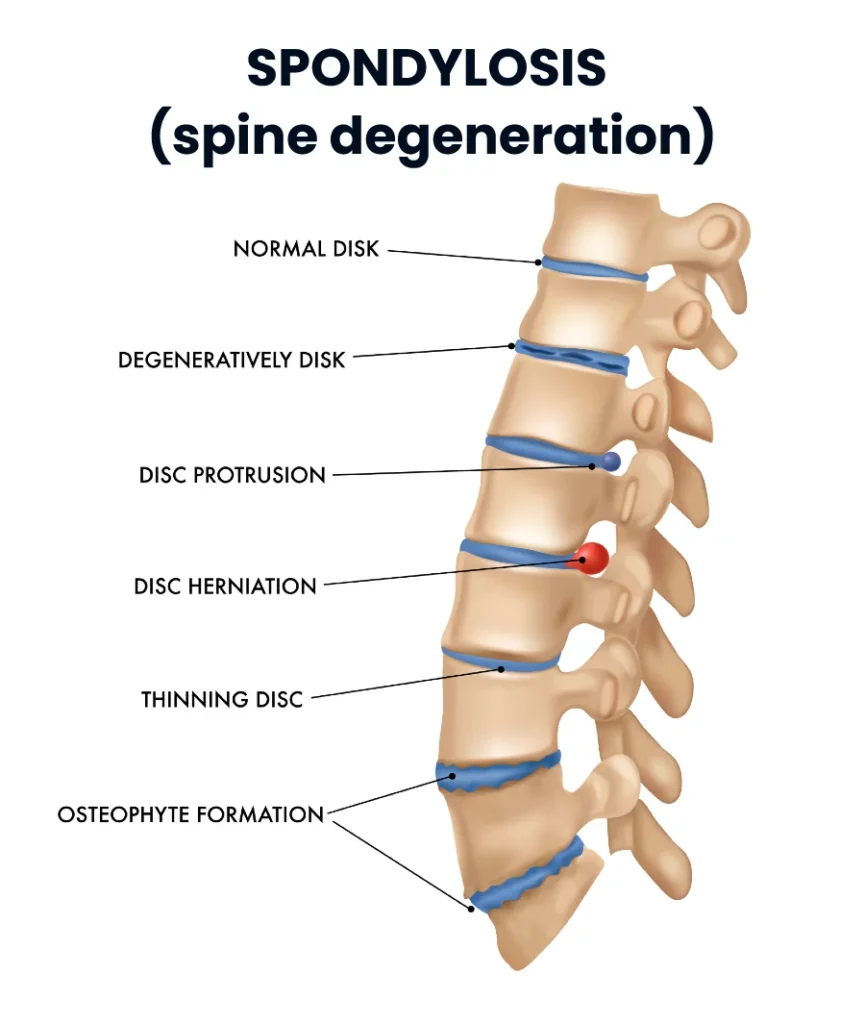
Osteophytes (Spondylophytes)
Osteophytes are bony outgrowths that form along the edges of vertebral bodies as a response to chronic mechanical stress and loss of spinal stability, usually resulting from degeneration of the intervertebral discs and facet joints.
Although osteophytes are often asymptomatic, their enlargement may lead to narrowing of the spinal canal or intervertebral foramina, potentially causing neurological symptoms due to nerve compression.
Degenerative Disc Disease
Degenerative disc disease refers to progressive structural changes of the intervertebral discs caused by aging and mechanical loading. These changes include:
- Loss of water content in the disc nucleus
- Reduction in disc height
- Development of fissures in the outer disc ring
As a result, disc degeneration may lead to disc herniation, reduced space between adjacent vertebrae, and segmental mechanical instability.
Facet Joint Osteoarthritis (Spondyloarthrosis)
Facet joints are paired joints located at the back of the spine and are structurally similar to other synovial joints in the body. Degenerative changes of these joints include:
- Thinning of the articular cartilage
- Formation of osteophytes
- Thickening of the joint capsule
These changes can contribute to spinal stiffness, pain, and reduced mobility.
Spondylosis of the Spine – Summary
In conclusion, spondylosis refers to degenerative processes affecting the spine, characterized by:
- Formation of osteophytes
- Degeneration of intervertebral discs
- Osteoarthritis of the facet joints
- Thickening of spinal ligaments
Together, these changes may alter spinal biomechanics and, in some cases, lead to pain, stiffness, or neurological symptoms.
