

Carpal tunnel syndrome is the most common nerve compression condition in the human body. It occurs when the median nerve becomes compressed as it passes through the carpal tunnel in the wrist—a narrow passageway made of bones and ligaments. This condition accounts for nearly 90% of all compressive neuropathies.
Most often, it affects people between the ages of 40 and 60, and women are up to ten times more likely to develop it than men. The condition causes pain, numbness, and tingling—especially in the thumb, index, and middle fingers. These symptoms typically worsen at night and can disrupt sleep and daily activities. If left untreated, it may lead to permanent nerve damage and long-term functional limitations.
In this article, you’ll learn what carpal tunnel syndrome is, what causes it, how to recognize the symptoms, what treatment options are available, and what steps you can take to help prevent it.
Carpal Tunnel Anatomy and the Role of the Median Nerve
Understanding the Structure of the Carpal Tunnel
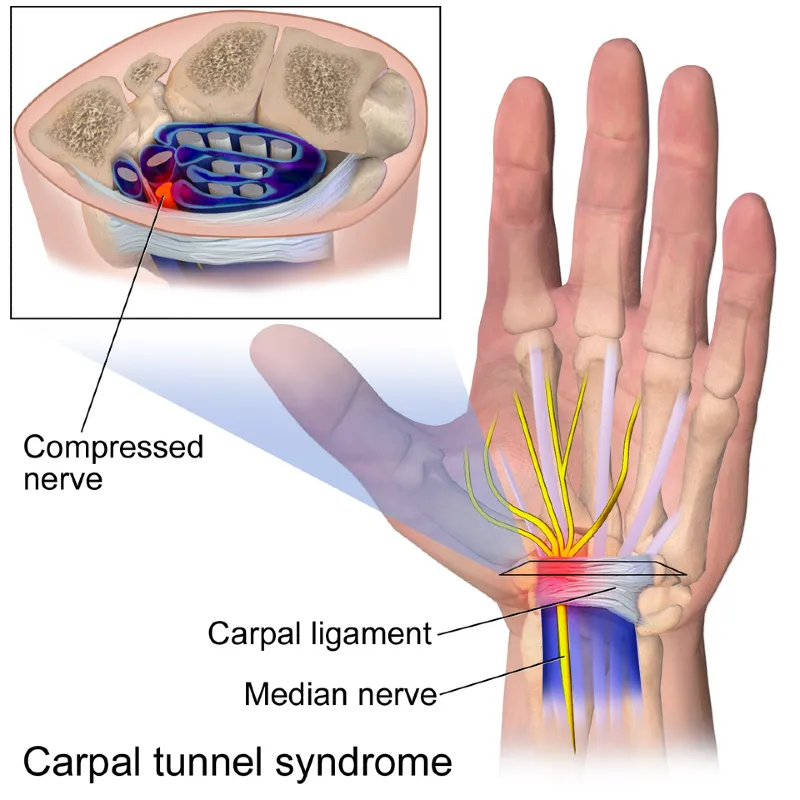
Before we dive deeper into carpal tunnel syndrome, it’s important to understand what the carpal tunnel actually is. The carpal tunnel is a narrow passageway located in the wrist. It serves as a protected corridor through which the median nerve and the flexor tendons (responsible for finger movement) pass.
The floor and sides of the tunnel are formed by the carpal bones, while the roof is made up of a tough connective tissue called the transverse carpal ligament. During surgical treatment for carpal tunnel syndrome, this ligament is usually the one that is cut to relieve pressure on the nerve.
The Function of the Median Nerve
The median nerve plays a crucial role in hand function. It carries sensory information from the thumb side of the palm and from the thumb, index finger, middle finger, and part of the ring finger. It also powers several muscles in the hand, particularly those at the base of the thumb, which are essential for grip and fine motor control.
When this nerve is compressed inside the carpal tunnel, it can no longer function properly—leading to pain, tingling, and loss of hand strength.
Why Does Carpal Tunnel Syndrome Occur?
