
Knee pain can be confusing, especially when it comes from an injury. Two of the most common and often confused knee injuries are a meniscal tear and an ACL (anterior cruciate ligament) tear. Both can happen suddenly, often during sports or twisting movements, and both can cause swelling, discomfort, and difficulty walking. But despite some similarities, these injuries affect completely different structures in the knee — and require different treatments and recovery plans.
In this article, we’ll break down the key differences between a meniscal tear vs ACL tear — from symptoms and diagnosis to treatment options and recovery timelines. Whether you’ve recently injured your knee or are just trying to understand what might be going on, knowing the distinction is a crucial step toward proper care and long-term knee joint health.
What Is the Meniscus, and What Is the ACL?
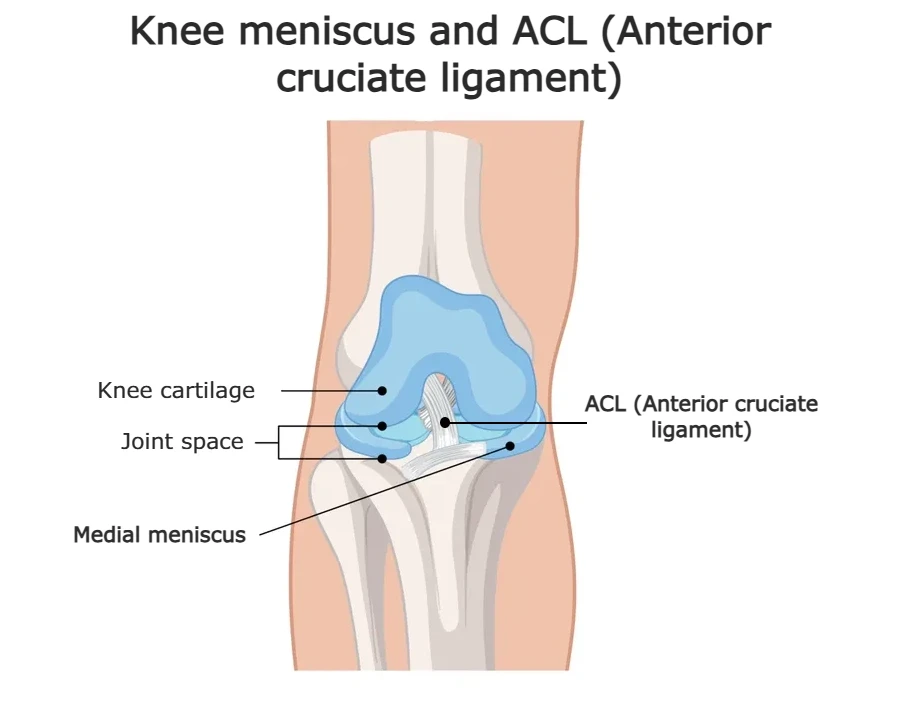
The meniscus and the anterior cruciate ligament (ACL) are two important structures inside the knee, but they serve very different roles.
Meniscus: Shock Absorber of the Knee
The meniscus is a crescent-shaped piece of cartilage located between the femur (thigh bone) and tibia (shin bone). Each knee has two menisci — the medial meniscus on the inner side and the lateral meniscus on the outer side.
Their job is to:
- Absorb shock during walking, running, or jumping
- Distribute body weight evenly across the joint
- Reduce friction between the bones
- Protect the cartilage and stabilize movement
Menisci are made of tough, rubbery fibrocartilage — strong enough to handle pressure, but not invincible.
ACL: The Knee’s Main Stabilizing Ligament
The ACL (anterior cruciate ligament) is one of the four major ligaments in the knee. It runs diagonally through the center of the knee, connecting the femur to the tibia.
Its main roles are to:
- Keep the knee stable during rotation or side-to-side movements
- Prevent the tibia from sliding too far forward under the femur
- Control knee alignment during movement and impact
Meniscal Tear vs ACL Tear: How Do These Injuries Happen?