Why Does Spondylosis Develop?
Spondylosis, or degenerative changes of the spine, develops gradually over many years as a result of the natural aging process and biomechanical loading of the spine. It is widely believed that the entire process of spondylosis begins with intervertebral disc degeneration and then progresses through several overlapping stages. This sequence of events is known as the degenerative cascade.
Over time, the intervertebral discs lose their elasticity, small fissures develop, nutrient diffusion decreases, and the discs gradually dehydrate and lose height. As disc degeneration progresses, disc herniation (disc protrusion) may occur.
Loss of normal disc function leads to increased compressive forces on the vertebral bodies, which promotes the formation of bony outgrowths (osteophytes). In addition, disc degeneration results in reduced segmental stability, increasing mechanical stress on the facet joints. As a consequence, degenerative changes of the facet joints (facet joint osteoarthritis) also develop.
It is believed that excessive osteophyte formation, facet joint osteoarthritis, and ligament thickening represent the spine’s adaptive response to instability caused by disc degeneration and dysfunction.
How Common Is Spondylosis?
Spondylosis is a very common condition, especially among older adults. Studies show that approximately 85% of people over the age of 50 exhibit signs of lumbar or cervical spondylosis. Around half of individuals in their 40s show some features of spondylosis on spinal imaging. In contrast, spondylosis is relatively rare in younger adults aged 20–30, affecting about 10% of cervical spines and roughly 5% of lumbar spines.
From these data, it is clear that spondylosis is more the rule than the exception in people over 50.
Risk Factors for Developing Spondylosis
While spondylosis develops to some degree in virtually all older adults, certain factors can accelerate or slow its progression.
- Age: The prevalence of spondylosis increases with age. However, not all individuals of the same age exhibit the same degree of spinal degeneration.
- Body weight (obesity): Research shows a clear association between increased body weight and the development of lumbar spondylosis. Interestingly, no significant link has been found between obesity and cervical spondylosis.
- Occupation and spinal loading: Some experts suggest that jobs involving heavy lifting, frequent bending, twisting, or prolonged awkward postures may contribute to spinal degeneration. Others, however, dispute any strong connection. If such a link exists, it appears to be relatively weak.
- Genetics and heredity: Genetics plays a significant role in the development of spondylosis. Studies of identical twins show a high similarity in spinal degeneration patterns. Additionally, if your parents have significant spondylosis, your risk is higher.
Summary
Spondylosis can be viewed as a natural and inevitable part of aging. Its development depends on genetic predisposition and environmental factors, such as body weight and spinal stress, affecting each individual to varying degrees.
Symptoms of Spondylosis
Before diving into the details, it’s important to answer a crucial question:
Does every case of spondylosis cause pain?
Fortunately, the answer is no. Most people with spinal spondylosis experience no symptoms at all. Patients who have signs of spondylosis on imaging should not automatically assume that these degenerative changes are the cause of their pain. Spinal degeneration is a natural part of aging, and any pain a patient feels may or may not be related to these changes.
When symptoms do occur, they generally present in one of four ways:
- Neck pain or lower back pain
- Cervical or lumbar radiculopathy
- Cervical myelopathy
- Spinal canal stenosis (neurogenic claudication)
1. Neck pain or lower back pain
The most common symptom of spondylosis is pain in the neck and/or lower back. This pain usually appears during physical activity or after prolonged standing, sitting, or poor posture, and it often improves with rest.
In the neck, it manifests as stiffness and reduced mobility, while in the lumbar spine it appears as localized lower back pain, sometimes radiating to the buttocks or thigh. In most cases, this pain is not caused by nerve damage but by changes in the static and dynamic stability of the spine.
2. Radiculopathy
Radiculopathy occurs when the nerve roots emerging from the cervical or lumbar spine are compressed or irritated. It is less common than neck or lower back pain.
In younger patients, typically in their 30s and 40s, the most frequent cause is a herniated disc, which presses on the nerve. As people age, degenerative changes become the main cause: disc degeneration is the leading cause in the 50s and 60s, while in the 70s, osteophytes or spondylophytes narrowing the nerve exits are usually responsible.