The carpal tunnel is a narrow, rigid passage in the wrist. Because it’s surrounded by bones and a tough ligament, it has little room to stretch or expand. Inside this tunnel run both the median nerve and the flexor tendons that control your fingers. That means there’s not much extra space—so even a small increase in pressure can lead to problems.
Under normal circumstances, the median nerve passes through the carpal tunnel without any issues. But when something reduces the available space or increases the contents of the tunnel, pressure builds up. This pressure disrupts the nerve’s blood supply, causing it to swell and function poorly—just like stepping on a garden hose cuts off water flow.
Common Causes of Increased Pressure in the Carpal Tunnel
Several different factors can contribute to increased pressure on the median nerve:
- Poorly healed wrist fractures can alter the shape of the tunnel, reducing space.
- Advanced degenerative changes (like osteoarthritis) can produce bony overgrowths (osteophytes) that compress the nerve.
- Inflammatory arthritis, especially rheumatoid arthritis, can cause swelling of the joint and tendons within the tunnel.
- Fluid retention due to obesity, diabetes, or thyroid dysfunction can increase tissue volume and pressure.
- Hormonal changes, especially during pregnancy or menopause, can lead to swelling in the wrist.
- Repetitive wrist movements, such as typing or operating vibrating machinery, can strain tissues and increase swelling.
- Vibration exposure, such as from power tools, may damage the small blood vessels supplying the nerve.
- Cysts or tumors, though rare, can physically occupy space in the tunnel and compress the nerve.
Often, more than one factor is involved—making the condition complex and sometimes tricky to diagnose.
Symptoms of Carpal Tunnel Syndrome
One of the earliest and most common signs of carpal tunnel syndrome is tingling, numbness, or burning pain in the thumb, index finger, middle finger, and half of the ring finger. These symptoms often appear at night and can be intense enough to wake you from sleep. Many people instinctively shake or flick their hands in an attempt to relieve the discomfort.
As the condition progresses, symptoms begin to show up during the day—especially during activities that involve repetitive wrist motions, like typing, driving, or holding a phone. With time, the nerve damage may worsen, and new symptoms can appear.
More Advanced Signs
- Weakness in the hand or fingers: Patients may notice difficulty gripping objects or find themselves dropping things.
- Clumsiness: Fine motor tasks like buttoning a shirt or using small tools can become challenging.
- A feeling of swelling in the fingers or palm, even though no swelling is actually present.
- Muscle wasting, especially at the base of the thumb (thenar muscle), may develop in later stages.
- Permanent numbness: If left untreated, long-term compression can lead to irreversible loss of sensation in the fingers.
Early recognition of these symptoms is key. With timely diagnosis and proper treatment, most people can avoid permanent nerve damage and regain normal hand function.
Want to learn more?
If you want a deep dive into the most common conditions that cause hand tingling and numbness, check out our full article:
“Hand Tingling: 7 Common Causes and How to Recognize Them” — where we explore key causes, symptoms to watch for, and the best steps to take for relief.
Carpal Tunnel Syndrome Differential Diagnosis? Conditions That Can Mimic CTS
Carpal tunnel syndrome (CTS) typically causes symptoms in the hand, such as tingling, numbness, and pain in the thumb, index, and middle fingers. However, in some cases, pain may radiate up the arm toward the elbow, leading to confusion with other conditions. That’s why carpal tunnel syndrome differential diagnosis is essential—to avoid misdiagnosis and ensure proper treatment.
Below are some of the most common conditions that can mimic carpal tunnel syndrome:
Cervical Spine Disorders and Radiculopathy
Degenerative changes or herniated discs in the cervical spine can compress nerve roots—most commonly C6 and C7—leading to symptoms that closely mimic carpal tunnel syndrome. This condition, known as cervical radiculopathy, may cause radiating pain, tingling, numbness, or weakness that starts in the neck and travels down the arm into the hand. Unlike CTS, symptoms often affect the entire arm, not just the thumb, index, and middle fingers, and they typically worsen with certain neck movements.
Myofascial Pain Syndrome
Trigger points in the neck, shoulders, or upper back—especially in the scalene or trapezius muscles—can refer pain to the hand and mimic nerve entrapment. These muscular causes often lack true numbness and instead cause deep, aching discomfort.