Meniscal and ACL tears often share a similar injury mechanism — a sudden twist, pivot, or awkward landing during sports or daily activity. Because both structures help stabilize the knee, it’s not uncommon for them to be injured at the same time. In fact, this combination is well known in sports medicine as the “unhappy triad” (also called the terrible triad) — involving injury to the ACL, medial meniscus, and the medial collateral ligament (MCL).
Even when the injuries don’t occur as part of the full triad, ACL tears and meniscal tears are frequently combined, especially in contact sports or high-speed movements. Understanding how these injuries happen — and how they differ — can help guide diagnosis, treatment, and rehabilitation.
Meniscal Tear: Twisting Under Load
Meniscal tears often occur when the knee is twisted while bearing weight — for example, planting the foot and rotating the upper body. This is common in sports like football, basketball, or tennis, but can also happen when getting up awkwardly from a squat or turning suddenly during daily activities.
Meniscus injuries can result from:
- Sudden trauma, especially in younger, active people
- Repetitive stress or degeneration, especially in older adults
In older individuals, meniscal tears often occur without a clear traumatic event and may develop gradually as the cartilage wears down.
ACL Tear: Sudden Stop or Change in Direction
ACL injuries typically result from a sudden change in direction, pivoting, or an awkward landing — usually without direct contact. They often happen during high-intensity sports like soccer, skiing, or basketball, but also from accidents like car accidents.
Typical mechanisms include:
- Landing from a jump with the knee slightly bent and twisted
- Rapid deceleration or cutting to change direction
- Direct blow to the knee in sport or car accident
Understanding how each injury occurs is key to early recognition — and often provides the first clue for accurate diagnosis.
| Injury Type | Typical Mechanism | Common Scenario |
|---|---|---|
| Meniscal Tear | Twisting or rotating the knee while bearing weight | Pivoting on a planted foot, deep squatting, or kneeling with rotation |
| ACL Tear | Sudden deceleration, pivoting, or awkward landing | Quick change of direction during running or landing from a jump |
| Combined Injury (Unhappy Triad) | Force applied to the outer knee with foot planted | Contact injury (e.g., football tackle) causing damage to ACL, meniscus, and MCL |
Meniscal Tear vs ACL Tear Symptoms: What Do You Feel?
Although both injuries affect the knee and share some overlapping symptoms, such as pain and swelling, there are also key differences that can help distinguish one from the other. Recognizing these similarities and differences is important for early diagnosis and choosing the right treatment path.
Below is a comparison of the most common symptoms associated with each type of injury:
Meniscal Tear Symptoms
- Pain on either the inner (medial) or outer (lateral) side of the knee, depending on which meniscus is torn
- Swelling that develops gradually over several hours or even days
- Locking or catching sensation when trying to bend or straighten the knee
- A feeling of the knee “giving way” in certain positions, especially during twisting movements
- Limited range of motion, especially difficulty fully extending the knee
- Symptoms may be mild at first and worsen with continued activity
- Can occur without a clear injury, especially in degenerative cases
ACL Tear Symptoms
- A loud “pop” at the moment of injury
- Immediate pain and an inability to continue activity
- Rapid and significant swelling within 1–2 hours
- Instability or buckling of the knee when trying to stand or walk
- Feeling like the knee is “slipping out of place”
- Often associated with a sense of sudden collapse during sports
- Pain may improve quickly, but instability remains
When Both Are Injured
In combined injuries (like the “unhappy triad”), symptoms often overlap: swelling is fast and severe, the knee feels unstable, and there may be locking or catching. These cases require thorough clinical evaluation and imaging for an accurate diagnosis.
| Symptom | Meniscal Tear | ACL Tear |
|---|---|---|
| Onset | May be gradual or sudden, especially with twisting injury | Usually sudden with a “popping” sound or sensation |
| Swelling | Develops slowly (over 24–48 hours) | Appears quickly, often within a few hours |
| Pain Location | Localized along joint line (medial or lateral side) | Diffuse pain around the entire knee |
| Locking or Catching | Common — knee may catch, lock, or feel like it’s “sticking” | Rare — may feel unstable rather than locking |
| Instability | Knee may feel unstable during specific movements | Frequent — knee may “give out” during walking or pivoting |
| Range of Motion | May be limited due to pain or mechanical block | Usually reduced immediately due to swelling and instability |
Meniscal Tear vs ACL Tear: Differences in Healing Potential
The healing potential of a meniscal tear and an ACL (anterior cruciate ligament) tear varies significantly — mainly due to differences in blood supply, tissue type, and injury location.