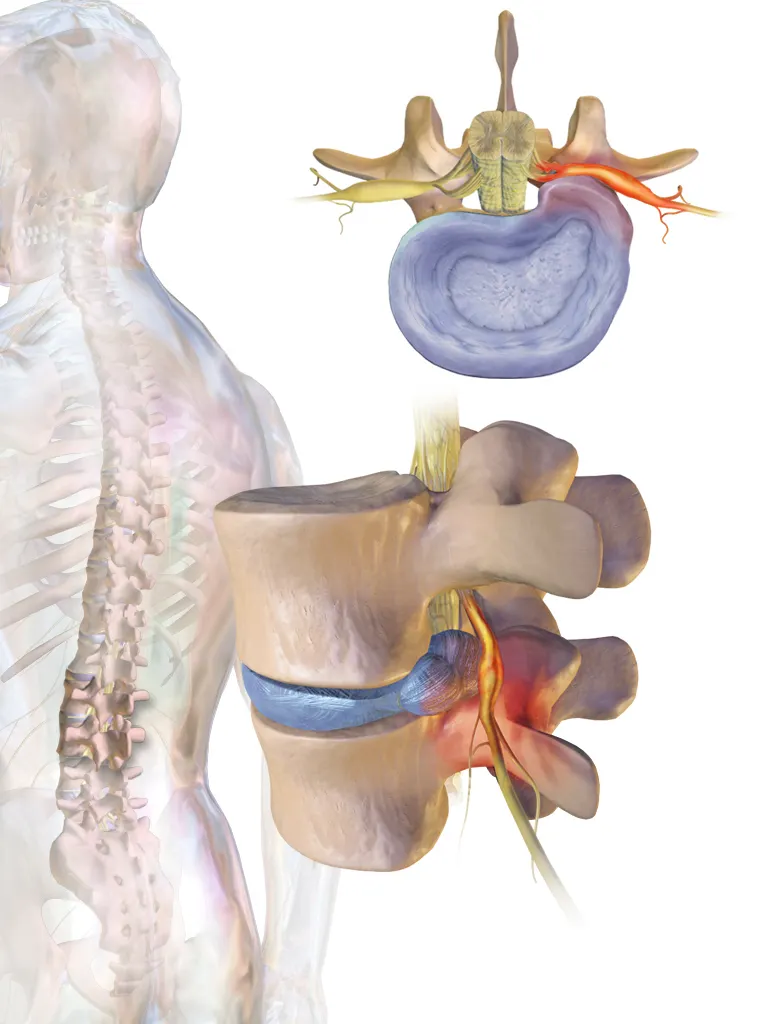
Common symptoms of cervical radiculopathy include pain radiating from the neck to the shoulder, arm, or hand, tingling in the hands, and weakness or numbness in the affected areas. Pain may worsen with neck movements, especially rotation or bending, and can persist throughout the day.
In the lumbar spine, nerve compression is commonly referred to as sciatica. The main symptom is lower back pain radiating down the leg, often reaching the foot.
3. Cervical spondylosis with myelopathy
Herniated intervertebral discs, thickened spinal ligaments, hypertrophic facet joints, and osteophytes can narrow the spinal canal and compress the cervical spinal cord. This condition is called cervical myelopathy.
Cervical myelopathy often develops gradually and may or may not include neck pain at the onset. Early symptoms can be subtle, such as hand weakness or difficulty performing fine motor tasks, like buttoning a shirt, tying shoelaces, or picking up small objects. Patients may also report gait instability or unexplained falls.
Urinary symptoms, such as incontinence, are rare in the early stages and usually appear only in advanced cases. This progressive compression of the spinal cord requires timely recognition and treatment to prevent permanent neurological damage.
4. Lumbar spinal canal stenosis and neurogenic claudication
Lumbar spinal canal stenosis occurs when the spinal canal narrows, compressing the nerve roots on their way to the legs. This narrowing can result from degenerative changes, including osteophytes, ligament thickening, or herniated discs.

One of the key symptoms is neurogenic claudication — pain, weakness, numbness, or tingling in the legs that worsens with walking or standing and improves when sitting or leaning forward. Lumbar spinal stenosis is generally a sign of advanced spondylosis, most commonly seen in individuals over 75 years of age.
How Is Spondylosis Diagnosed?
Spondylosis can be detected through spinal imaging such as X-rays, magnetic resonance imaging (MRI), and computed tomography (CT) scans. A typical X-ray report may describe osteophytes (bony growths), narrowing of intervertebral spaces, sclerosis of the vertebral endplates, facet joint degeneration, and soft tissue calcifications. The extent of degenerative changes seen on imaging does not necessarily correlate with a patient’s symptoms. Some patients with minimal changes may experience severe pain, while others with significant spondylosis may have no symptoms at all.