Tendon-Related Conditions
Inflammatory or degenerative conditions affecting tendons in the wrist and hand can resemble CTS:
- De Quervain’s tenosynovitis causes pain on the thumb side of the wrist, especially with grasping or twisting motions.
- Thumb joint arthritis (rhizarthrosis) can also lead to hand pain and reduced grip strength, particularly at the base of the thumb.
Takeaway: If symptoms extend beyond the hand, affect both arms, or are accompanied by neck or shoulder pain, it’s crucial to consider other causes. A thorough clinical evaluation—including neurological and orthopedic assessment—is the key to identifying the right diagnosis and avoiding unnecessary treatments.
How Is Carpal Tunnel Syndrome Diagnosed?
If you suspect carpal tunnel syndrome, it’s important to consult a doctor early to ensure a correct diagnosis and begin proper treatment. The diagnosis is based on a detailed review of your symptoms, a physical examination, and specific diagnostic tests. Blood tests are not helpful in diagnosing carpal tunnel syndrome.
Clinical Examination: Are There Carpal Tunnel Syndrome Tests?
Yes — several clinical tests are commonly used during a physical exam to help confirm the diagnosis:
- Tinel’s Sign: Light tapping over the median nerve at the wrist may reproduce tingling sensations in the hand.
- Phalen’s Test: Pressing the backs of the hands together with wrists flexed for 30 to 60 seconds can trigger tingling in the affected fingers.
- Durkan’s Compression Test: Applying direct pressure over the carpal tunnel just below the wrist crease. If tingling or numbness appears within 30 seconds, the test is considered positive.
Ultrasound: A Quick and Accessible Imaging Option
Ultrasound is a fast, non-invasive imaging test that allows doctors to assess the structure of the median nerve. It can reveal swelling, thickening, or entrapment, as well as limited nerve mobility caused by adhesions to the transverse carpal ligament.

EMG/NCS (Electromyography and Nerve Conduction Studies)
EMG, often combined with nerve conduction velocity (NCV) testing, measures the electrical function of the median nerve and the muscles it controls. This test is considered essential in confirming the diagnosis and grading the severity of nerve damage. It helps differentiate CTS from other conditions and guides the choice between conservative or surgical treatment.
Carpal Tunnel Syndrome Treatment Options
Treatment for carpal tunnel syndrome depends on the severity of the nerve compression and each patient’s individual needs. In general, there are two main approaches:
- Conservative (non-surgical) treatment
- Surgical treatment
Conservative Treatment Options
Conservative therapies are recommended as the first-line treatment in cases where there is no significant nerve damage.
Preventive Measures
Doctors often recommend ergonomic adjustments to reduce stress on the wrist. These include proper hand positioning during work, especially while typing. Adjusting keyboard height and using soft gel pads for the mouse can reduce wrist strain. Reducing repetitive hand movements and addressing underlying health factors such as obesity, diabetes, or thyroid disorders is also beneficial. Increasing physical activity and maintaining a healthy weight can support overall nerve health.
Brace for Caral Tunnel Syndrome
Wrist splints or braces are commonly used during the early stages of carpal tunnel syndrome, especially if symptoms occur primarily at night. These braces keep the wrist in a neutral position during sleep, minimizing compression on the median nerve. While splints may not provide immediate relief, consistent use over several weeks can significantly reduce pain and tingling, improving sleep and quality of life.
Physical Therapy and Exercises
Physical therapy includes treatments like laser therapy, therapeutic ultrasound, magnet therapy, and electrical stimulation aimed directly at the carpal tunnel. Therapy often includes nerve-gliding exercises and stretching routines to increase wrist mobility and decrease pressure on the nerve. Some patients benefit from targeted exercises to help the nerve glide more freely within the tunnel.
Corticosteroid Injections
Corticosteroid injections are an effective non-surgical treatment, especially when guided by ultrasound. These injections reduce inflammation and swelling in the median nerve, easing symptoms.
- In early stages, a single injection can provide long-term relief.
- In moderate to severe cases, the relief may be temporary — typically lasting up to a year, sometimes longer.