Meniscal Tear Healing
Not all meniscal tears are the same, and whether or not they can heal on their own depends heavily on the location and type of tear.
The outer third of the meniscus (known as the “red zone”) has a rich blood supply, which allows some tears in this area — particularly small, longitudinal tears — to heal naturally or respond well to conservative treatment like physical therapy.
About 60-70% of meniscal tears can heal completely on its own without surgery.
However, tears located in the inner two-thirds (the “white zone”) have very limited blood flow, making spontaneous healing unlikely — especially in the case of degenerative or complex tears.
ACL Tear Healing
Unlike the meniscus, the ACL is a ligament, not cartilage — and it does not heal on its own once completely torn. The ACL has a poor blood supply and, when ruptured, the two torn ends tend to retract and scar, preventing natural reconnection.
Partial ACL injuries may sometimes be managed without surgery, especially in less active individuals. But for complete ACL ruptures, particularly in athletes or younger, active individuals — surgical reconstruction is often required to restore knee stability. Without proper treatment, further damage can occur to other joint structures, including the meniscus.
Key Difference
In summary, while some meniscal tears may heal with rest and rehabilitation, ACL tears typically do not, especially if full-thickness.
Meniscal Tear vs ACL Tear: Treatment Options
While both meniscal and ACL tears affect the knee and may occur through similar injury mechanisms, the treatment approach for each can differ significantly. Choosing the right treatment depends on factors such as the type and severity of the tear, the patient’s age, activity level, and overall joint health. Below is a breakdown of how treatment typically differs between these two common knee injuries.
Conservative (Non-Surgical) Treatment
Meniscal Tear
- Often the first line of treatment, especially for smaller tears or degenerative changes.
- Includes rest, ice, compression, elevation (RICE), anti-inflammatory medications, and physical therapy.
- Effective for stable tears, especially in the outer (vascular) zone.
- Many patients recover without surgery, particularly older or less active individuals.
ACL Tear
- Partial tears may sometimes be managed conservatively with physical therapy and activity modification.
- Conservative treatment may be appropriate for older or less active patients.
- Complete tears rarely heal without surgery and often lead to ongoing instability.
Surgical Treatment
Meniscal Tear
- Surgery may be required if the tear causes mechanical symptoms like locking or persistent pain.
- Surgical options include:
- Meniscectomy: removal of the damaged part of the meniscus.
- Meniscal repair: suturing the tear, often used in younger patients with tears in the red zone.
- Meniscal transplant: considered in select cases with previous total meniscectomy and ongoing symptoms.
ACL Tear
- Surgical reconstruction is the standard treatment for complete ACL ruptures in active individuals.
- Involves replacing the torn ligament with a graft (often from the patellar tendon, hamstring, or donor tissue).
- Helps restore knee stability and reduces the risk of further injury to the meniscus and cartilage.
Rehabilitation
Meniscal Tear
- Physical therapy focuses on restoring knee strength, mobility, and function.
- Recovery time depends on whether the meniscus was repaired or removed:
- After meniscectomy: patients may return to activity within 4–6 weeks.
- After repair: healing takes longer — typically 3–6 months.
ACL Tear
- Rehabilitation is longer and more intensive.
- Return to sports typically takes 6–9 months post-surgery, depending on progress.
- Physical therapy is critical for restoring strength, coordination, and joint control.
Summary
- Meniscal tears can often be treated conservatively and may heal on their own depending on the tear type and location.
- ACL tears, particularly complete ruptures, usually require surgical reconstruction to restore joint stability and prevent further damage.
- Rehabilitation plays a central role in the recovery of both injuries, but recovery time and intensity differ significantly.
Meniscal Tear vs ACL Tear: Recovery Timeline and Rehabilitation
Although both injuries affect the knee, the recovery process — including rehabilitation and return to activity — varies significantly between meniscal and ACL tears.
Recovery Duration
Meniscal Tear
- Recovery time depends on whether the tear is treated conservatively or surgically.