MRI is the most reliable method for visualizing nerve structures and soft tissues. It provides a detailed view of nerve or spinal cord compression and can detect pathological changes such as disc herniations, osteophytes, or ligament hypertrophy. However, because degenerative changes are often present in asymptomatic individuals, MRI is typically reserved for clinically indicated cases.
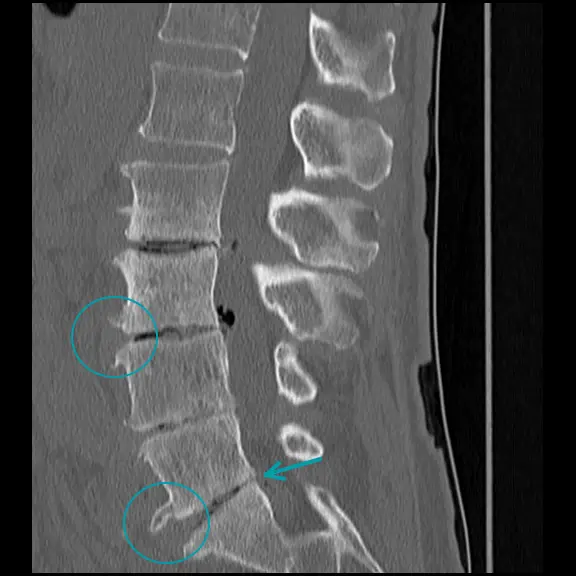

CT scans provide detailed imaging of bony structures and are superior to X-rays for evaluating foraminal stenosis, especially when hypertrophy of the facet or uncovertebral joints is present. CT is less effective than MRI for visualizing soft tissues and nerve structures.
Multilevel Spondylosis
Multilevel spondylosis refers to degenerative changes affecting more than one segment of the spine. This condition is common, especially in older adults, and may involve multiple cervical, thoracic, or lumbar vertebrae.
In multilevel spondylosis, the spine may show a combination of:
- Disc degeneration at several levels
- Osteophyte formation along multiple vertebrae
- Facet joint osteoarthritis across multiple segments
- Ligament thickening in several areas
Because multiple segments are affected, patients may experience more widespread pain, stiffness, or neurological symptoms compared to single-level spondylosis. For example, nerve compression at several levels in the cervical spine can lead to arm weakness, numbness, or fine motor difficulties, while lumbar involvement can result in sciatica affecting multiple nerve roots.
Is Spondylosis Dangerous?
In most cases, spondylosis is not a cause for concern. As mentioned earlier, it is a normal part of aging and occurs in almost all older adults. Most people with spondylosis do not experience symptoms. Spondylosis becomes clinically significant only if it leads to spinal canal stenosis in the cervical or lumbar regions and compresses neurological structures (spinal cord or nerves).
How Is Spondylosis Treated?
If a person shows signs of spondylosis on imaging but has no symptoms, treatment is generally not required.
Neck pain or lower back pain without radiation into the arms or legs is usually not caused by nerve irritation or damage and is typically managed with conservative methods, including:
- Pain-relieving medications
- Physical therapy
- Regular exercise
If radiculopathy or myelopathy symptoms are present, further diagnostic evaluation (MRI) is required to determine the location and severity of nerve compression. In most cases, treatment initially remains conservative. If symptoms persist after several weeks or 2–3 months of treatment, or if signs of neurological damage appear, surgical intervention may be considered.
Kuo DT, Tadi P. Cervical Spondylosis. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551557/
https://www.spine-health.com/conditions/lower-back-pain/spondylosis-what-it-actually-means
Middleton K, Fish DE. Lumbar spondylosis: clinical presentation and treatment approaches. Curr Rev Musculoskelet Med. 2009 Jun;2(2):94-104. doi: 10.1007/s12178-009-9051-x. Epub 2009 Mar 25. PMID: 19468872; PMCID: PMC2697338.
Sheng B, Feng C, Zhang D, Spitler H, Shi L. Associations between Obesity and Spinal Diseases: A Medical Expenditure Panel Study Analysis. Int J Environ Res Public Health. 2017 Feb 13;14(2):183. doi: 10.3390/ijerph14020183. PMID: 28208824; PMCID: PMC5334737.

