- Injections may be safely repeated up to three times per year if needed.
When Is Carpal Tunnel Syndrome Surgery Needed?
Surgical treatment is considered when conservative options fail or in cases of advanced nerve damage. The procedure — known as carpal tunnel release surgery — is usually performed by a plastic surgeon or hand specialist.
The goal of the operation is to cut the transverse carpal ligament, increasing the space in the tunnel and reducing pressure on the nerve. This is typically an outpatient procedure and can be performed under either local or general anesthesia.
There are two main surgical techniques:
Open Surgery
The surgeon makes a small incision on the palm to access and cut the transverse ligament. This method allows a direct view of the structures involved and is widely used.
Endoscopic Surgery
In this minimally invasive method, one or two tiny incisions (portals) are made to insert a small camera and specialized instruments. The ligament is cut from the inside under visual guidance.
Both approaches are considered effective, and studies show no significant difference in success rates. Over 90% of patients experience relief after surgery. However, up to one-third may see symptoms return within a few years, especially if underlying risk factors remain unaddressed.
Carpal Tunnel Surgery Recovery
Recovery after carpal tunnel release surgery can vary depending on several individual factors, such as the extent of the procedure, overall health status, and how well a patient follows post-operative instructions. In general, the recovery period ranges from a few weeks to several months.
Early Recovery (First Few Days)
During the initial days after surgery, patients typically experience pain, swelling, and limited mobility in the affected hand. To manage these symptoms:
- Apply cold compresses regularly.
- Keep the hand elevated to reduce swelling and discomfort.
- Use pain medications as prescribed by the doctor.
Weeks 2–3: Gradual Return of Function
About two to three weeks after surgery, most patients begin physical therapy. This includes gentle exercises to:
- Strengthen the muscles of the hand and wrist
- Restore range of motion
- Prevent stiffness and improve coordination
At this stage, it’s important to avoid heavy lifting or repetitive hand movements that could strain the healing tissues.
Long-Term Recovery
Over time, most patients notice a significant reduction in symptoms, including tingling, numbness, and pain. Grip strength and hand function gradually return, although full recovery may take several months, especially in cases of long-standing nerve compression.
While many patients can resume light activities within a few weeks, returning to work that involves manual labor may take longer. Following your doctor’s and physical therapist’s recommendations is essential for a smooth and successful recovery.
Frequently Asked Questions (FAQ)
1. Is Carpal Tunnel Permanent
Carpal tunnel syndrome isn’t always permanent, especially if treated early. In mild to moderate cases, symptoms can improve with rest, splinting, and lifestyle changes. However, if the pressure on the median nerve continues over time without treatment, it can lead to permanent nerve damage, weakness, and muscle loss in the hand. That’s why early diagnosis and treatment are crucial.
2. Home Remedies for Carpal Tunnel
Several home remedies for carpal tunnel can reduce symptoms. Wearing a wrist splint at night helps prevent nerve compression. Applying cold packs reduces inflammation, while gentle wrist stretches and taking breaks from repetitive hand activities can ease pressure on the nerve. Anti-inflammatory foods and avoiding activities that aggravate symptoms can also support recovery.
3. Can Carpal Tunnel Cause Arm Pain
Yes, carpal tunnel can cause arm pain. While the condition primarily affects the wrist and hand, pain can radiate up the forearm and sometimes even into the upper arm or shoulder. This happens when the median nerve becomes compressed and irritated. However, if arm pain is severe or persistent, it’s important to rule out other conditions like cervical radiculopathy.
4. How Do U Know If You Have Carpal Tunnel
You might have carpal tunnel if you experience numbness, tingling, or pain in your thumb, index, middle finger, or half of your ring finger — especially at night. You may drop objects more often or feel weakness in your grip. These symptoms typically worsen with repetitive wrist movements. A clinical exam and nerve conduction tests can confirm the diagnosis.
5. Why Is Carpal Tunnel Worse at Night
Carpal tunnel is often worse at night because of wrist position during sleep. Many people sleep with their wrists flexed, which increases pressure inside the carpal tunnel and compresses the median nerve. Additionally, reduced movement and distractions at night make tingling and pain more noticeable.