- After a partial meniscectomy, most patients resume normal activities within 4–6 weeks.
- After meniscus repair, recovery is longer — typically 3–6 months to allow proper healing of the stitched tissue.
- Degenerative tears managed without surgery may improve within 6–8 weeks of physical therapy.
ACL Tear
- Full recovery from ACL reconstruction surgery usually takes 6–9 months, with return to high-level sports often delayed up to a year.
- Recovery from non-surgical management (in select cases) varies widely and often includes long-term activity modification.
Rehabilitation Process
Meniscal Tear Rehab
- Focuses on reducing swelling, restoring range of motion, and gradually rebuilding strength — particularly in the quadriceps and hamstrings.
- Low-impact exercises such as cycling and swimming are commonly introduced early.
- After repair, weight-bearing may be restricted in the early phase to protect the sutured tissue.
ACL Tear Rehab
- Rehab is longer and more structured, often divided into phases.
- Early goals: control swelling, regain extension, and activate the quadriceps.
- Later phases include neuromuscular training, proprioception, and sport-specific drills.
- A return-to-sport assessment is essential before resuming full athletic activity.
Return to Sport or Activity
| Injury Type | Light Activity | Full Activity | Competitive Sports |
|---|---|---|---|
| Meniscal Tear (Meniscectomy) | 2–4 weeks | 4–6 weeks | 6–8 weeks |
| Meniscal Tear (Repair) | 6–8 weeks | 3–4 months | 4–6 months |
| ACL Reconstruction | 3–4 months | 6–9 months | 9–12 months |
Prognosis and Long-Term Outlook
The long-term outcome after a meniscal tear or ACL injury depends on several key factors: the type and severity of the injury, the treatment approach, and how consistently rehabilitation is followed.
Meniscal tears generally have a good prognosis when located in the outer, well-vascularized zone of the meniscus — particularly if the tear is vertical and stable. These injuries may heal on their own or respond well to surgical repair. On the other hand, tears in the inner, avascular region or those associated with degeneration tend to have limited healing capacity and may require partial removal of the damaged tissue. Although this can relieve symptoms, removing meniscal tissue increases stress on the joint surfaces, which may lead to cartilage wear and osteoarthritis over time.
ACL tears have a more complex recovery path, especially when fully ruptured. In younger or physically active individuals, surgical reconstruction is often recommended to restore knee stability and protect other joint structures. With a well-structured rehabilitation program, most people can return to everyday activities within several months, and many athletes return to their sports within 6 to 12 months. However, full recovery is not guaranteed for everyone — some may experience reduced performance, lingering instability, or fear of re-injury.
Both meniscal and ACL injuries carry a risk of long-term joint degeneration, particularly if left untreated or if associated with other damage. That’s why early diagnosis, careful treatment planning, and patient adherence to rehab are essential in achieving the best possible outcome.
Key Takeaways
- Meniscal tears vary widely; some heal on their own, while others may require surgery.
- ACL tears, especially full ruptures, typically need surgical reconstruction in active individuals.
- Symptoms may overlap, but ACL injuries often involve more swelling, instability, and a “popping” sensation.
- Recovery timelines differ, but both conditions require patience and commitment to rehab.
- Long-term joint health depends on early treatment, accurate diagnosis, and protecting the joint from further injury.
Raj MA, Bubnis MA. Knee Meniscal Tears. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431067/
Luvsannyam E, Jain MS, Leitao AR, Maikawa N, Leitao AE. Meniscus Tear: Pathology, Incidence, and Management. Cureus. 2022 May 18;14(5):e25121. doi: 10.7759/cureus.25121. PMID: 35733484; PMCID: PMC9205760.
Evans J, Mabrouk A, Nielson Jl. Anterior Cruciate Ligament Knee Injury. [Updated 2023 Nov 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499848/
Shom P, Varma AR, Prasad R. The Anterior Cruciate Ligament: Principles of Treatment. Cureus. 2023 Jun 11;15(6):e40269. doi: 10.7759/cureus.40269. PMID: 37448400; PMCID: PMC10336184.

