6. How to Relieve Carpal Tunnel Pain at Night
To relieve carpal tunnel pain at night, wear a wrist splint to keep the wrist in a neutral position. Avoid sleeping with your hands under your head or bent. Elevate your arm on a pillow and use cold packs to reduce swelling. If symptoms persist, consult a healthcare provider for treatment options like physical therapy or steroid injections.
7. When Is Carpal Tunnel Bad Enough for Surgery
Carpal tunnel may be bad enough for surgery if conservative treatments fail after several months, or if you develop persistent numbness, hand weakness, or muscle wasting. Surgery is typically recommended when nerve tests show significant slowing or damage to the median nerve, indicating the condition is progressing despite non-surgical treatments.
8. Will Carpal Tunnel Heal on Its Own
Carpal tunnel will not always heal on its own. In very mild or early cases, symptoms may improve with rest, ergonomic changes, and night splinting. However, if the underlying cause of compression persists, the condition can worsen over time. Untreated, it may lead to permanent nerve damage — so early intervention is key.
Sevy JO, Sina RE, Varacallo MA. Carpal Tunnel Syndrome. [Updated 2023 Oct 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448179/
Joshi A, Patel K, Mohamed A, Oak S, Zhang MH, Hsiung H, Zhang A, Patel UK. Carpal Tunnel Syndrome: Pathophysiology and Comprehensive Guidelines for Clinical Evaluation and Treatment. Cureus. 2022 Jul 20;14(7):e27053. doi: 10.7759/cureus.27053. PMID: 36000134; PMCID: PMC9389835. https://www.cureus.com/articles/93509-carpal-tunnel-syndrome-pathophysiology-and-comprehensive-guidelines-for-clinical-evaluation-and-treatment#!/
Keith MW, Masear V, Chung K, Maupin K, Andary M, Amadio PC, Barth RW, Watters WC 3rd, Goldberg MJ, Haralson RH 3rd, Turkelson CM, Wies JL. Diagnosis of carpal tunnel syndrome. J Am Acad Orthop Surg. 2009 Jun;17(6):389-96. doi: 10.5435/00124635-200906000-00007. PMID: 19474448; PMCID: PMC5175465.
Wielemborek PT, Kapica-Topczewska K, Pogorzelski R, Bartoszuk A, Kochanowicz J, Kułakowska A. Carpal tunnel syndrome conservative treatment: a literature review. Postep Psychiatr Neurol. 2022 Jun;31(2):85-94. doi: 10.5114/ppn.2022.116880. Epub 2022 May 31. PMID: 37082094; PMCID: PMC9881572. https://doi.org/10.5114/ppn.2022.116880
Klokkari D, Mamais I. Effectiveness of surgical versus conservative treatment for carpal tunnel syndrome: A systematic review, meta-analysis and qualitative analysis. Hong Kong Physiother J. 2018 Dec;38(2):91-114. doi: 10.1142/S1013702518500087. Epub 2018 Jul 2. PMID: 30930582; PMCID: PMC6405353.
Karjalanen T, Raatikainen S, Jaatinen K, Lusa V. Update on Efficacy of Conservative Treatments for Carpal Tunnel Syndrome. J Clin Med. 2022 Feb 11;11(4):950. doi: 10.3390/jcm11040950. PMID: 35207222; PMCID: PMC8877380. https://www.mdpi.com/2077-0383/11/4/950
Alrayes MS, Altawili M, Alsaffar MH, Alfarhan GZ, Owedah RJ, Bodal IS, Alshahrani NAA, Assiri AAM, Sindi AW. Surgical Interventions for the Management of Carpal Tunnel Syndrome: A Narrative Review. Cureus. 2024 Mar 5;16(3):e55593. doi: 10.7759/cureus.55593. PMID: 38576667; PMCID: PMC10994685.
Karpalni kanal: Najčešće mjesto kompresije živca (Fizijatar.hr)
Injekcije za sindrom karpalnog kanala: Može li se izbjeći operacija? (Fizijatar.hr)

















